
Abstract
Abstract
Background:
Little is known about state-level variation in patterns of hospice use, an important indicator of quality of care at the end of life. Findings may identify states where targeted efforts for improving end-of-life care may be warranted.
Objective:
Our aim was to characterize the state-level variation in patterns of hospice use among decedents and to examine state, county, and individual factors associated with these patterns.
Methods:
We conducted a retrospective analysis of Medicare fee-for-service decedents. The primary outcome measures were state-level hospice use during the last 6 months of life and the state's proportion of hospice users with very short hospice enrollment (≤7 days), very long hospice enrollment (≥180 days), and hospice disenrollment prior to death.
Results:
In 2011, the percentage of decedents who used hospice in the last 6 months of life nationally was 47.1%, and varied across states from 20.3% in Alaska to 60.8% in Utah. Hospice utilization patterns also varied by state, with the percentage of hospice users with very short hospice enrollment ranging from 23.0% in the District of Columbia to 39.9% in Connecticut. The percentage of very long hospice use varied from 5.7% in Connecticut to 15.9% in Delaware. The percentage of hospice disenrollment ranged from 6.2% in Hawaii to 19.0% in the District of Columbia. Nationally, state-level hospice use among decedents was positively correlated with the percentage of potentially concerning patterns (including very short hospice enrollment, very long hospice enrollment, and hospice disenrollment) among hospice users (the Pearson correlation coefficient=0.52, p value<0.001). Oregon was the only state in the highest quartile of hospice use and the lowest quartiles of both very short and very long hospice enrollment.
Conclusions:
The percentage of decedents who use hospice may mask important state-level variation in these patterns, including the timing of hospice enrollment, a potentially important component of the quality of end-of-life care.
Introduction
H
Prior literature has shown considerable state-level variation in the proportion of decedents who enroll in hospice.14,15 Data from 2002 indicated that the use of hospice varied from 8% to 49% across states. 14 Although these reports are informative, they are based on data that are more than a decade old, and they did not report more detailed information regarding state-level variation in patterns of hospice utilization such as very short hospice enrollment, very long hospice enrollment, or hospice disenrollment. Understanding state-level variation in both the overall hospice use and utilization patterns simultaneously may help identify geographies that, despite high hospice use, may have concerning patterns of use. As hospice provisions were recently added to the Improving Medicare Post-Acute Care Transformation Act of 2014 (IMPACT Act), 16 efforts to examine the patterns of hospice use would provide important insight and improve hospice care.
Accordingly, we sought to investigate state-level variation in patterns of hospice use. We identified states with particularly high use of hospice and low proportions of very short or very long hospice enrollment and less frequent disenrollment from hospice. Additionally, we identified the patient-, county-, and state-level factors that were associated with increased likelihood of hospice use and varying patterns of hospice use separately. Findings from this study can provide a more complete picture of geographic variation in the quality of end-of-life care across the United States.
Methods
Study design and sample
We conducted a retrospective analysis of all fee-for-service Medicare beneficiaries older than 66 years who died between July 1, 2011, and December 31, 2011. We retrieved their demographics and chronic conditions from the Master Beneficiary Summary File, as well as hospice Medicare claims in the 6 months prior to death. We limited our sample to beneficiaries who had been enrolled in Medicare Parts A and B in the last 6 months before death. Within this full sample, we further identified beneficiaries who had been enrolled in hospice programs as the second sample. The study was reviewed by the institutional review board of Yale University and was exempt from full review.
Measurement
Outcomes
The primary outcomes of interest were a set of binary variables to indicate use of hospice, as well as patterns of hospice use. For the subset of decedents who enrolled with hospice, we created three binary measures to indicate very short hospice enrollment (enrollment ≤7 days), very long hospice enrollment (enrollment≥ 180 days),and hospice disenrollment. For people who were enrolled with hospice more than one time during the last 6 months of life, we calculated total days of hospice enrollment across all hospice enrollment periods. Very short hospice enrollment had to be ≤7 days of enrollment and the last hospice enrollment was initiated ≤7 days prior death. We identified individuals as having disenrollment from hospice if: (1) they had more than one hospice enrollment period, or (2) they had only one hospice enrollment period and the date of discharge differed from the date of death. We used the term potentially concerning to refer to patterns of hospice use with very short or very long hospice enrollment or hospice disenrollment.
Covariates
We included as candidate covariates patient age (categorized as 66–69 years, 70–74 years, 75–79 years, 80–84 years, and ≥85 years), race/ethnicity (non-Hispanic white, black, Hispanic, and other), and gender. We ascertained chronic conditions using data from the Master Beneficiary Summary File including heart disease (acute myocardial infarction, heart failure, and ischemic heart disease), Alzheimer's disease or dementia, kidney disease, diabetes, chronic obstructive pulmonary disease or asthma, depression, stroke, and cancer (breast, colorectal, prostate, lung, and endometrial). In addition, we used zip code information to identify the residence of county and hospital referral region (HRR) for each beneficiary. We then used data pertaining to the county in which the patient resided using the Area Resource File, which included median county-level income and percentage of adults in the county with a high school education or less, the percentage of individuals in health maintenance organizations (HMOs) in the county, and the number of physicians, hospital beds, skilled nursing facility beds, hospices, and home health agencies per 1000 people aged 65 and older in the county. We also included state-level factors from 2011, including whether hospice was regulated by Certificate of Need (CON) 17 and the percentage of hospitals reporting palliative care services (categorized as ≤20%, 21–40%, 41–60%, 61–80%, and ≥80%). 18
Statistical analysis
We applied standard frequency analysis to describe the full sample by demographic, clinical, and social factors by hospice use with χ2 statistics. We determined the proportion of decedents who used hospice and mapped the states by quartiles of use. We performed the same analysis to classify hospice use according to patterns of use (i.e., very short enrollment, very long enrollment, or disenrollment) with the number of decedents who used hospice in each state as the denominator. Correlations across state-level measures were tested using the Pearson correlation coefficient.
In the multivariable analyses, we used sequential logistic regression models to determine the independent contribution of individual and market factors to overall hospice use. We estimated three-level hierarchical generalized linear models (HGLMs), and we also adjusted for patient-, county-, and state-level characteristics and clustering of patients by HRR and state to identify independent correlates of overall hospice use. Discrimination was measured using the C statistic, and the proportion of explained variation was measured by the sums-of-squares between observed and predicted outcomes. 19 We assessed the variation at the HRR and state levels using the covariance estimate at each level, derived from the random effect of HGLMs. We calculated the absolute percentage deviation for each state, the difference between the predicted and the actual proportions of hospice use divided by the actual proportion of hospice use. We performed the same multivariable analysis classifying hospice use as potentially concerning use. We included nonhospice users and hospice users with potentially concerning patterns of use when we estimated the independent associations between individual/market factors and potentially concerning hospice use. All statistical analyses were complete dusing SAS software, version 9.3 (SAS Institute, Cary, NC), and a two-tailed p value<0.05 was used to define statistical significance.
Results
The full study sample consisted of 660,132 decedents enrolled in fee-for-service Medicare during the last 6 months of life. A total of 47% of them had been enrolled in hospice programs. The mean age at death was 82.6 years, whereas 44.9% were 85 years or older at the time of death. Among the cohort, 54.9% were recorded as female and 84.6% were recorded as non-Hispanic white. Characteristics of decedents who were and were not enrolled in a hospice program were summarized in Table 1. A total of 49.7% of hospice users had potentially concerning patterns of hospice use; that is, they used hospice for either longer than 180 days or less than 7 days or were disenrolled prior to death (9.9%, 32.4%, and 8.5%, respectively).
Hospice use differed substantially across states (Table 2). The mean proportion of decedents in a state who used hospice was 45.9%, ranging from 20.2% in Alaska to 60.8% in Utah. Furthermore, the proportion of hospice users with potentially concerning patterns of hospice use (that is, very short, very long, or disenrollment) also varied markedly across states, ranging from 38.8% in Vermont to 56.0% in Rhode Island. The percentage of very short hospice enrollment varied from 23% in the District of Columbia to 39.9% of hospice users in Connecticut, and the percentage of very long hospice use varied from 5.7% in Connecticut to 15.9% of hospice users in Delaware. The percentage of hospice disenrollment varied from 6.2% in Hawaii to 19% of hospice users in the District of Columbia.
The unit of analysis is state (each value represented the mean of state means).
Potentially concerning hospice use included very short hospice enrollment, very long hospice enrollment, or hospice disenrollment.
SD, standard deviation.
Across states, the proportion of decedents who used hospice was positively associated with the proportion who had potentially concerning patterns of use (rho=0.52, p value<0.001; Fig. 1). Although Arizona, Delaware, Florida, and Rhode Island had relatively high overall hospice use, they were also the states with the highest proportion of hospice users with concerning patterns of use. In contrast, although Alaska, North Dakota, and Vermont had relatively low hospice use, they also had a lower proportion of hospice users with potentially concerning patterns of use. We found only one state, Oregon, that was in the highest quartile of overall hospice use and the lowest quartile for potentially concerning patterns of hospice use.
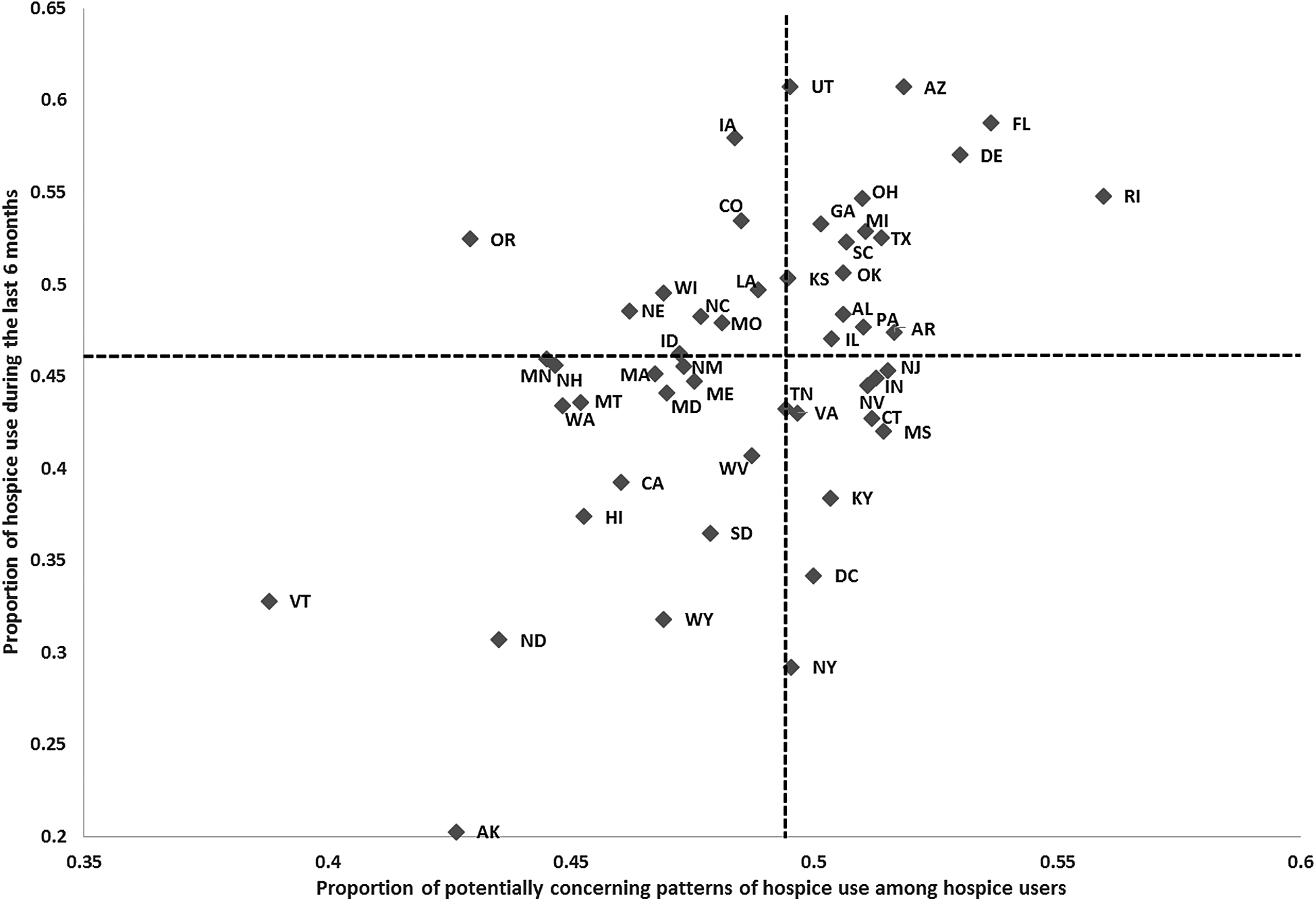
Hospice use among decedents and potentially concerning patterns of hospice use across states. (Pearson correlation coefficient=0.516, p<0.001. Dash lines indicate median values.)
Among hospice users, proportions of very short hospice enrollment, very long hospice referral, or hospice disenrollment varied across states (Fig. 2). The proportion of hospice users with very long hospice enrollment was positively correlated (rho=0.42, p value=0.002) with the proportion of hospice users with hospice disenrollment and negatively correlated (rho=–0.50, p value<0.001) with the proportion of hospice users with very short hospice enrollment. Vermont was in the lowest quartile of all three potentially concerning patterns of hospice use. We did not find any state that was in the highest quartile in all three measures.

Quartiles of potentially concerning patterns of hospice use across states (lighter color signifies higher quartile).
In the multivariable analyses, we found that older adults, females, adults with reported race of white, and adults residing in metropolitan areas, areas with higher income, and areas with higher education were more likely to use hospice (Table 3). Furthermore, Medicare decedents who had dementia, kidney disease, depression, stroke, or cancer were more likely to be enrolled in a hospice program than those who did not have these diseases, whereas decedents who had heart disease or diabetes were less likely to be enrolled in a hospice program compared with those who did not have heart disease or diabetes. Decedents in areas that had a higher HMO penetration rate, a greater number of hospices per 1000 people, and more physicians per 1000 people aged 65years or older were more likely to use hospice. Decedents in the areas that had more hospital beds and more home health agencies per 1000 people aged 65 or older were less likely to use hospice. Neither the presence of CON regulations nor access to hospital-based palliative care was associated with use of hospice. The mean absolute percent deviation of the proportion of hospice use across state was 0.3%, ranging from 0% to 3.6%. The demographic, social, clinical, and market factors generally had similar impact on overall hospice use and potentially concerning patterns of hospice use (Table 3). Furthermore, HRRs with greater HMO penetration, more hospice programs, and more physicians were more likely to have very long and very short hospice enrollments (data not shown).
p<0.05; ** p<0.01; *** p<0.001; Numbers in bold indicate P-value at the 0.05 level.
Controlled for age, sex, race/ethnicity, chronic conditions, metro residence, education, incomes, and county- and state-level covariates; clustered by hospital referral region (HRR) and state.
All decedents.
Decedents who did not use hospice or had potentially concerning patterns of hospice use (who had very short or very long enrollment or who were disenrolled).
Controlled for age, sex, race/ethnicity, chronic conditions, metro residence, education, and incomes.
CI, confidence interval; OR, odds ratio; HGLM, hierarchical generalized linear model, HS, high school.
Discussion
Using comprehensive national data, our study provides more detailed estimates of hospice utilization across the state than have been previously published. We found approximately 45% of the decedents used hospice and that nearly 50% of this hospice use reflected potentially concerning patterns, including very short or very long enrollment times or hospice disenrollment. State-level variation in the prevalence of potentially concerning patterns of hospice use was substantial. Although hospice use has been used as a quality indicator for end-of-life care, our findings suggest that examining only the percentage of decedents who use hospice may mask important aspects of care at the end of life.
Our assessment regarding appropriateness of hospice use represents a new approach to assessing the quality of end-of-life care. Previous work evaluating variation of hospice use generally assessed the quantity of hospice use across states.14,15 Recent work has started examining very short and very long enrollments as well as hospice disenrollment6,13; however, no previous study has documented geographic distribution of potentially concerning patterns of hospice use by state. Importantly, even among states with high hospice use, some have substantial portions of this use that is potentially concerning in its pattern, providing greater nuance in our understanding of geographic variation in end-of-life care.
Although there is no consensus about appropriateness for hospice use, Earle and colleagues have identified very short hospice enrollment for patients with advanced cancer as an indicator of problematic hospice use, 1 a conclusion that has also been endorsed by the National Quality Forum. 3 In other studies, very short length of hospice enrollment has been linked to fewer hospice services received, increased unmet need, and clinical depression among surviving family caregivers.9,11 If providers continue intensive care unit (ICU)-level care and discharge patients to nearby hospices at the very end of life, such short hospice enrollments may result.20,21 Additionally, given the current per diem payment for hospice, policymakers and researchers have concerns about very long hospice enrollment, as the dramatic increase of Medicare spending for hospice care was partially driven by longer stays among hospice patients with the longest stays.8,22 Under the IMPACT Act of 2014, higher percentages of hospice patients receiving care for more than 180 days trigger medial review by the Centers for Medicare & Medicaid Services. Instead of stopping payment to hospices for patients with a very long stay, this policy change implies the necessity of clinical jurisdiction, accounting for patient demographics and disease characteristics. For example, previous research has found that patients residing in nursing homes prior to hospice enrollment and having dementia are more likely to have very long stays. 23 Last, although hospice disenrollment to attain acute care support after hospice enrollment may be preferred by patients and family in certain cases, financial incentives may lead hospices to inappropriately use disenrollment to avoid costly hospital-based services.13,24 In this study, we confirm recent work finding that approximately half of all hospice use reflects at least one of these potentially concerning patterns of care, 5 and demonstrate that these utilization patterns persist at the state level. The variation in these patterns across states was unexpected and warrants further examination in future studies.
The implications of our findings are several. First, our results underscore the importance of assessing not only the proportion of decedents who use hospice but also the patterns of hospice use, recognizing the substantial magnitude of state-level variation in the United States. Of note, Oregon was in the highest quartile of hospice use as well as in the lowest quartile of potentially concerning pattern of hospice use. As Oregon follows federal hospice regulation without additional state-specific legislation governing hospice, 25 it is possible that the Oregon Death with Dignity Act 26 has resulted in or at least reflects more open conversation and careful evaluation of end-of-life options, more appropriate palliative care training of physicians, and more efforts to reduce barriers to access to hospice care and has thus increased hospice referrals and reduced potentially concerning patterns of hospice use in the state.27–29 Second, our findings suggest that health care resources are associated with both overall use and potentially concerning patterns of hospice use. Decedents living in areas with higher HMO penetration, more hospice programs, and more physicians were more likely to have higher overall use and potentially concerning patterns of hospice use. These findings indicate that improvement in overall hospice use by reallocation of health care resources may come at the expense of increased potentially concerning patterns of hospice use. Future studies examining state-specific policies and resources in relation to patterns of hospice use could help determine which strategies can minimize potentially concerning patterns of hospice use. Last, it is not surprising to see a negative correlation between proportions of very short and very long hospice use across states. These findings indicate that the quality of hospice use should be based on a set of indicators, rather a single measure. Benchmarking efforts in hospice quality improvement may need to focus on several performance measures simultaneously. Future research is warranted to construct a quality measure metric to assess quality of hospice use.
Our findings should be interpreted in light of several limitations. This was a descriptive, exploratory study, and due to the cross-sectional nature of our data, we could not draw causal inferences. The associations between hospice characteristics and survival is out of the scope of this study, and future research in this area may be warranted. Furthermore, although we measured the prevalence of various chronic diseases, we did not have data on the severity of disease or the cause of death, both of which may be important correlates of hospice use and the patterns of use. Last, we lacked data on patient preferences, which might have enabled us to better interpret various patterns of hospice care. Nevertheless, patient preferences are unlikely to explain the systematic differences in hospice use we found across states.
In conclusion, we provided contemporary data on state-level variation in use of hospice, patterns of hospice use, and identified relevant demographic, clinical, and market factor correlates. Although increasing proportions of decedents are using hospice, some states have a preponderance of potentially concerning patterns of hospice use. Our findings highlight the importance of considering not only use of hospice but also patterns of its use when assessing the quality of care at the end of life.
Footnotes
Acknowledgments
This study was supported by grant 1R01CA116398-01A2 from the National Cancer Institute (Drs. Aldridge and Bradley), the John D. Thompson Foundation (Dr. Bradley), and grant 5R01NR013499 from the National Institute of Nursing Research (Dr. Aldridge).
The sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author contributions: Dr. Wang had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Wang, Aldridge, Gross, Canavan, Cherlin, Bradley. Acquisition of data: Bradley. Analysis and interpretation of data: Wang, Aldridge, Gross, Canavan, Cherlin, Hürzeler, Bradley. Drafting of the manuscript: Wang, Aldridge, Gross, Bradley. Critical revision of the manuscript for important intellectual content: Wang, Aldridge, Gross, Canavan, Cherlin, Hürzeler, Bradley. Statistical analysis: Wang. Obtained funding: Aldridge, Bradley. Administrative, technical, and material support: Canavan, Cherlin, Hürzeler. Study supervision: Wang, Aldridge, Gross, Bradley.
Author Disclosure Statement
Dr. Gross receives support from Medtronic, Inc., Johnson & Johnson, Inc., and 21st Century Oncology. Dr. Gross is also a member of a scientific advisory board for FAIR Health, Inc. These sources of support were not used for any portion of the current study. None of the other coauthors have conflicts to report.