
Abstract
Abstract
Background:
Survey research indicates that decisions about the provision and limitation of treatment near the end of life in patients with cancer vary considerably.
Objectives:
The study objectives were to review the evidence on variables associated with explicit decisions about limitation of treatment in patients with cancer and to critically appraise the factors from a clinical ethics perspective.
Methods:
A search was conducted of studies published in EMBASE, CINAHL, PsycINFO, Assia, Current Contents Medicine, Belit, and Euroethics before February 5, 2014. Eligible studies reported data on explicit treatment limitation in patients with cancer and included a statistical analysis on possibly associated factors. Information on study participants, types of limited treatment, and variables associated with limiting treatment were extracted by two researchers independently. Data synthesis was performed jointly by researchers from oncology, medical ethics, and social sciences.
Results:
The search yielded 897 publications, of which 7 were relevant for this review. Factors significantly associated with decisions about limitation of treatment could be distinguished in three categories: first, sociodemographic variables such as the ethnic background of patients; second, health- or treatment-related variables including a lack of capacity in patients with cancer; and third, patients' preferences and the role of relatives in decisions about limitation of treatment. Limitations to this study are that the studies lacked a predefined hypothesis and they all had been conducted in Western countries.
Conclusion:
The identified variables raise ethical issues with regards to possible influence of value judgments underlying decisions about limitation of treatment in end-of-life care.
Introduction
W
The factors that are relevant to decisions about the limitation of treatment at the end of life have been explored in conceptual10–13 as well as empirical research.14,15 Empirical research suggests that physicians' values14,15 and the degree of communication between patients and physicians 16 influence decisions in cancer care. In addition, concordance or discordance of views regarding appropriate treatment is associated with different communication about treatment decisions between patients and physicians. 17 However, to the best of our knowledge, so far there has not been conducted a systematic review on the available evidence on factors associated with explicit limitation of treatment in cancer care. Such research can inform professional decision making by providing information on factors that should be looked at as potential source of bias when making decisions. Furthermore, data about variables associated with decisions about treatment limitation can inform the design and implementation of clinical ethics support services to support decision making near the end of life.
In this study we present findings from a systematic review of studies that have analyzed variables associated with explicit decisions to limit treatment in patients with cancer. In order to assess whether explicit decision making about treatment limitation in end-of-life care for patients with cancer raises ethical concerns, we will discuss the empirical findings in the light of relevant concepts of ethics and medical professionalism.
Methods
Search strategy
We conducted a systematic search of studies published in English or German in PubMed, EMBASE, CINAHL, PsycINFO, Assia, Current Contents Medicine, Belit, and Euroethics from their inception until February 5, 2014. In line with recommendations issued in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 18 and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) 19 guidelines, the search terms were identified from keyword lists of relevant publications and amended following an interdisciplinary exchange between the authors and professionals in medical ethics and oncology. Supplementary table 1 shows the search algorithm used for PubMed (the search algorithms for other databases can be obtained from the first author). (See online supplementary material at www.liebertpub.com/jpm and at www.liebertonline.com.)
Study selection and definition
A total of 897 references resulted from the systematic search after duplicates had been removed. The first author and one more researcher (AB, MC, or SS) categorized the articles based on title and abstract as possibly eligible or ineligible in light of the review question, “Which variables are associated with explicit decisions about treatment limitation in patients with cancer at the end of life?” For definite inclusion, eligible studies had to report results from a clinical trial, cohort study, or survey, including the findings of a statistical analysis of variables associated with explicit decision making about limitation of medical treatment in patients with cancer.
Following careful multidisciplinary analysis of the concept of “limitation of treatment,” we encountered a number of situations that differ with regards to clinical and ethical relevant aspects. This is due to different notions of what consists of “treatment,” for example with regards to nutrition or hydration and also due to differing concepts of “limitation.” It should be emphasized that according to the clinical experience of the authors, patients near the end of life usually are treated although there may be “nontreatment decisions” with regards to particular measures. Against the background of differing notions of the term we decided not to provide a definition but to follow the concepts of the authors. This means that the use of the term in this publication encompasses a range of different cases. However, studies were not considered eligible that reported implicit decisions about limitation, as with introduction of a palliative care intervention, often associated with increasing symptom treatment and limiting cancer-specific treatment.
Qualitative studies and surveys including hypothetical scenarios were excluded for methodological reasons. The most common reason for exclusion of articles was that papers reported factors associated with implicit decisions about limitation of treatment but not with explicit decisions as described above. The full text of possibly eligible articles was searched and read by the first author and one more author (AB or MC). Disagreement between the researchers was discussed until consensus was reached. Reference lists of eligible articles were reviewed for further eligible studies according to the procedure described above. Figure 1 provides an overview of the study selection process.
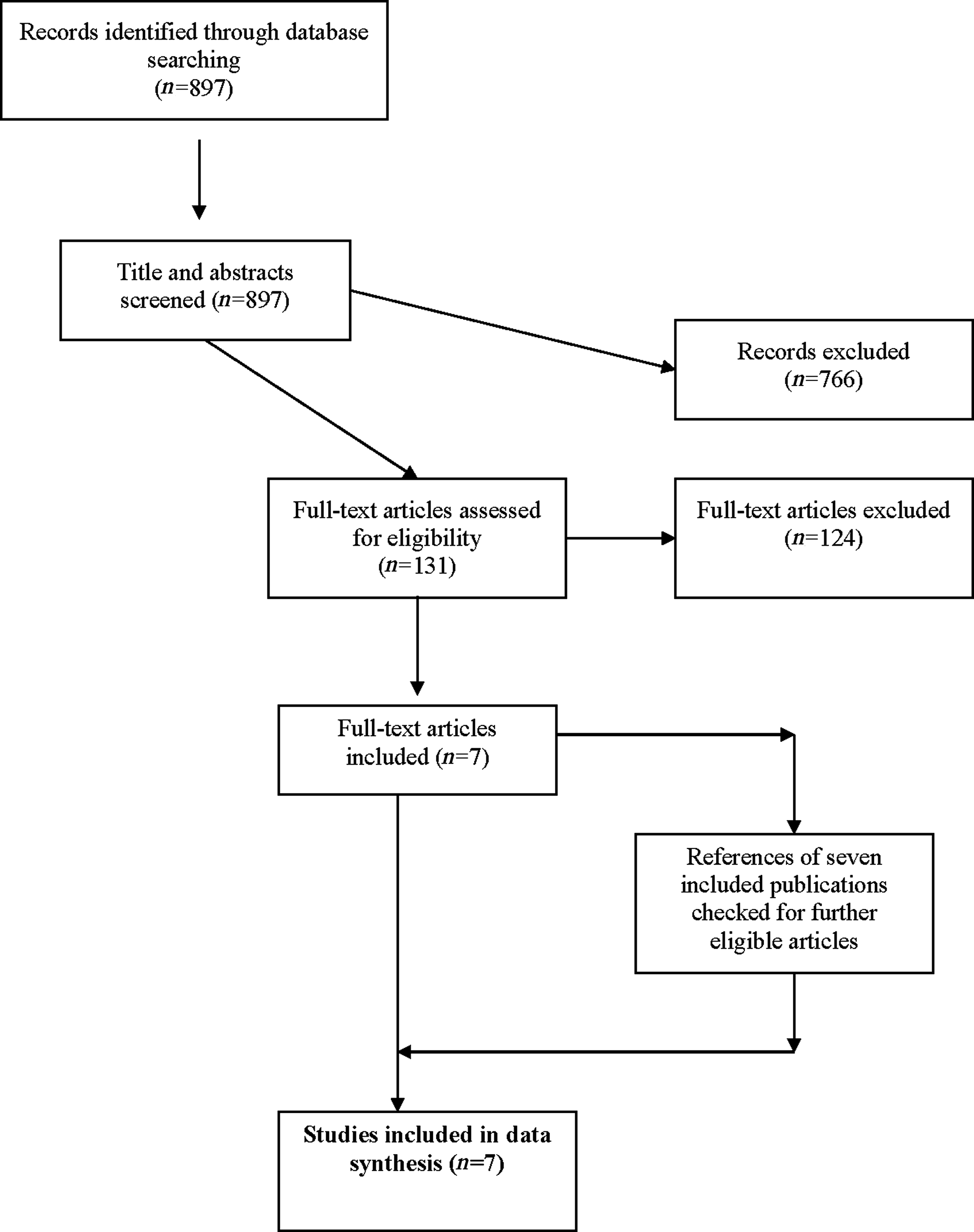
Flowchart of literature search.
Quality assessment and data synthesis
Each study included was assessed by two authors (JS, AB) against the methodological quality criteria defined by the Scottish Intercollegiate Guidelines Network (SIGN). 20 Use of the SIGN tool was in line with the specific content of studies investigating factors associated with limitation of treatment rather than usual cohort studies assessing associations with certain clinical outcomes. Table 1 summarizes the selected SIGN criteria and the results for each study.
SIGN, Scottish Intercollegiate Guidelines Network.
Data from the studies included were extracted independently by two authors (JS and MC). Data abstraction included the country in which the study was performed, research design, patient population, respondents and response rate, treatment that was limited, and variables tested for significance regarding their association with limitation of treatment (see Table 2). Initial data extraction was compared between the two authors and discussed in the case of divergences until consensus was reached. In a subsequent step, data extraction was checked by a third author (SS) against the data reported in the original paper and against the aim of this review. We tabulated the findings associated with treatment limitation. Due to the heterogeneity of research design and the variables analyzed within the sample of the seven studies included, we decided against statistical meta-analysis and instead provide a detailed narrative analysis of the studies in accordance with relevant sections of the PRISMA checklist 18 (see Supplementary table 2) (See online supplementary material at www.liebertpub.com/jpm and at www.liebertonline.com.)
Results
Study characteristics and quality
Our systematic review identified seven publications that provide information about factors significantly associated with limitation of treatment in patients with cancer.21–27 The first study was published in 1994 21 and four studies were published in 2009 or later.23–25,27 Four studies were conducted in the United States21–23,25 and the other studies were conducted in Canada, 24 Japan, 26 and The Netherlands. 27 Three studies had a prospective research design.21,25,26 Methods for data gathering most frequently included medical chart;21–25 in the two other studies data stem from structured questionnaires directed to physicians26,27 or relatives of patients with cancer. 27 The studies included reported data on a minimum of 118 patients 24 and a maximum of 417 patients. 22 All studies reported data on different types of cancer, except for the study of Brown et al., which included only patients with pancreatic cancer. 22
Variables associated with treatment limitation
Five studies reported analyses of associations between decisions about the limitation of treatment and sociodemographic and contextual factors.22–25,27 Four studies reported such analyses with regard to patients' health- or treatment-related aspects as factors influencing decisions about limiting treatment.21,22,24,26 Three studies investigated patients' preferences, end-of-life communication, and the role of relatives as variables possibly associated with treatment limitation.22,26,27 Table 2 provides a brief summary of each study. Selected findings of data excerption are described below for each of these three categories.
Sociodemographic and contextual variables
Sociodemographic and other contextual factors were most frequently analyzed as variables possibly associated with treatment limitation in our study sample. There were three studies conducted in the United States that investigated the role of ethnicity as a variable in decisions about treatment limitation.22,23,25 According to a study by Cesta et al. 23 there was significantly more withdrawal of life supportive therapy such as vasopressor or respiratory support in white patients with cancer who died in the intensive care unit compared to patients from other ethnic groups. In addition, Mack et al. 25 reported in their study that white patients who had a do-not-resuscitate (DNR) order, who reported end-of-life communication, or who were aware of the terminal situation were statistically significantly less likely to receive life-prolonging care (i.e., use of mechanical ventilation, resuscitation, or intensive care unit hospitalization) during the last weeks of life than other white patients; whereas this was not the case for the group of black patients.
In a study conducted by Brown et al. on patients with pancreatic cancer, statistical analysis indicates that white dehydrated patients received significantly less hydration than dehydrated patients from other ethnic groups. 22 Brown et al. also reported that married febrile or anemic patients received significantly less treatment (e.g., blood transfusion, antibiotics, fluids) than nonmarried patients in the same state of health. Two studies23,24 reported a statistically significant association between the length of hospital stay and the frequency of decisions about limiting treatment. In a retrospective survey among physicians and relatives conducted by van der Heide et al., 27 the authors found that, based on information from physicians involved in treatment, there were no statistically significant differences for limitation of cancer treatment between patients staying in hospitals, nursing homes, or at home. However, the wish of the patient as a reason for not starting a therapy was stated by physicians significantly more frequently with patients in nursing homes or at home compared to hospital patients. 28 The authors also reported that relatives of patients in nursing homes or at home indicated that patients had refused medical treatment more often.
Health- or treatment-related variables
Two out of four studies analyzing health- or treatment-related aspects as possible variables for treatment limitation described the patients' mental state as a variable associated with treatment limitation.21,22 In a retrospective medical chart review conducted by Brown et al., 22 there was a significant association between patients described as “comatose” and nontreatment decisions for febrile, dehydrated, or anemic patients. Furthermore, Hanson et al. 21 reported in a subset of 148 patients with cancer that patients lacking capacity to make decisions received chemotherapy significantly less often than competent patients (3% versus 32%), while there was no such difference with regard to treatment with radiotherapy. The authors also reported that lack of capacity was an independent predictor for decisions to limit life-sustaining treatment for the whole sample of 311 patients, which also included patients without cancer. Three studies reported that diagnosing patients as “terminal” or “dying” is significantly associated with decisions about the limitation of treatment.22,24,26 One of these studies, Morita et al., 26 additionally reported a statistically significant inverse association between physicians' judgment that rehydration was advantageous for the patient and a decision to withhold hydration in patients with cancer. 26 The timing of the establishment of supportive care plans was reported in one study conducted by Hui et al. to be significantly associated with decisions to limit cancer treatment. 24
Patients' preferences, end-of-life communication, and the role of relatives
Next to findings on contextual and health-related factors, we identified three studies that reported data regarding the influence of patients' preferences, the role of end-of-life communication between patients (or their representatives) and physicians, and the role of relatives concerning decisions about limiting treatment. In the study by Morita et al. on variables associated with decisions about limitation of hydration in patients with cancer in a palliative care unit mentioned previously, the authors described patients' “denial” as an independent predictor against limitation of rehydration. 26 The authors further reported that patients' or family members' belief that rehydration could worsen the patients' distress was significantly associated with decisions about the limitation of artificial hydration. By contrast, families' belief that limitation of hydration may increase the patient's anxiety or worsen the patients' symptoms was associated significantly with rehydration. 26 Mack et al. 22 showed in their study that white patients' wishes with regards to end-of-life care were followed significantly more often if there had been an end-of-life communication. Furthermore, this study shows that patients' awareness of their terminal situation was statistically significantly associated with a limitation of life-prolonging care. As reported regarding context factors, patients' preferences for treatment at the end of life were referred to significantly more often by physicians and relatives of patients in nursing homes and homecare compared with patients in hospitals. 27
Discussion
This paper summarizes sociodemographic, contextual, health-related, and further factors associated with explicit decisions about limiting treatment in end-of-life care for patients with cancer. While some of the variables prima facie seem more plausible (e.g., limitation of hydration in cases where this is perceived to be harmful) than others (e.g., differences in end-of-life treatment depending on ethnicity of the patient), a well-argued judgment can be made only after careful analysis from a clinical as well an ethical perspective. To the best of our knowledge, only one systematic review that had analyzed factors associated with different end-of-life practices across different patients groups has been published so far. 28 We have limited our review to decisions about limiting treatment in the group of patients with cancer to be able to take disease-specific aspects and ethico-legal characteristics into account. At the same time it is important to acknowledge that the clinical cases in which treatment is “limited” differ with regards to clinically and ethically relevant facts. While the number of eligible studies is small, the analysis of data suggests that value-laden factors influence decisions about limiting treatment in current practice.
Evaluating benefit and harm in the context of treatment limitation
The findings of the review show that decision criteria for limiting treatment are related to descriptive but also to normative features. To judge hydration not to be of advantage for the patient 26 is one example in this respect. While such judgment often can be linked to observable signs (e.g., edema), these decisions are eventually made with reference to an evaluation of benefit and harm. As experienced by many health care professionals, there may be differing outcomes of such evaluation: a patient (or the relatives) may deem “a drip” to be of utmost importance for his or her psychological well-being, while from a medical perspective such treatment may be considered inappropriate given the risk of lung edema.
In the context of the evaluation of benefit and harm of treatment, it is also of interest that two studies identified the mental state of the patients as a predictor for limitation of treatment in patients with cancer.21–22 While there are a number of health-related explanations for such an association (e.g., reduced consciousness), as well as clinically relevant issues (e.g., importance of cooperation), the findings raise questions about health care professionals' evaluation of benefit and harm of treatment in cases where patients are not able to decide. Particularly in times of scarcity of staffing and lack of time, one may ask how much investment is necessary in delivering care in this patient group to elicit patients' (presumed or stated in advance) preferences. With value judgments such as weighing benefit and harm being an integral part of clinical practice, it is important to be sensitive to this dimension of decision making and to seek strategies to make them explicit, in particular in cases where there are conflicting value judgments. Structured deliberation on such value judgments are, for example, done in clinical ethics case discussions 29 —one option to ensure that ethical aspects of treatment decisions are handled in a professional manner.
Patient preferences and modulating sociodemographic and contextual factors
Several studies included in this systematic review indicate that the impact of patients' preferences with regards to limiting treatment is modulated by sociodemographic and contextual factors. In two studies, the ethnicity of patients has been identified as such a modulating factor. While it is known that black patients more often receive intensive care at the end of life,30,31 the study of Mack et al. 25 shows that even if black patients state a wish for limiting treatment, there is no significant association of this wish with a factual limitation of treatment, which stands in contrast to the results of the group of white patients. This finding raises the question of whether prejudices or stereotypes of assumed wishes of patients with certain cultural backgrounds dominate the delivery of health care at the end of life. In societies with a diversity of ethnicities, cultural backgrounds, and associated values, professional end-of-life care needs not only to be informed about individual preferences, but to assess whether these preferences are put into practice and, if not, why this is the case and whether such decisions may infringe patients' rights. In this context and relevant for the interpretation of findings, the differing notions of autonomy in different cultures should also be taken into account.32,33 Interestingly, none of the studies included in this review assessed physicians' sociodemographic factors as possible determinants for decisions about limiting treatment. However, as pointed out by Seale 34 following a survey among physicians in the United Kingdom, physicians' ethnicity or religious belief influence end-of life decisions and should be taken into account when analyzing possible obstacles to implementing patients' preferred mode of care.
There is only one study in our sample, by van der Heide et al., 27 which compared decisions about limiting treatment in different settings of care. While the physician respondents did not report differences regarding the frequency of decisions about limiting treatment, the relatives of patients staying at home significantly more often reported a refusal of treatment by these patients. In line with this, physicians who cared for patients at home indicated significantly more often that a refusal by the patient was a reason to limit treatment. One interpretation of this finding, which is also in line with results from our own qualitative research,15,35 is that patients' preferences may be respected to differing degrees by health care professionals depending on the treatment setting. In settings characterized by availability of more technical treatment options, there seems to be a tendency to make use of the available facilities. Based on this interpretation we suggest that especially in treatment settings in which medico-technical interventions are accessible easily, the health care team should critically assess whether the use of available options is in accordance with the patient's will.
Limitations
One important methodological limitation is the low number of studies that could be included and that report descriptive findings lacking a predefined hypothesis. However, next to the fact that the findings of all included studies can be interpreted with regards to the potential role of value judgments, a contribution of this review is to point out the need for more robust research which can improve our knowledge about the factors associated with limitation of treatment. A second limitation of this review is its restriction to those studies that explicitly investigated decisions about limitation of treatment in patients with cancer. Accordingly we have excluded studies that analyzed limitation of treatment and other end-of-life-practices in different patient groups.36–38 An advantage of this approach is that the eligible studies are rather uniform with regards to disease-specific end-of-life trajectories and deal with a well-defined practice at the end of life. Another limitation is that all studies stem from countries with practices and values of the Western world and thereby cannot be extrapolated to practices in other countries. Last but not least our analysis, which has focused on patients with cancer, may need to be adapted for other fields of medicine.
Conclusions
This combined systematic review and clinical-ethical analysis indicates that a number of criteria associated with limiting treatment in clinical practice are value laden. Based on our clinical-ethical analysis, we argue that the normative dimension of variables associated with limiting treatment should be acknowledged as an inevitable part of clinical decision making, and strategies should be developed to handle these situations in the best professional way. Given the small number of studies on explicit decisions about limitation of treatment and the limited number of factors explored in these studies, we also suggest that further prospective studies with predefined hypothesis as well as mixed-method research should be conducted to shed more light on the factors associated with treatment limitation.
Footnotes
Author Disclosure Statement
All authors declare that there are no financial or nonfinancial competing interests.
Acknowledgments
The authors thank Prof. Wolf-Dieter Ludwig and his team from the Department of Hematology, Oncology, Tumorimmunology and Palliative Care at the HELIOS Klinik Berlin-Buch and the participants of the empirical ethics seminar at the Institute of Medical Ethics and History of Medicine, Ruhr University Bochum for their valuable comments during the preparation and analysis of this systematic review. In addition, we thank Dr. Pia Beiderwellen for her contributions to quality assessment and recommendations on data synthesis, and Birte Dahmen for her support regarding data extraction. Dr. Schildmann, Dr. Salloch, Anne Baumann (2010–2011), and Mahmut Cakar formed part of the NRW-Junior Research Group “Medical Ethics at the End of Life: Norm and Empiricism” (2010–2014) at the Institute for Medical Ethics and History of Medicine, Ruhr University Bochum which had been funded by the Ministry for Innovation, Science and Research of the German state of North Rhine-Westphalia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.