
Abstract
Abstract
Background:
The convergence of prevalence, cost, symptom experience, community setting, and informal caregiving in heart failure (HF) has profound implications for outpatient palliative care. The majority of HF patients depend on informal caregiver's assistance. Dyadic (patients and caregiver) characteristics can complicate this assistance. Yet relatively little is known concerning dyadic characteristics' impact on self-care. HF self-care involves routine, daily treatment adherence and symptom monitoring (self-care maintenance), and symptom response (self-care management).
Objective:
Describe the dyadic characteristics of mood and perception of the relationship in HF patients and caregivers, then explore the relationship of the characteristics with self-care.
Design:
Prospective, cross sectional study of hospitalized HF patients in mixed dyads (spousal/adult child/relative) analyzed using Actor-Partner Interdependence Model (APIM) techniques.
Measurements:
Mood was measured by the Brief Symptom Inventory and Patient Health Questionnaire, perception of the relationship by the Dyadic Adjustment Scale, and self-care by the Self-care in Heart Failure Index.
Results:
In 40 dyads the average patient was a 71 year old male (n = 30); caregiver was a 59 years old female (n = 26). Overall self-care scores were consistently low. Patient depression scores were significantly greater than caregivers (p = .0055). Greater caregiver anxiety were associated with lower caregiver maintenance scores (p < .0001) but greater caregiver depression were associated with lower patient maintenance scores (p < .0001). While patient and caregiver's perception of the relationship was associated with their self-care, more importantly, caregiver's perception of the relationship was associated with their confidence to engage in the patient's self-care (p = .003).
Discussion/Conclusion:
This study suggests that caregivers, often unacknowledged or unmeasured, impact patient's day to day HF self-care. Palliative care clinicians need to talk to dyads with a history of poor self-care about their relationship.
Introduction
A
HF self-care involves routine, daily treatment adherence and symptom monitoring (self-care maintenance), and symptom response (self-care management). 8 Self-care confidence or self-efficacy is known to facilitate self-care. 9 Recent studies suggest that patients' and caregivers' engagement in self-care impacts their own and their care partner's quality of life 10 and that patients engage less and caregivers engage more as HF progresses and the patient becomes sicker. 11 But what factors impact the patient's and caregiver's decision to engage or how fully to engage in self-care is currently poorly understood.
From the HF literature, anxiety and depression12,13 and perceptions of symptoms and the relationship14,15 are known to have personal and dyadic dimensions. Whether these factors influence engagement in HF self-care is less well known—the relationships between patients' or caregivers' depression, perception of the relationship, and patients' HF self-care has been explored in only one small, correlational study. Trivedi and colleagues 16 tested a conceptual model of dyadic characteristics and relationships with HF self-care, measuring depression, relational satisfaction, and self-care. Interesting associations were found between these variables, but further research was recommended. From the larger geriatric literature, perception of the relationship is a known contextual element in chronic illness management. 17 The quality of spousal relationships (one common dyadic relationship) moderates the association between the effects of symptoms on both partners. 18 Several recent, tantalizing glimpses are seen into the importance of dyadic interaction in HF. One study found that spousal distress predicted increases in patients' symptoms and poorer general health. 13 A series of palliative care papers19–21 support the impact of HF on the dyad 19 ; the importance of dyadic congruence in improving patient outcomes in HF 20 ; and that caregivers' perception of the relationship is associated with benefit or burden in their role. 21 But the relationships between dyadic characteristics and self-care outcomes has not been examined structurally in HF. The specific aim of this study was to first describe the dyadic characteristics of mood and perception of the relationship in HF patients and caregivers, and then explore the relationship of these dyadic characteristics with HF self-care.
Methods
Study design
This was a small, prospective study using cross-sectional data. The Actor-Partner Interdependence Model (APIM) 22 (see Fig. 1) provided the conceptual and analytic framework. This model posits that patient and caregiver characteristics are interdependent. The model accounts for this lack of independence by modeling the effect of the individual on their own outcomes as actor effects and the effects on the partner as partner effects. This project was not powered to test the model per se but rather to generate information on the participants, variables, and strength of the relationships between the variables.
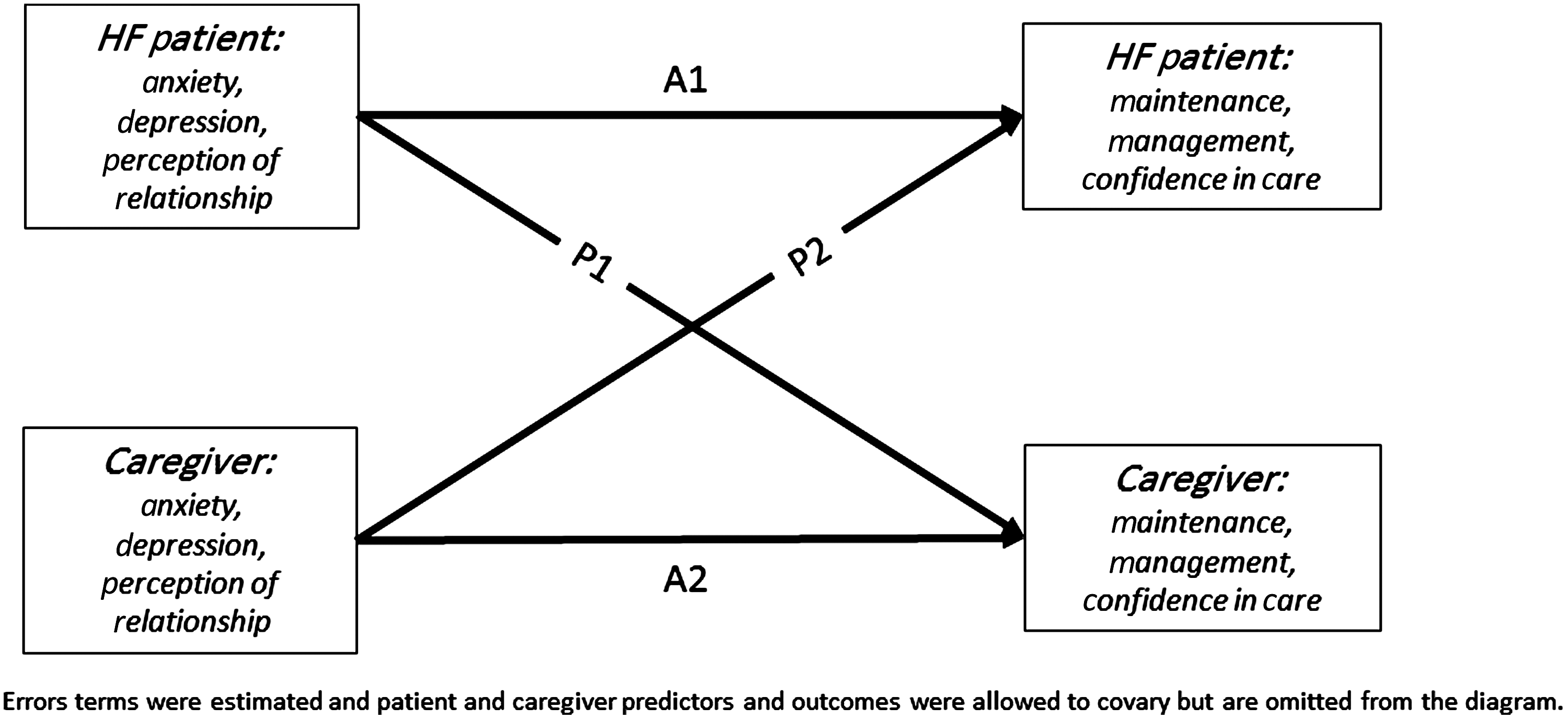
Actor-Partner Interdependence Model.
Setting and sample
Forty Stage C or D 1 HF patient and caregiver dyads were recruited from a community health system and an academic medical center in the northeastern United States. Institutional review board approval was obtained from both institutions, and informed consent was obtained from both patient and caregiver. Inclusion criteria were that patient and caregivers were both adults, 18 years of age or older; patient had a documented HF diagnosis in the medical record; and patient and caregiver were willing and able to participate. Patients were excluded if they had received a heart transplantation or a left ventricular assist device. These exclusion criteria were devised to assure the homogeneity of the caregiving experience. 23 Trained research assistants screened daily hospital admission records for patients admitted with a HF diagnosis in the previous 24 hours who met the inclusion criteria. This time was selected to allow for recent recall of symptom management. Patients were approached, the study was explained, consent was obtained, and questionnaire packets were completed in one visit. If a caregiver was not present at the visit, a packet was sent to the caregiver for completion.
Measures
Depression was measured by Patient Health Questionnaire-9 (PHQ-9). Responses range from 0 (“not at all”) to 3 (“nearly every day”) for a total score of 1 to 27 with a score of 10 used as a cut point for major depression. 24 The PHQ-9 is reported to have a sensitivity of 88% and specificity of 88% for detecting a major depression. 24 In this sample the coefficient alpha for the patient was 0.80 and for the caregiver was 0.91.
Anxiety was measured by the Brief Symptom Inventory (BSI). 25 The anxiety subscale consists of six statements rated on a scale of 0 (“not at all”) to 4 (“extremely”). The average of the six items comprises the total score, with a score of 0.35 or higher used as a cut point for anxiety. Reliability in the current sample was considered excellent (patient α = 0.82, caregiver α = 0.91).
Perception of the relationship was assessed using the Dyadic Adjustment Scale short form (DAS-7) developed by Sharpley and Rogers 26 from the longer version. 27 The DAS-7 consists of six statements about a person's perception of their degree of agreement on relational factors such as shared philosophy, goals, and time spent together. Participants are required to rate items on a scale from 0 (“always disagree”) to 5 (“always agree”). A seventh item asks their perception of degree of happiness in the relationship on a scale from 0 (“extremely unhappy”) to 6 (“perfect”). All items are summed to create a total score. In the current sample, reliability was acceptable for both members of the dyad (patient α = 0.70, caregiver α = 0.78).
Self-care maintenance, management, and confidence for the patient was measured by the Self-care of Heart Failure Index which includes a scale for each of the constructs. 28 The 10-item maintenance scale focuses on treatment adherence, such as following medication, diet, and exercise guidelines, and symptom monitoring on a 1 (“never or rarely”) to 4 (“always or daily”) point scale. The six-item management scale assesses the ability of the patient to recognize symptom occurrence, implement a meaningful treatment, and evaluate the outcome of that treatment choice on a 1 to 4 point scale. The six-item confidence scale assesses the perception of HF self-care self-efficacy on a 1 to 4 point scale. For all scales, higher responses reflect better self-care maintenance, management, and greater perceptions of self-care self-efficacy. Internal reliability and construct validity have been shown in multiple studies.8,29,30 Maintenance, management, and self-care self-efficacy for the caregiver were measured by an adaptation of the patient scales. This was developed in collaboration with other HF researchers and a similar caregiver adaptation has shown comparable psychometric properties with the patient instrument.31,32
Patient and caregiver sociodemographic data was by self-report, including age, gender, race/ethnicity, education level, and income.
Data analysis
The current analyses used APIMs 33 implemented using a structural equation modeling framework in MPLUS. 34 These models allow a researcher to simultaneously calculate the effects of the patient's experiences (i.e., mood state and perceptions of the relationship) on their own self-care maintenance, management, or self-efficacy and the effect of their experiences on the caregiver's ratings of the same outcome and vice versa. These models also account for the intercorrelation among partners for both the predictors and outcomes. Models in the current analysis were considered “just-identified,” because all possible relationships among variables were specified. Just-identified models will always have perfect model fit, 35 and individual model fits were not interpreted in light of this. Figure 1 depicts the general form of the APIM. Models were estimated using maximum likelihood estimation, which allowed patients to be included even when caregiver information was missing. These individuals contributed information to the estimation of actor effects in the models. Separate models were fit for each combination of predictors and outcomes resulting in nine models.
Results
Sample
Table 1 summarizes the demographic characteristics of the sample (patients n = 40; caregivers n = 31). Most patients were male (70%, n = 30). Caregivers were mostly female (81%, n = 26). Dyads primarily consisted of spousal pairs (65%) or a close relative (e.g., adult child, 35%). There were no differences in predictors or outcomes based on the type of dyad (all p's >0.18).
Generally, patients and caregivers scored below the cut-off for adequate self-care on the individual HF self-care scales. With the exception of patient self-care maintenance, the scores for both groups fell below the standardized SCHFI score of 70 (see Table 2). 28
To determine whether dyads with complete data differed from those with incomplete data, we conducted a missing data analysis by comparing scores for patients with available caregivers to those without. We found that there were no significant differences for patients with or without available caregivers on the independent variables (all p's >0.28). Specific to the HF self-care index, patients with available caregivers trended toward having lower HF self-care maintenance scores (t[38] = −2.00, p = 0.053) and lower HF self-care self-efficacy (t[38] = −1.88, p = 0.068). This suggests that patients with the greatest difficulty with self-care were more likely to have a caregiver who completed the questionnaire packet and returned it.
Patient and caregiver self-report outcomes
Means and standard deviations for all variables appear in Table 2. Using paired t-tests, we examined whether there were significant within-dyad differences. Depression was significantly different across members of the dyad, with the patient reporting significantly more depressive symptoms (in the mild to moderate level) compared with the caregiver. HF self-care maintenance scores were also significantly higher (but just adequate) for the patient. All other comparisons were not significant.
Relationships between patient and caregiver self-report outcomes
Tables 3 and 4 include the correlations for the variables of interest. The shaded diagonal in Table 4 illustrates the level of agreement within a dyad for a given measure. Only a few correlations reached significance, most likely due to the small sample size, but the directions were consistent with previous theory and research. Higher levels of depression correlated with higher levels of anxiety and poorer perception of the relationship. Specific to the HF self-care index scales, patient perceptions of the relationship were significantly, positively related to a caregiver's rating of their self-efficacy. Additionally, caregiver depression was negatively correlated with patient HF self-care maintenance. The strongest correlation on the same variable was the dyad's perception of the relationship.
*p < 0.05.
†p < 0.07.
Patient-caregiver raw intercorrelations.
p < 0.05.
p < 0.07.
Actor-Partner Interdependence Models
The goal of the current study was to explore the relationship of dyadic characteristics (e.g., anxiety, depression, and relationship quality) with HF self-care. Using the APIM framework, individual models were fit for each independent-dependent variable combination. Results for these models appear in Table 5 and are reported as standardized effects. Caregiver anxiety and depression each significantly predicted patient HF self-care maintenance as a partner effect. Higher levels of depression or anxiety for the caregiver predicted lower HF self-care maintenance scores for the patient. For the other HF self-care scales, only caregiver actor effects were significant. Higher caregiver anxiety predicted lower caregiver HF self-care management scores, and higher caregiver ratings of relationship quality predicted greater caregiver ratings of self-efficacy.
All bs (b, beta) are standardized using XY standardization.
Discussion
This study described the dyadic characteristics of mood and perception in HF patients and caregivers, then explored the relationship of the dyadic characteristics with HF self-care or how the dyad manages routine care and symptom exacerbations at home. What was found: (1) Higher caregiver anxiety and depression was associated with lower patient engagement in self-care maintenance (treatment adherence and symptom monitoring). (2) Higher caregiver anxiety was also associated with lower caregiver engagement in self-care management (symptom response and evaluation). (3) Caregiver perception of the relationship was associated with their self-efficacy in self-care.
Why is this study important? To date there has been little empiric evidence to support that caregivers have any effect on patient outcomes in HF. In a recent study, the association between family caregiver presence at clinic visits and self-care were examined and suggested that caregiver satisfaction with clinician communication mediates the relationship between frequency of caregiver presence at the clinic visit and better HF self-care maintenance and management at home. 36 Yet in a review of clinical encounter videos conducted at the Mayo Clinic, clinicians rarely engaged caregivers, even when present. 37 Taken together, these studies highlight the importance of clinician interaction with the caregiver, yet the linkage of caregivers to HF patient outcomes has been tenuous. A systematic review of caregivers' contributions to HF self-care found only 2 out of 40 studies attempted to quantify this relationship. 7 In a study similar to ours, Trivedi and colleagues found a relationship between caregiver depression and patient self-efficacy in bivariate correlation. 16 What our study adds to this emerging science is advanced modeling—we were able to examine the effects of the individuals' characteristics on their own self-care and the effect of their characteristics on their care partners' ratings of the same outcome simultaneously, while accounting for the known intercorrelations among partners for both the predictors and outcomes. Caregivers' mood states and perception of the relationship were found to be associated with the patients' and their own engagement in self-care and caregiver self-efficacy. Given the small sample size, the statistical significance speaks to the strength of the signal.
Due to rigorous adherence and symptom monitoring needs, HF co-opts time and energy of patients and caregivers (if present). One way to tease out the impact of the caregiver in HF self-care is to examine partner effects in the patient's self-care. Partner effects in the APIM measure the contribution of the caregiver's independent variable to the patient's dependent variable, accounting for the effect of the patient on their own variable. This study provides evidence that caregiver anxiety and depression are associated with poorer patient self-care maintenance. Simply put, the more anxious or depressed the caregiver was, the less likely that the patient was adherent or monitored their own symptoms.
This finding is particularly intriguing, as no actor effect of the patient's anxiety and depression on their own self-care maintenance was found despite the fact that the patients generally scored higher in depression (in the mild to moderate range) than the caregiver. This could be a function of our small sample size; with a larger sample we might have found patient effects, but it bears further consideration. Self-care maintenance involves everyday HF care. If the caregiver was anxious or depressed, the patient was less likely to report weighing themselves, checking their ankles for swelling, keeping clinician appointments, exercising, taking all of their medications, or watching their sodium intake. This caregiver effect on patient self-care maintenance may be a result of the anxious or depressed caregiver being less likely to cue the patient or that the patient is more concerned with the caregiver's state then with their own. Previously, strong, positive relationships were found in mixed (spousal, adult child, parent) dyad's shared care and self-care maintenance, supporting our findings that caregivers matter in self-care maintenance. 38 What this study adds is that this engagement in self-care maintenance can be negatively impacted by caregivers' mood states.
The current health care system is built on the assumption that caregivers will engage with the patient in self-care. But to what degree they are able to engage or what stressors in their own lives impact that engagement need to be better understood. A way to tease out the correlates of caregiver engagement in HF self-care is to study actor effects. Actor effects measure the contribution of the caregiver's independent variable on the caregiver's dependent variable, accounting for the effect of the patient. This study provides evidence that caregiver's anxiety is associated with their own engagement in self-care management, and their perception of the relationship is associated with their overall self-efficacy for self-care. The more anxious the caregiver, the poorer their engagement in making meaning of the patient's symptoms, taking action, and then evaluating the response to the action taken. In addition, the higher the caregiver rates their satisfaction with their relationship with the patient, the higher their self-efficacy related to HF care. Self-efficacy is important, as it has been found to mediate the relationship between social support and self-care management and moderate the relationship between self-care management and cost in HF. 8 In the same study that measured shared care, noted above, no associations were found between shared care with self-care management; however, moderate to weak associations were found with self-care confidence. 38 What this study adds is that caregivers are contributing to self-care management; however, caregiver anxiety is associated with poorer contributions. A second finding is that the caregiver's perception of their relationship is related to their self-efficacy in self-care.
Limitations
This study has several limitations. First, the sample is primarily white and of moderate income. More diverse samples may result in different outcomes. Second, the sample is relatively small and measured at one time point. Once again, a larger sample measured over time may provide additional findings.
Implications for outpatient palliative care
There are several implications for palliative care found in this study. First, these findings may have relevance to other chronic disease populations with rigorous self-care requirements. Caregivers may or may not have their own chronic illnesses and suffer from poor self-efficacy impacting their ability to engage. Some of these stressors, such as anxiety and depression, can be mitigated, potentially resulting in improved patient self-care. However, in the present health care system, providers are not reimbursed for providing family interventions; thus, care for caregivers is unlikely to happen. Secondly, assessing for these stressors and providing additional self-care information involves communication. Clinicians need to talk to the patient and caregiver about their mood states and relationship, particularly in dyads with a history of poor self-care. Communication is a nonpharmacological intervention that improves patient outcomes.
Conclusion
In summary, we found that caregivers' mood states and perception of the relationship impacts the patient and their own engagement in HF self-care as well as the caregiver's self-efficacy. The next steps in this line of inquiry is to determine if dyadic HF self-care interventions that address mood states and support the relationship result in better self-care outcomes.
Footnotes
Acknowledgments
This study was supported by the National Palliative Care Research Center Junior Faculty Career Development Award.
Author Disclosure Statement
No competing financial interests exist.