
Abstract
Abstract
Background:
Framing is known to influence decision making.
Objective:
The study objective was to describe language used by physicians when discussing treatment options with a critically and terminally ill elder.
Methods:
High-fidelity simulation was used, involving an elder with end-stage cancer and life-threatening hypoxia, followed by a debriefing interview. Subjects were hospitalist, emergency medicine, and critical care physicians from three academic medical centers. Measures were observation of encounters in real time followed by content analysis of simulation and debriefing interview transcripts. During the simulation we identified the first mention (“broaching”) of principal treatment options—intubation and mechanical ventilation (life-sustaining treatment [LST]) and palliation in anticipation of death (palliation)—and used constant comparative methods to identify language used. We identified physician opinions about the use of LST in this clinical context during the debriefing interviews, and compared language used with opinions.
Results:
Among 114 physician subjects, 106 discussed LST, 86 discussed palliation, and 84 discussed both. We identified five frames: will (decided), must (necessary), should (convention), could (option), and ask (elicitation of preferences). Physicians broached LST differently than palliation (p<0.01), most commonly framing LST as necessary (53%), while framing palliation as optional (49%). Among physicians who framed LST as imperative (will or must), 16 (30%) felt intubation would be inappropriate in this clinical situation.
Conclusions:
In this high-fidelity simulation experiment involving a critically and terminally ill elder, the majority of physicians framed the available options in ways implying LST was the expected or preferred choice. Framing of treatment options could influence ultimate treatment decisions.
Introduction
S
While the content of physician-patient communication undoubtedly influences decision making, the language used to frame treatment alternatives also has the potential to influence decision making. We define framing as “the act, process, or manner of constructing” something through the selection of words, metaphor, or reference points. Framing has known effects on decisions. Kahnemann and Tversky demonstrated that framing risk in terms of potential gain or loss changes choice. 6 Public opinion research has shown that varying emphasis on social values can shift opinions about issues, such as whether hate groups should be allowed to hold political rallies. 7 In the context of medical decision making, framing influences parents' opinions regarding resuscitation of extremely premature infants 8 and it influences potential patients' interest in preventive surgery. 9 Nonetheless, little is known about how framing can influence decision making at the end-of-life.
The purpose of the current study was to describe the language used by physicians to introduce (i.e., to broach) treatment options for a terminally ill elder presenting with critical illness: intubation and mechanical ventilation (life-sustaining treatment) versus palliation in anticipation of death.
Methods
Between 2007 and 2009, we performed three studies of physician decision making for patients at the end of life, using a high-fidelity simulation to standardize the clinical context: a study of the feasibility of using simulation to understand decision making, 10 a study of the effect of patient race on decision making, 11 and a study of the effect of institutional norms on decision making. 12 Here, we report a secondary analysis of those simulation encounters and debriefing interviews.
Simulation
We have previously described the details of the development and validation of the simulation.10,11 Briefly, the simulation took place on a set designed to mimic either an emergency department room (for emergency medicine physicians) or a ward room (for hospitalists and critical care physicians). An experienced, trained standardized patient depicted a 78-year-old bedbound man with metastatic cancer and life-threatening hypoxia. Physician subjects were asked to imagine that they were cross-covering for a colleague. They had to decide how to manage the patient based on information elicited from the patient, his surrogate (also present at the bedside), the chart, bedside vital signs tracings, and any diagnostic tests or therapeutic interventions they wished to order. The simulated patient had stable preferences to avoid intubation and mechanical ventilation but would share that information only if asked. If the physician did not directly elicit preferences, the actors were trained to follow the physician's lead: if the physician recommended LST without offering alternatives, the patient was to accept, and if presented with multiple options, the patient was to ask the physician for a recommendation. We halted the simulation when the physician articulated a plan.
Debriefing interviews
After completing the simulation, one investigator conducted a debriefing interview with the physician subject. The investigator played a video recording of the subject's encounter, stopping the video at prespecified decision points and standardized patient statements or every two minutes, whichever came first, to probe “Tell me what was going on here?” At the close of the interview, we additionally probed with the questions, “If you had done [the opposite of what the subject ordered, such as intubating the patient when they had ordered comfort measures only, or vice versa], what would have happened to the patient?” and, “What would your colleagues have thought, done, or said?”
Participants
As previously reported, we recruited board-certified emergency medicine (EM) physicians, hospitalists, and intensivists responsible for managing or triaging critically ill patients in the hospital setting from three U.S. academic medical centers. We recruited providers through in-person presentations at respective faculty meetings, e-mails to department distribution lists, and calls or visits to physicians' offices.
Data collection
Each physician provided demographic, training, and employment data. Two investigators (AB and DM) conducted the simulations at each institution's simulation center, which were audiorecorded and later transcribed. During the study on race, participants completed two encounters with otherwise similar black and white patients. For these physician subjects we restricted analysis to the first encounter. 11 Physicians in the studies on the effect of race and of norms on decision making also participated in a cognitive debriefing interview after the simulation, which were audiorecorded and later transcribed.
Qualitative content analysis
Simulation encounters
We used a constant comparative method approach to develop the coding framework for the simulation and interview transcripts. Investigators (AB and DM) debriefed daily to discuss their observations after watching simulation encounters live. Based on observations regarding apparent differences in word selection when discussing treatment options, a multidisciplinary team reviewed a random selection of encounter transcripts and systematically compared textual segments in which physicians first broached the two principal treatment options: intubation and mechanical ventilation (life-sustaining treatment) and nonintubation and initiation of palliation in anticipation of death (palliation). The group identified five distinct frames used by physicians when discussing intubation and palliation (see Table 1). “Will” referred to textual segments communicating a decided action; “must” referred to segments communicating a necessary action; “usually” referred to segments communicating a conventional or usual action; and “could” referred to those communicating a potential or optional action. The fifth, “ask,” referred to segments in which the physician made statements or asked questions intending to elicit the patient's treatment preference. We then developed a detailed codebook with definitions and examples for each of the five major strategies used for life-sustaining treatment and palliation. One investigator applied the codebook to all 114 encounters (AL), and a second (DM) evaluated a random 20% sample of transcripts to assess the reliability of the coding. Co-coders achieved a kappa statistic of 0.7–0.8, indicating excellent interrater reliability. 13 Coders resolved disagreements through consensus.
Debriefing interviews
After completing the analysis of the encounters, the team systematically identified any segments in the debriefing interview in which the physician articulated an opinion regarding intubation and mechanical ventilation in this clinical situation. We classified articulated opinions into those in favor of and those against intubation (see Table 2). One investigator then applied the codebook to all 89 interviews (CM), and a second (AL) evaluated a 20% sample to establish reliability. Co-coders achieved a kappa statistic of 1.0, indicating perfect interrater reliability.
Statistical analysis
We summarized the characteristics of the participants using means and proportions. We categorized the order in which physicians broached the possibility of using life-sustaining treatment or palliation. We summarized the frequency with which physicians used each frame to discuss life-sustaining treatment and palliation, and compared the use of frames for life-sustaining therapy and palliation using McNemar's test for nonindependent samples. Among physicians who completed a debriefing interview, we dichotomized frames as “will/must” or “other.” We then summarized the frequency with which physicians used “will/must” but expressed opinions against life-sustaining therapy, to gain insight into the possibility of physicians unwittingly framing life-sustaining treatment as the preferred treatment option despite clinical opinions indicating otherwise. We conducted all analyses with Stata statistical software version 11.1 (StataCorp LP, College Station, TX).
Human subjects
The institutional review boards of the three academic medical centers reviewed and approved the study. We received permission to tell physician participants that our purpose was to study “how physicians make decisions for patients with whom they do not have an established relationship” without disclosing until after completion of participation that we were interested in end-of-life communication and decision making. All physicians provided written informed consent for participation.
Results
Participants
One hundred fourteen physicians completed the simulation: 29 (25%) were emergency medicine physicians, 40 (35%) were hospitalists, and 45 (39%) were intensivists (see Table 3). Physicians' mean age was 40 years (SD=9.15). On average, 13 years (SD=9.03) had elapsed since their medical school graduation, and 8 years (SD=7.23) since joining their current institution. Most participants were men (72%) and non-Hispanic whites (68%).
Language framework
Among 114 participants, we excluded six physicians: four did not broach life-sustaining therapy or palliation (see online Supplementary material at www.liebertpub.com/jpm and at www.liebertonline.com), and two used approaches that could not be classified in one of the five language frames. (One asked, “Did [your doctor] mention hospice or palliative care?” and the other spoke to the investigators who were controlling the simulation behind a two-way mirror, rather than to the patient or his surrogate, saying, “I would make sure that somebody had the conversation with [the patient] where we more comfortably introduced…and then raise the question about foregoing life support.”) Of the remaining 108 participants, 106 broached intubation as a treatment option, 86 broached palliation, and 84 broached both.
We found that when discussing these end-of-life treatment options, physicians most commonly broached intubation first (64%), and did not broach palliation until after the patient or his surrogate expressed his preference to avoid intubation (see Table 4). Fewer (12%) broached intubation, and elicited intubation preferences without mentioning palliation as an alternative. A few physicians (8%) presented both treatment alternatives first, then assessed treatment preference. Of note, only three (3%) physicians explored the patient's preferences before broaching any treatment options.
Of the 106 encounters in which life-sustaining treatment was broached, the most common frame was “must,” in 56 (53%) encounters. Phrases meeting this classification included, “we may need to,” “he needs,” or “we should,” reflecting an attitude of necessity adopted by the physician toward intubation. For example, one subject stated, “He will more than likely require more oxygen in the near future…. At some point it will require putting a tube down and breathing for you with a mechanical device.” In contrast, examples in which palliation was broached using a “must” frame, such as, “So in talking to you guys it seems like we should do whatever we can just to make him comfortable,” occurred much less frequently, in only 22 (26%) encounters.
Of the 86 encounters in which palliation was broached, the most common frame was “could,” in 42 (49%) encounters. Phrases meeting this classification included “we can,” “we may,” and “the options include,” reflecting notions of optional possibility adopted by the physician regarding palliation. For example, one subject offered, “There are a few things that we could try to make you more comfortable.” Another subject stated, “We can keep doing maximum management…and if things are not working, then we can just withdraw all those things…we can just control your pain…and we can consult some palliative care people to provide you some support.” In contrast, examples in which life-sustaining therapy was broached using a “can” frame (e.g., “We could put you on a breathing machine if your breathing gets to be too labored”) occurred much less frequently, in only 10 (9%) encounters. There was a statistically significant difference in the frame used to broach life-sustaining treatment compared to palliation (p<0.01; see Fig. 1).
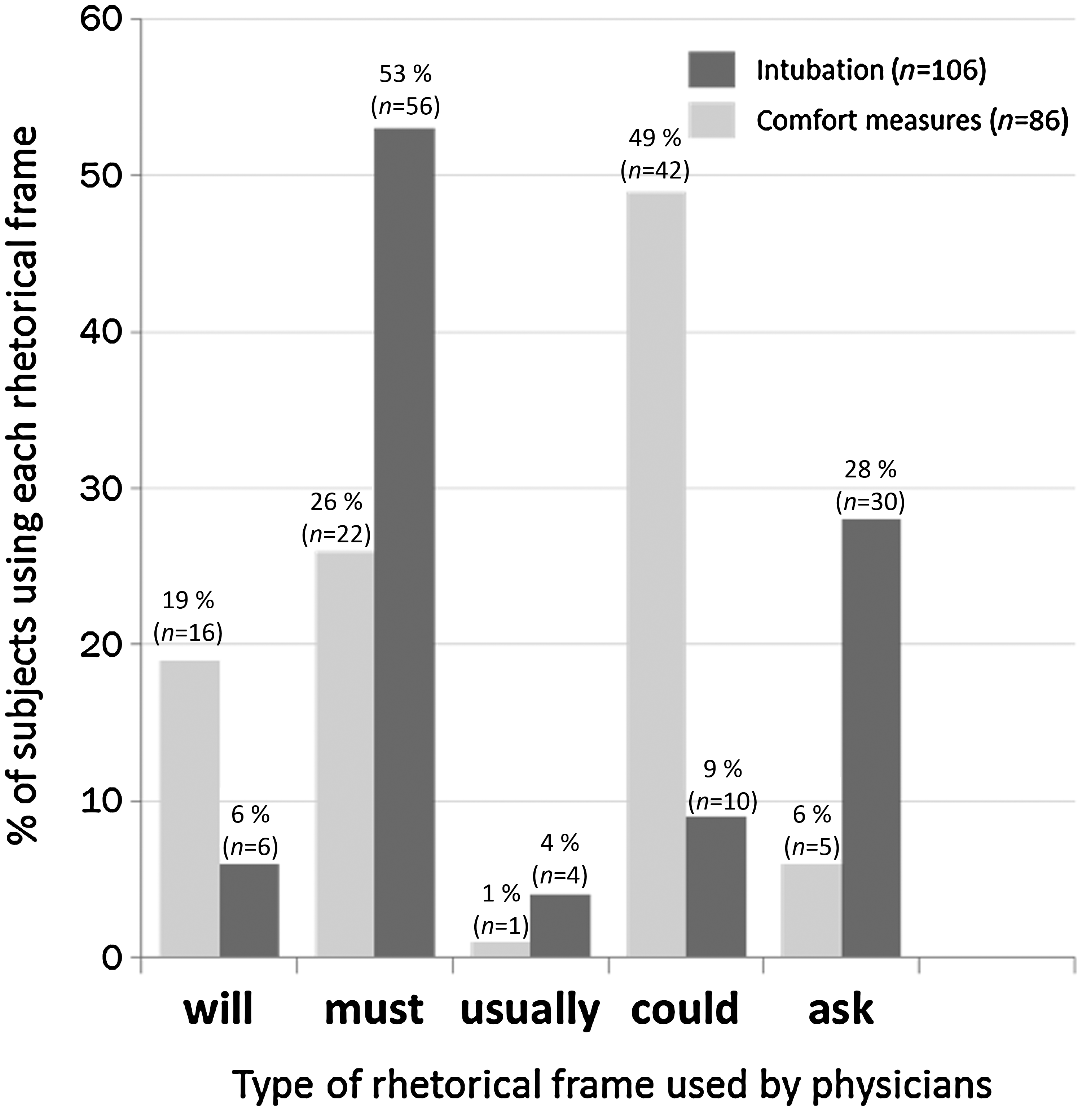
Frequency data for physicians' use of frames in broaching treatment options.
Comparison of physician language and clinical opinion
Among 89 physicians who participated in debriefing interviews, 5 had been excluded from the analysis above; an additional 2 interviews contained inaudible segments and could not be transcribed. Of the 82 remaining subjects, 48 used language during the simulation encounter implying they viewed life-sustaining treatment as necessary, using “will” or “must” frames. Yet in debriefing interviews, 16 (33%) felt intubation would be inappropriate in this clinical situation. Illustrating this tension, one subject explained, “We need to go to an ICU, do all that kind of stuff, but I also know that this guy has got metastatic cancer and he is dying from it…. I know that this guy needs to get intubated and I do not really think we should.”
Discussion
In this qualitative analysis of high-fidelity simulation encounters involving a critically and terminally ill elder, we observed that physicians used distinct language to discuss the available treatment options. The majority of physicians discussed life-sustaining treatment first, and only broached palliation as an alternative after the patient revealed his preference to avoid intubation. They most often framed life-sustaining treatment as required, whereas they framed palliation as optional. Many who framed life-sustaining treatment as necessary expressed the opinion during debriefing interviews that life-sustaining treatment was not the appropriate option for the patient in this scenario.
While studies of shared decision making at the end of life have focused on the content of communication,4,5,14 less is known about the language used by physicians in these discussions. A recent study by Dieltjens et al. evaluating conversations between physicians and patients requesting physician-assisted suicide in the Netherlands 15 analyzed communication style at the level of grammatical expression. They reported differences between physicians in their usage of modal verbs. Modal verbs do not express actions or what actually happened, but instead express an attitude adopted by the speaker toward the situation being described. Common modal verbs include can, could, may, might, must, shall, should, will, and would, and express semantic notions of possibility, necessity, obligation, intention, and ability. 16 Upon finalizing our code book, we discovered that three of our categories—will, must, and could—fit remarkably well into this lexical classification of modal verbs. However, in contrast to the study by Dieltjens et al., which selected preexisting categories (Dutch modal verbs) and applied them to the data, we began with the data and inductively derived distinct categories of frames, some of which corresponded to modal verbs.
The difference in the language used to describe treatment options probably occurs unconsciously by the physician. This hypothesis is supported by the observation that many physicians who framed the life-sustaining treatment option as necessary later expressed the opinion that intubation was inappropriate because it would not change the outcome (i.e., inpatient death). We believe that this discrepancy between language chosen and opinion implicitly reflects the tension between the physiologic imperative inculcated by medical training (i.e., a patient with an oxygen saturation that low needs to be intubated) and basic principles of medical decision making (i.e., will intubating this patient change the outcome). There are many valid reasons that may have led physicians to describe intubation more imperatively than palliation, such as clinical uncertainty regarding the reversibility of the acute deterioration. Rightly or wrongly, providers may also worry about losing the patient's trust by raising the option of palliation upon a first meeting. However, it is interesting that this imperative was unwittingly expressed while discussing treatment options even among those who strongly believed intubation would not alter the patient's outcome. Ultimately, the framing of intubation as an imperative reflects the default in the United States to initiate or escalate life-sustaining therapy unless an alternative is actively chosen.
Understanding the language physicians use to discuss treatment alternatives has importance, because framing has the potential to exert significant influence over preference and choice. Evidence suggests that the selection of default options influences behavior in many health care settings, from organ donation 17 and influenza vaccination 18 to end-of-life decision making. In decisions about code status, patients' treatment preferences can depend on whether they must opt-in or opt-out of life-sustaining treatment, 19 what treatment option comes preselected on an advance directive form, 20 and which option is implied to be the social norm. 21 In addition to reinforcing the default, language may also influence behavior via more subtle mechanisms. A recent study demonstrated that people were more likely to choose cardiopulmonary resuscitation (CPR) if the withhold-CPR option was framed as “do not resuscitate” compared to “allow natural death.” 21 As with the use of euphemistic words and phrases, the choice of particular modal verbs may independently modify patients' treatment preferences.
Our work has a number of limitations. First, we used a standardized patient to study communication and decision making, which has unclear generalizability to real practice patterns. However, simulation allowed us to study end-of-life decision making in a context that would be challenging to study in real-world practice, because it is unscheduled and time-pressured. Another strength of simulation was our ability to hold clinical and sociodemographic variables of the case constant. These factors vary in the real world, with greater prognostic uncertainty or patient/family ambivalence regarding treatment preferences perhaps tipping the scale in favor of a time-limited trial of life-sustaining treatment (and greater use of will/must/should if intubation is broached)—and well-documented treatment preferences, such as a “do not attempt resuscitation” order on the chart perhaps tipping the scale in favor of palliation in anticipation of death (and greater use of could/ask if intubation is broached). Our findings are all the more compelling given the clinical context we created. Second, we evaluated the practices of a small sample of physicians from three academic medical centers, producing observations that may lack generalizability. However, this analysis was designed to be exploratory and hypothesis-generating. Specifically, our work has produced an empirical framework to evaluate the language used by physicians to discuss decisions the end of life, and the need to understand the degree to which this framing might influence decision making by patients.
Conclusion
Shared decision making is the recommended model for communication between physicians and patients or surrogates for decisions regarding end-of-life-treatment for patients with terminal illnesses. In this high-fidelity simulation experiment involving a critically and terminally ill elder, the majority of physicians framed the available options in ways implying life-sustaining treatment was the expected or preferred choice. Physicians' unconscious framing of treatment options could influence ultimate treatment decisions. Increased recognition of what is likely an inadvertent difference in framing of treatment options may help physicians to choose their language more carefully.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.