
Abstract
Abstract
Background:
Numerous studies have focused on the treatment of non-small cell lung cancer patients with brain metastases. However, to our knowledge, few have sought to examine outcomes in patients who required whole brain radiation and developed radiation-refractory disease.
Methods:
This study examined the medical records of all non-small cell lung cancer patients who developed brain metastases between 2004 and 2013, required whole brain radiation, and received their cancer treatment at the Mayo Clinic in Rochester, Minnesota.
Results:
A total of 141 patients, most of whom were symptomatic, met the above criteria. Of these, 33 (23%) did not tolerate a corticosteroid taper and were therefore deemed to have radiation-refractory disease. The median survival of patients with and without radiation-refractory disease was 3.12 and 4.27 months, respectively, (hazard ratio [HR]: 0.65 [95% confidence interval (CI): 0.44–0.99]; p=0.04 by log rank test). In a subgroup analysis of patients with radiation-refractory disease (n=33) and radio-responsive disease (n=43), median survival was 3.12 and 5.94 months, respectively (HR: 0.43 [95% CI: 0.26–0.70]). Among patients with radiation-refractory disease, 12 received chemotherapy after radiation, and two received erlotinib. Systemic therapy was associated with improved symptoms in two patients but did not appear to improve survival.
Conclusion:
Non-small cell lung cancer patients with radiation-refractory brain metastases represent a small subgroup who have a short survival and who appear to derive minimal benefit from systemic cancer therapy.
Introduction
O
In contrast, a paucity of research is available on patients with no surgical or stereotactic radiation options and with radiation-refractory intracranial metastases. Typically, when first diagnosed with brain metastases, these patients receive corticosteroids for cerebral edema, whole brain radiation, and then a corticosteroid taper. However, when neurological symptoms persist, recur, or arise during the corticosteroid taper, the literature provides scant data on outcomes. How large is this subgroup with radiation-refractory brain metastases? What are their symptoms? Should these patients be treated with systemic therapy, such as chemotherapy, or palliative care alone?
In view of the large proportion of lung cancer patients with brain metastases, this study attempted to answer these questions.
Methods
Overview
The Mayo Clinic Institutional Review Board approved this study, which focused on non-small cell lung cancer patients treated at the Mayo Clinic in Rochester, Minnesota from January 1, 2004 to December 31, 2013. These dates provide approximately a decade of contemporary experience that coincides with the approval of erlotinib, a targeted epidermal growth factor receptor inhibitor. 6
The Mayo Clinic Tumor Registry provided a file of patients diagnosed with brain metastases. Patients were excluded if they had received resection or stereotactic radiation. This list was culled to create a final one of those who received whole brain radiation.
Clinical data
Medical records were abstracted for patient date of birth, gender, date of cancer diagnosis, cancer histology, date of brain metastases and associated symptoms, dates of whole brain radiation, vital status, and date of death or last follow-up.
The medical record was examined for information on whether patients tolerated a steroid taper. A steroid taper was defined as a planned reduction in corticosteroid dosing over time, as described in the medical record. Patients were considered intolerant of a steroid taper in the event of recurrent, persistent, or new neurological symptoms. These patients were considered to have radiation-refractory disease. In the event of ambiguity—either because the specific corticosteroid dose was not noted in the medical record or because the patient transitioned quickly to hospice—then a separate “unable to determine” category was used. Information on post-radiation systemic cancer therapy was abstracted for patients with radiation-refractory brain metastases. One of the authors (CMS) performed this medical record review; spot checks were performed by another (AJ).
Data analyses
Results are reported descriptively. In making comparisons, patient groups were collapsed if doing so seemed clinically logical with enhanced statistical power; for example, the category to denote that a patient tolerated the corticosteroid taper and the category “unable to determine” were collapsed into one group. Exploratory subgroup analyses were performed as appropriate and are reported as such. Kaplan Meier curves were constructed based on whether patients had clear evidence of radiation-refractory brain metastases. Data were censored as appropriate, and a log rank test was used to compare overall survival. Cox regression hazards models were used to assess factors associated with improved survival. A p value of<0.05 was considered statistically significant.
Results
Demographics
Among these 141 patients, 33 (23%) were deemed to have radiation-refractory brain metastases. Demographics appear in Table 1. Of note, 47 patients appeared to have tolerated a corticosteroid taper, and the remaining fit into the “unable to determine” category. Most patients were symptomatic from their brain metastases at initial presentation (Table 2).
Numbers in parentheses refer to percentages of the group referred to in that column, unless otherwise specified.
Age refers to age at time of diagnosis of brain metastases.
Numbers in parentheses denote the number of patients who had this symptom, with some patient's having more than one symptom.
Cancer treatment with radiation-refractory brain metastases
Among patients with radiation-refractory brain metastases, 12 received chemotherapy after radiation; two received erlotinib. Two who received chemotherapy manifested symptom improvement.
Of note, the tumor's epidermal growth factor receptor mutation status was not checked in most patients with radiation-refractory disease, but it was checked in three; one patient's cancer had an epidermal growth factor receptor exon 19 deletion.
Survival
Among the 33 patients with radiation-refractory brain metastases, 29 were deceased at the time of this report; in the remaining group (which included those who tolerated the corticosteroid taper and those in whom it was unable to be determined), 97 were deceased. The median survival for patients who did and did not have radiation-refractory brain metastases was 3.12 and 4.27 months, respectively (hazard ratio [HR]: 0.65 [95% confidence interval (CI): 0.44–0.99]; p=0.04) (Fig. 1). In an exploratory subgroup analysis of patients with radiation-refractory disease (n=33) and radio-responsive disease (n=43), median survival was 3.12 and 5.94 months, respectively (HR: 0.43 [95% CI: 0.26–0.70]; p=0.0004).
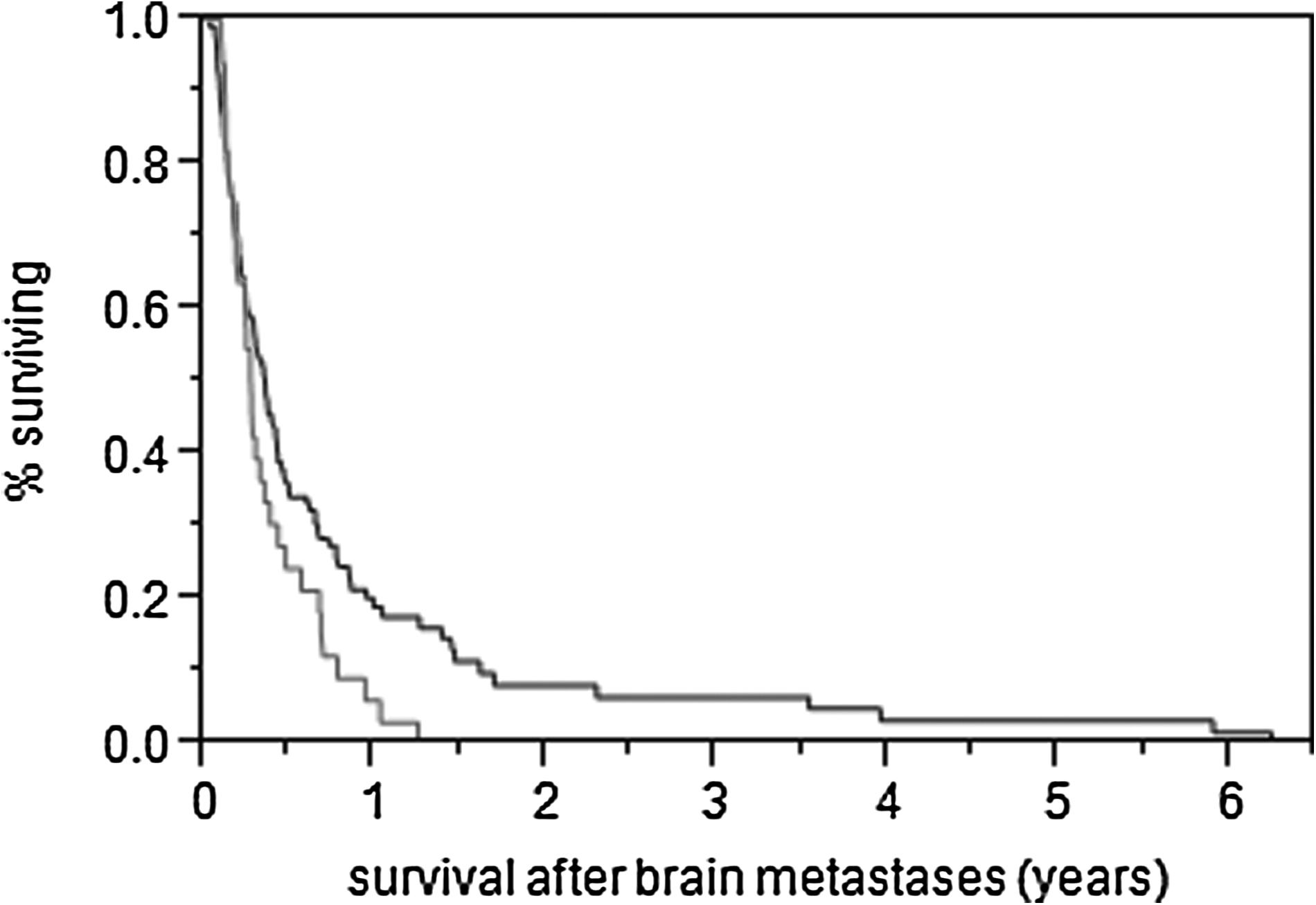
The median survival for patients who did (lower curve) and did not (upper curve) have clear-cut radiation-refractory brain metastases was 3.12 and 4.27 and months, respectively (hazard ratio 0.65 [95% confidence interval: 0.44–0.99]; p=0.04 by log rank test).
Among the 33 patients with radiation-refractory disease, those who received chemotherapy or erlotinib did not appear to gain a statistically significant improved survival compared with those who did not with a median survival of 3.36 months and 3.22 months, respectively (HR: 1.07 [95% CI: 0.50–2.21]; p=0.86). One patient with radiation-refractory disease was diagnosed with synchronous brain metastases, started erlotinib at diagnosis with an exon 19 deletion, but lived only slightly over 3 months after her diagnosis of brain metastases.
Discussion
This study generated outcome data from non-small cell lung cancer patients with radiation-refractory brain metastases. It provides three observations. First, 23% of patients have radiation-refractory metastases, per the definition used here. This problem is small but not trivial. Second, patients with brain metastases appear to be highly symptom-laden with headaches, extremity weakness, and other neurological deficits. Patients with radiation-refractory brain metastases are no exception, but their situation is particularly concerning because their symptoms are unremitting. Although chemotherapy might have improved symptoms in two patients, it is challenging to know for sure because the “placebo” effect can account for symptom improvement in 30% to 40% of cancer patients. 7 In essence, most radiation-refractory patients who received chemotherapy derived marginal symptom improvement. Finally, survival in lung cancer patients with brain metastases and no local therapeutic options is severely compromised, in the range of only 4 months. 1 Survival is even worse in patients with radiation-refractory brain metastases; as shown in this report, these patients lived a median of 3 months.
This last point is poignant when one considers that patients with radiation-refractory brain metastases often have unremitting symptoms. Previous studies have questioned the importance of the blood–brain barrier in shielding brain metastases from chemotherapy; these studies have reported intracranial tumor response rates of 30% to 50% in solid tumor cancer patients, although overall survival in these trials remained modest. 8 Furthermore, small prospective studies have reported intracranial tumor response rates of 50% to 80% with the use of erlotinib with the more favorable rates derived from lung cancer patients with tumors with epidermal growth factor receptor mutations. 9 However, to our knowledge, none of these studies focused on highly symptomatic patients with radiation-refractory brain metastases. Although the current study provides descriptive data on only 33 patients with radiation-refractory brain metastases, we found marginal data to indicate that systemic chemotherapy improves symptoms and no compelling evidence that systemic antineoplastic therapy leads to improvements in survival. The above findings might make health care providers pause before recommending systemic therapy to these patients.
Our study has limitations. First, the fact that we defined radiation-refractory disease based on neurological symptoms during a corticosteroid taper is unprecedented, further illustrates the paucity of research in this area, and reflects an acknowledgment that brain imaging is often not performed under these circumstances, particularly so soon after the completion of radiation. In effect, we needed to develop our own definition. Admittedly, a small subgroup of “radiation-refractory” patients may have developed neurological symptoms as a result of the whole brain radiation itself. If this had been the case, the outcomes described here might have appeared more favorable than those seen in patients with uncontroversial, progressive intracranial tumor growth, as indicated in our survival subanalysis. Thus, despite this limitation, it is unlikely that our conclusions would be altered had we used a more restrictive definition of radiation-refractory disease. Importantly, our findings also suggest that patients with radiation-refractory disease—as defined here—might be candidates for thoughtful end-of-life discussions. These discussions might focus on the fact that these patients might not have long to live, would potentially benefit from supportive care exclusively, and might specifically benefit from the use of hospice resources. Second, the number of patients with radiation-refractory brain metastases turned out to be quite small. Although this limited sample size is a shortcoming, it underscores the need to conduct further research in this area. Finally, the retrospective nature of this study carries limitations, particularly with respect to understanding symptoms and their temporal resolution. This limitation once again underscores the need for further research, preferably in a prospective manner.
In summary, a subgroup of non-small cell lung cancer patients develops radiation-refractory brain metastases. They are symptomatic with a shortened survival and gain dubious benefit from systemic therapy. These findings allow for better counseling of patients who face these circumstances and underscore the need for further research.
Footnotes
Author Disclosure Statement
No competing financial interests exist.