
Abstract
Abstract
Background:
An order protocol for distress (OPD), including respiratory distress and acute pain crisis, has been established for pediatric palliative care patients at Sainte-Justine Hospital (SJH). After discussion with the patient/his or her family, the OPD is prescribed by the attending physician whenever judged appropriate. The OPD can then be initiated by the bedside nurse when necessary; the physician is notified after the first dose is administered.
Objectives:
The study objectives were to evaluate the perceptions and experience of the medical/nursing staff towards the use of the OPD.
Methods:
A survey was distributed to all physicians/nurses working on wards with pediatric palliative care patients. Answers to the survey were anonymous, done on a voluntary basis, and after consent of the participant.
Results:
Surveys (258/548) were answered corresponding to a response rate of 47%. According to the respondents, the most important motivations in using the OPD were the desire to relieve patient's distress and the speed of relief of distress by the OPD; the most important obstacles were going against the patient's/his or her family's wishes and fear of hastening death. The respondents reported that the OPD was frequently (56%) or always (36%) effective in relieving the patient's distress. The respondents felt sometimes (16%), frequently (34%), or always (41%) comfortable in giving the OPD. They thought the OPD could never (12%), rarely (32%), sometimes (46%), frequently (8%), or always (1%) hasten death. Physicians were less favorable than nurses with the autonomy of bedside nurses to initiate the OPD before notifying the physician (p = 0.04). Overall, 95% of respondents considered that they would use the OPD in the future.
Conclusions:
Data from this survey shows that respondents are in favor of using the OPD at SJH and find it effective. Further training as well as support for health care professionals are mandatory in such palliative care settings.
Introduction
C
Objectives
The study objectives were to evaluate the perceptions and experience of the medical/nursing staff towards the use of the OPD.
Methods
The OPD used at SJH is detailed in Table 1. A previous study in our institution demonstrated that the indication to initiate the OPD is severe and acute onset of respiratory distress in 84% of the cases, an acute pain crisis not relieved by regular medication in 10% of the cases, and severe anxiety (panic/agitation/delirium) in 5% of the cases. 15
OPD, order protocol for distress.
This study uses a survey which evaluated perceptions and personal experience of the medical/nursing staff regarding the use of an OPD in pediatric palliative care patients at SJH. Questions were elaborated according to the recommendations of A Guide for the Design and Conduct of Self-Administered Surveys of Clinicians from Burns et al. 16 Item generation (consideration of all potential ideas) and item reduction (limitation to the relevant questions) was done through a focus group session with 15 experts (see Acknowledgments). The survey was developed in collaboration with a biostatistician (TD) to ensure that the data required for analysis would be obtained in a usable format. The appropriateness of each question and whether respondents interpreted questions in a consistent manner was assessed using pretesting with 10 of the previous 15 experts. In order to demonstrate that the questionnaire had a good clinical sensibility (comprehensiveness, clarity, face validity), pilot testing (validation) was performed with 16 independent health professionals (physicians and nurses). Finally, comments were taken into account to improve the questionnaire; and the final version was elaborated, which consisted of 21 questions in addition to demographic data questions.
The survey is summarized in Table 2. Some questions were structured on a five-point Likert scale; respondents were asked to indicate the frequency (never, rarely, sometimes, frequently, always) for each answer. For questions on motivations or obstacles to use the OPD, the respondents had to answer on the degree of importance accorded to each item (really not important, not important, neutral, important, really important). For questions on disadvantages/advantages of the OPD, the respondents had to answer on the degree of disadvantage/advantage accorded to each item (really disadvantageous, disadvantageous, neutral, advantageous, really advantageous). The survey also allowed for open-ended answers and comments for all questions.
OPD, order protocol for distress.
The study was done between September 2010 and September 2012. During this time, all the staff from different units where pediatric palliative care patients are hospitalized (except for the neonatal intensive care unit) were offered a training workshop on the use of the OPD. The workshop was highly recommended and offered during working hours but was not mandatory. The training was provided to one care unit at a time and consisted of small teaching groups. Surveys were distributed to the participants after the workshop. When the training was finished for one care unit, surveys were again distributed to all physicians, residents, fellows, and nurses working in that care unit. All health professionals were invited to answer the survey (if not previously completed), whether they had attended the worskhop or not. The whole process for one care unit lasted about two months. The respondents gave written consent to the survey, which was anonymous and completed on a voluntary basis.
Data management
A research assistant (GB) transferred all data from the questionnaires to a database (Excel). Data management fulfilled requirements of standard good clinical data management practice, and all data were treated anonymously.
Statistical analysis
Categorical variables were described by frequency distribution and expressed as percentage of completed answers. Bivariate comparisons were made using chi-square or Fisher's exact test statistics. Nonimputations were made for missing data. A two-tailed p < 0.05 was considered statistically significant. No adjustment for multiple comparisons was made. Analyses were done with statistical software SAS (SAS 9.3, SAS Institute, Cary, NC). This study was approved by the institutional review board of SJH and was funded by the Centre d'Excellence en Soins palliatifs pédiatriques of SJH.
Results
A total of 548 surveys were distributed and 258 were completed, which correspond to a response rate of 47%. Demographic data on the respondents is detailed in Table 3. Statistical analysis showed there was no significant difference in answers according to demographic data (age, gender), death of a loved one, respiratory distress at the end of life of a loved one, or attendance in the OPD workshop.
N/A, not available.
Percentages are expressed as compared to all respondents.
Subspecialties: respirology, cardiology, gastroenterology.
According to this survey, 159 respondents (82%) have taken care of at least one palliative care patient with respiratory distress/acute pain crisis in the last five years. For 40% of these respondents, it occurred in 2 to 5 of their patients, for 16% in 6 to 10 patients, and for 6% in more than 10 patients. For 97 respondents (75%), the most recent episode occurred in the last year.
Ninety percent of the respondents knew about the OPD, either through the workshop (71%), after reviewing a patient's prescriptions (36%), after a pediatric palliative care team consultation (31%), through consultation with a colleague (27%), or through the hospital pharmacy website (12%).
Since the establishment of the OPD at SJH, 27 respondents (10%) have prescribed the OPD at least once, and sometimes up to 15 times. Furthermore, 87 respondents (35%) have administered (n = 51) and/or have assisted in the administration (n = 44) of the OPD at least once, and sometimes up to 10 times. According to the experience of the respondents who have used the OPD, it was frequently (56%) or always (36%) effective in relieving the patient's symptoms. The respondents rarely (5%), sometimes (17%), frequently (33%), or always (44%) felt comfortable in administering the OPD. As for the respondents who were not always comfortable in the administration of the OPD, they chose to administer the protocol despite their discomfort (n = 21) in the majority of situations or to discuss it with another colleague (n = 25), whether nurse or physician, before the administration; no one refused to administer the OPD.
All respondents, including those who never administered the OPD, were asked what they considered the most important motivations, obstacles, advantages, and disadvantages in using the OPD. In order, the four most important motivations in using the OPD were (1) the desire to relieve patient's distress; (2) the speed of relief of distress by the OPD; (3) the intensity of patient's distress; and (4) the autonomy of the nurses in implementing the OPD. The four most important obstacles in using the OPD were (1) going against the patient's wishes; (2) going against the patient's family's wishes; (3) fear of hastening death; and (4) improper evaluation of the patient's distress. The four most important advantages of the OPD were (1) the nurse has the ability to judge when the OPD should be initiated; (2) the nurse has the autonomy to initiate the protocol before advising the physician (in order to avoid delay); (3) use of subcutaneous as well as intravenous route; and (4) the OPD can be repeated up to three times, if necessary, until evaluation by the physician. The four most important disadvantages were (1) the OPD could be used instead of a regular basic analgesia; (2) the OPD could be used for indications other than distress; (3) the OPD could be used to attempt to hasten death; and (4) the OPD could be used to alleviate suffering in the caregivers or the family.
There was a specific question (Table 2 question 16) concerning the autonomy of nurses to initiate the OPD before notifying the physician (to avoid delay). Answers are reported in Figure 1. Thirty-two percent of nurses answered that they would always feel comfortable initiating the OPD when necessary before notifying the physician, while 24% of physicians said they would always feel comfortable if a nurse initiated the OPD before notifying them, showing that physicians were less favorable to this initiative than nurses (p = 0.04). Results were also different when we compare the different care units (see Fig. 2). Nurses from hemato-oncology and intensive care units answered they would always be comfortable to initiate the OPD before notifying the physicians in 50% and 45% of cases, respectively, while nurses from general pediatric wards and pediatric subspecialties answered they would always be comfortable to initiate the OPD before notifying the physicians in only 21% and 17% of the cases, respectively, (p = 0.004).
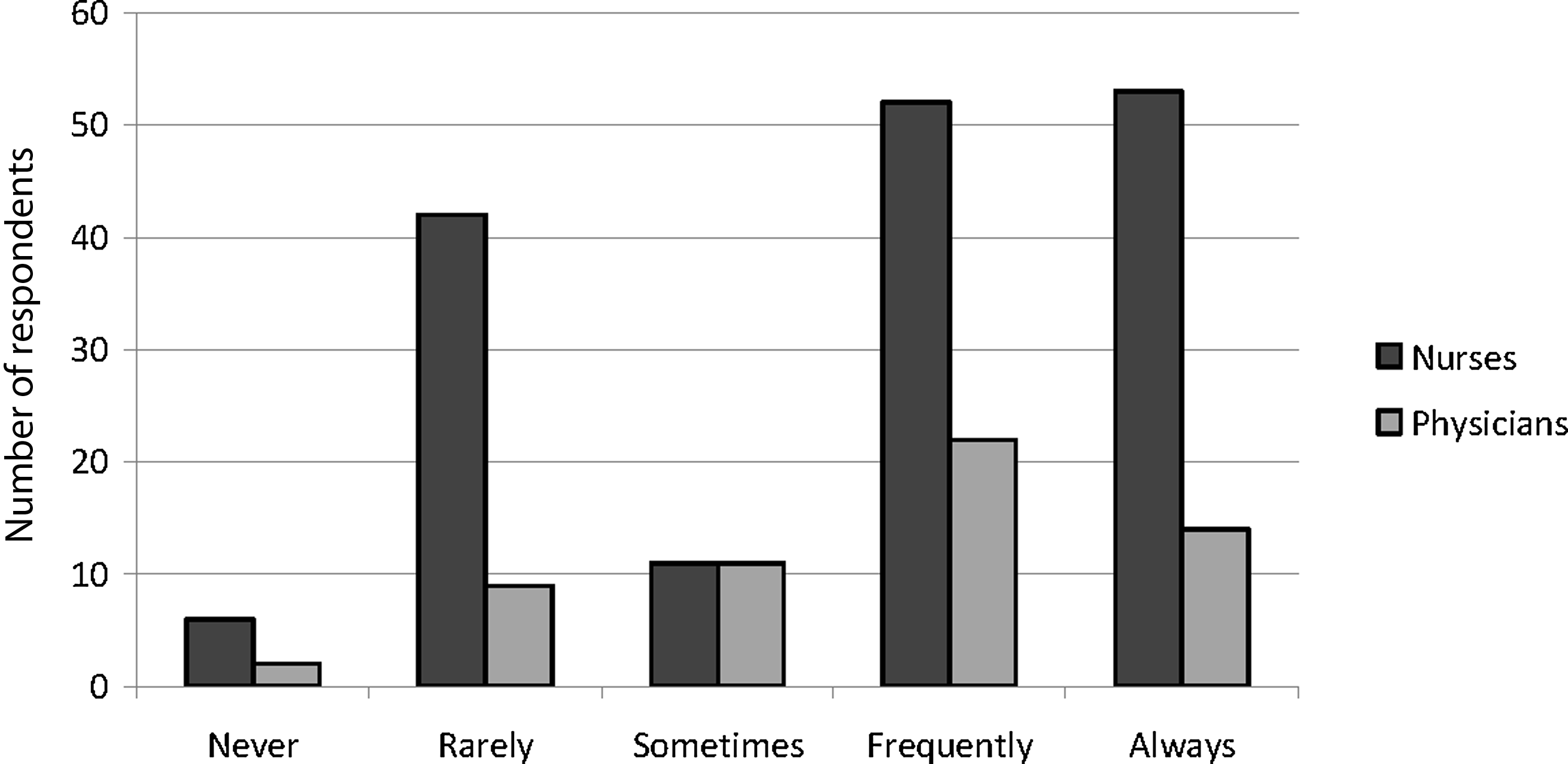
Answers to the question, “Do you feel comfortable to initiate OPD (if you are a nurse) or that the nurse initiates the OPD (if you are a physician), knowing that the physician is advised right after the first dose is administered?” (p = 0.04) OPD, order protocol for distress.

Responses from nurses of different care units to the question concerning their autonomy to initiate the OPD before notifying the physician (p = 0.004). OPD, operating protocol for distress.
The respondents (nurses and physicians) felt that the OPD was frequently or always beneficial for the patients in 99% of the cases. In one case a physician reported that the OPD was not beneficial because it was administered too late. As reported in Figure 3, nurses more frequently answered that the OPD was always beneficial (66%) for the patients compared to the physicians (36%); the difference was statistically significant (p = 0.001).

Answers from nurses and physicians to the question, “Do you think the protocol is beneficial to palliative care patients with respiratory distress or pain crisis?” p = 0.001.
Respondents answered that the OPD could never (13%), rarely (33%), sometimes (46%), frequently (7%), or always (1%) hasten death. As for responders who thought that the OPD could hasten death, they would nevertheless choose to administer it, if it was necessary. Again there were different results depending on the care units (see Fig. 4); 53% of respondents from hemato-oncology, intensive care units, and emergency room answered that the OPD would never or rarely hasten death; while 38% of respondents from pediatric and subspecialty care units gave the same answer (p = 0.03). Likewise, 14% of respondents from pediatrics and subspecialty care units answered that the OPD could frequently or always hasten death, while this answer was given in only one respondent from hemato-oncology and no respondent from the emergency room and intensive care units. The answer was also significantly different depending on professional experience of the participant; 12% of respondents with more than five years of experience answered that the protocol could frequently or always hasten death compared to 0% in the respondents with less than five years of experience (p = 0.03).

Answers of respondents from different care units to the question, “Do you think the order protocol for distress can hasten death?” p = 0.03.
Overall, 95% of respondents considered that they would use the OPD, if necessary, for a pediatric palliative care patient in the future. Respondents from pediatric and subspecialty care units answered less positively (85% and 91%, respectively) than respondents from the hemato-oncology care unit, intensive care unit, and emergency room (all 100%); the difference was statistically significant (p = 0.008).
Discussion
This study shows that in our institution most of the nursing/medical staff have taken care of at least one palliative care patient with distress in the last year. This new reality for these health care professionals and patients implies many changes in the objectives of treatment, support to family, and decision making at the bedside.
The objective of the OPD was to rapidly relieve symptoms in children undergoing palliative care. According to our survey, this objective has been reached, since the respondents thought the OPD was frequently or always effective in relieving the patient's symptoms in 92% of the cases. Furthermore respondents reported that the OPD was frequently or always beneficial for the patient in 99% of the cases. Walling et al. used an order protocol for end-of-life symptoms in adult palliative care. 17 Their protocol was also evaluated by health professionals and showed that 87% of the clinicians found it to be valuable.
The most important motivations chosen by the respondents in the use of the OPD was the desire to relieve patient's distress, the speed of the OPD to treat distress, and intensity of distress of the patient. The advantages highlighted were that the nurse could judge when the OPD was necessary, could then initiate the OPD before advising the physician in order to avoid delay, could use the subcutaneous route if no intravenous route was available, and could repeat the OPD if necessary until evaluation by the physician. All of these items are related to the importance, for health care professionals, of rapidly relieving a patient's symptoms.
In the study by Walling et al., one fourth of the physicians felt that initiation of the protocol was delayed. 17 This was reported only once in our survey. Several reasons could possibly explain this low number at SJH: (1) great emphasis is given to distress, and the OPD is prescribed as soon as judged appropriate by the palliative care team; (2) before the OPD is prescribed, the objectives of treatment and level of care are reviewed with the patient (if appropriate) and/or his or her family, avoiding these decisions/discussions taking place during acute episodes of distress; (3) the drugs used in the OPD, their indication, advantages, and side effects are always explained at the time of prescribing the OPD, so less time is spent reviewing these topics at the time of crisis by the bedside nurse; (4) for all patients with a prescribed OPD, the first three doses of medication are prepared beforehand and are ready to use (in prefilled syringes) and available in the care unit so nurses can administer them immediately; (5) systematic workshops on the OPD have been given to nurses and physicians in our institution, demystifying the use of analgesia and sedation in palliative care and explaining the objective of the OPD in distressed patients.
Although most medical and nursing staff members feel comfortable giving the OPD, important obstacles remain, such as the fear of hastening death, not evaluating the distress appropriately, or going against the patient's or his or her family's wishes. In spite of these obstacles, 95% of the respondents say they would use the OPD in the future if necessary; no respondent chose not to administer the OPD even though they felt uncomfortable. Many comments from respondents related that “it is worse to see my patient suffer than to feel uncomfortable about giving the OPD.” These responses demonstrate that health care professionals need ongoing training in palliative care, analgesia, and sedation, as well as end-of-life symptom relief. Workshops on how to support caregivers and the decision making process are essential in this specific area.18–20
Even if many studies have proven that adequate analgesia and sedation do no hasten death in palliative care patients9–14,21–23 respondents reported this as a possible disadvantage of the OPD. These myths are difficult to dissipate, and similar results have been reported in other studies.17,24,25 In a survey conducted by Houlahan et al. on the evaluation of a pediatric model for the management of pain/dyspnea/agitation at end of life, 17% of physicians and nurses worried that they might hasten a patient's death with opioids. 3 In our institution, 54% of respondents thought this was possible at least sometimes. This was seen more frequently in health professionals with more experience; it is possible that these health professionals might not have systematically attended the workshop on this topic, compared to the recently hired staff. Furthermore these health professionals might be convinced of some myths concerning the effect of opiates on causing death that are difficult to change. Lack of education is one of the many barriers to pediatric palliative care, as reported by Davies et al. 26 The concern about hastening death was also more frequently seen in respondents from the pediatric and subspecialty care units, which are units where analgesia/sedation is less frequently used and where consultations to the palliative care team are seldom used. Also, in our cohort, there are fewer patients who die in those units (30%) compared to the intensive care units and the hemato-oncology care units (70%).
Autonomy of the bedside nurse to start the medication is a key to the success of this OPD. This was also suggested by Houlahan et al.; 3 in their survey, 64% of the nurses wished that they could write the orders themselves rather than waiting for doctors. In our study, nurses were more favorable to this initiative than physicians, although answers were varied in both groups. As reported in the comments by the participants, although autonomy is seen as a great advantage to some nurses, the increased responsibility that comes with this is not always welcomed. This can be seen by the variability of responses according to the different care units; health care professionals from units where analgesia/sedation and/or palliative care are more frequently used (hemato-oncology, intensive care unit, emergency) are more favorable to this initiative than other units (general pediatrics, subspecialties). In a study evaluating circumstances of deaths of 3793 adults, one of the main factors according to the bedside nurses that could improve end-of-life care is the availability of a written protocol. 27 Nurses concluded that those procedures accepted by all staff members decrease the risk that individual opinions may influence difficult decisions and thus improve quality of patient care.
To our knowledge, this is the first article in the current literature which provides data on perceptions and personal experience of the medical and nursing staff towards the use of an order protocol for respiratory distress/acute pain crisis in pediatric palliative care patients. Our results bring important information about health care professionals' concerns with regards to the use of these protocols, autonomy of nurses in initiating the protocols, and concerns related to hastening death. Identification of these concerns is essential to achieve implementation of these protocols, which help to rapidly relieve pain and respiratory distress in pediatric palliative care patients.
A limitation of this study is the fact that it was conducted in only one center, although health care professionals from multiple and different care units answered the survey. Another limitation is the selection bias; since the study was done on a voluntary basis it is possible that only health care professionals who were interested in palliative care or the OPD answered the survey. Recall bias is another possible limitation, especially in regard to asking participants if they remember taking care of palliative care patients with distress in the last five years. Finally, few residents/fellows participated in this survey, which prevented us from analyzing the statistics in this group. The response rate in this group was very good (51%), but the low number of residents/fellows compared to other groups (nurses and physicians) is the main reason they were not compared as an independent group. Future studies specifically with this population would help us see the advantages of an OPD in how residents manage patients in palliative care and distress. Jarabek et al. has shown that introducing palliative care orders improved significantly resident comfort with symptom management in dying patients. 28
Conclusions
Data from this survey shows that respondents are in favor of using an OPD for pediatric palliative care patients at SJH and find it effective. The desire to relieve a patient's symptoms seems to be the main motivation to use the protocol. Nurses are more favorable than physicians toward initiating the OPD and then notifying the physician (in order to avoid delays). Most respondents think the OPD is beneficial for patients and would use it in the future. Repeated and continuous training related to OPD use is mandatory, especially with the high turnover rate of health care professionals in an academic center. Support of health care professionals who have to deal with these situations is essential, and should be provided through workshops and ongoing communication with colleagues and palliative care teams familiar with this context.
Future studies should emphasize other aspects of the OPD, particularly perceptions of patients/parents towards the OPD as well as the impact on a resident's knowledge of palliative care.
Footnotes
Acknowledgments
We would like to thank the following experts who helped us with validation of the questionnaire: G. Bidet, MD, Palliative Care; M. P. Coté, RN, Hemato-Oncology; L. Daoust, RN, MSc, Palliative Care; M. Duval, MD, Hemato-Oncology; N. Gaucher, MD, Emergency Room; F. Gauvin, MD, MSc, Palliative Care; C. Hervouet-Zeber, MD, Pediatrics; N. Humbert, PhD, MSc, Palliative Care; K. Houle, RN, multispecialties; M. P. Pelletier, RN, Pediatrics; A. Petti, RN, Palliative Care; A. V. Roy, MD, Pediatrics; S. Stojanovic, MD, Pediatrics; S. Plante, RN, Ethics; M. F. Vachon, RN, Hemato-Oncology.