
Abstract
Abstract
Background:
Terminal ventilator withdrawal entails cessation of mechanical ventilation to allow a natural death. There is little empirical evidence to guide the conduct of this procedure. If the process is not well conducted, patients undergoing terminal ventilator withdrawal are at high risk for experiencing significant respiratory distress.
Objectives:
Our aim was to (1) establish the feasibility of a nurse-led algorithmic approach; (2) determine differences in patient comfort between groups; and (3) determine differences in the use of opioids and benzodiazepines.
Methods:
A prospective, two-group, repeated measures, observation design was used with nurses from one medical intensive care unit (MICU) conducting the algorithm and nurses from a second MICU providing unstandardized usual care. Patient respiratory comfort/distress was measured with the Respiratory Distress Observation Scale (RDOS).
Results:
Nurses and respiratory therapists were trained to follow the algorithm in one-hour educational sessions; fidelity to the algorithm was subsequently confirmed. Fourteen patients evenly distributed by ethnicity and gender were enrolled, eight in the control MICU and six in the intervention unit. No significant differences in age, consciousness, illness severity, or baseline RDOS were found. All control patients underwent a one-step terminal extubation process. There were no incidences of post-extubation stridor in the intervention group, whereas three (38%) control patients experienced stridor. Patients in the intervention group had greater respiratory comfort compared with control patients (p<0.05). Differences in medication use were found with lorazepam favored in the control unit; morphine is recommended in the algorithm.
Conclusions:
Feasibility and proof of concept for the nurse-led algorithm were established.
Introduction
T
Patients undergoing ventilator withdrawal are heterogeneous. Some patients choose ventilator withdrawal while conscious and able to report dyspnea. 2 A majority undergoing withdrawal, however, are critically ill, cognitively impaired, or unconscious and unable to self-report dyspnea; these patients may or may not be able to experience respiratory distress depending on the severity of unconsciousness. 3 If the patient has been intubated for only a short time, subsequent extubation of the endotracheal tube is not expected to produce airway complications. In other cases, use of the endotracheal tube for more than a few days or other airway conditions such as laryngeal edema predict complications such as stridor or complete airway obstruction. 4 Therefore, the anticipated experience of the patient will vary greatly. The ideal best practice for conducting the ventilator withdrawal process across a heterogeneous population must account for variance in patients' experience and suggests that a patient-centered algorithm will provide the best guide. Development of a nurse-led algorithm recognizes and promotes the integral role of the nurse during ventilator withdrawal. Standardization of common procedures contributes to quality of care and patient safety; an algorithmic approach affords standardization while simultaneously allowing for the unique care needs of the patient.
The purpose of this pilot study was to test the utility of a novel algorithmic approach to terminal ventilator withdrawal using the following aims: (1) to establish the feasibility of patient recruitment and family consent; (2) to ascertain nurse fidelity to the algorithm after training; and (3) to ascertain proof of concept regarding differences in patient comfort, development of post-extubation stridor, and use of medications comparing the algorithmic approach with usual care.
Methods
Design
A prospective, two-group, repeated measures, observation study of patients undergoing terminal ventilator withdrawal was conducted. The two groups were: intervention (algorithmic process) versus comparison (unstandardized usual care) with at least 3 time periods of measuring patient respiratory distress.
Sample
Any adult medical intensive care unit (MICU) patient whose family members were English speaking were included. We excluded patients who were cognitively intact because negotiation about the withdrawal processes and sedation are expected under those clinical circumstances and the pilot algorithm under this testing did not include those domains. We also excluded patients undergoing organ donation after cardiac death following ventilator withdrawal.
Setting, recruitment, and enrollment
The study was conducted in two MICUs in a tertiary care hospital in the Midwest United States. The units had 12 and 16 beds, respectively. Both units had a similar 1:1 or 1:2 nurse: patient ratio. Institutional Review Board approval was obtained from the study site and from the principal investigator's (PI's) university; patients' families were requested to give written informed consent as legally authorized representatives.
Measurements
Patient characteristics
Patient demographics were obtained from the medical record and family report. Consciousness was assessed with the Reaction Level Scale (RLS85).5,6 Illness severity was quantified using the Simplified Acute Physiology Score (SAPS II).7–11 SAPS II was calculated with variables from the first 24-hour interval after MICU admission. Oxygenation performance was quantified using a peripheral oxygen saturation/fraction of inspired oxygen ratio (SpO2/FiO2) calculated using the patient's baseline (pre-withdrawal) SpO2 and FiO2. Normal SpO2/FiO2 is 98%/0.21 or 466. The SpO2 was measured by oximetry.
Dependent variables
Opioid and benzodiazepine doses were calculated as follows: (1) total dosage for the 24-hour period before ventilator withdrawal commenced; (2) pre-medication bolus; and (3) the total dose administered in the interval from the first ventilator change until the patient died. Opioid doses were converted to parenteral morphine equivalents.
Respiratory comfort or distress was measured with the Respiratory Distress Observation Scale (RDOS). An RDOS<4 signified respiratory comfort in this application. Validity and reliability psychometrics have been established.12,13
Stridor is a high-pitched airway sound produced by narrowing of the pharynx, often secondary to laryngeal edema. For this application stridor was operationalized as not audible, audible at the head of the patient's bed, audible at the foot of the patient's bed, or audible 10 paces from the foot of the patient's bed. We recorded the presence and/or intensity of stridor immediately following endotracheal extubation and every 15 minutes for the first hour after extubation.
Procedures
Training
The PI conducted training sessions on the use of the algorithmic approach with the registered nurses (RNs) and respiratory therapists (RTs) from the intervention MICU. Staff practiced the algorithm using simulated cases from video. Fidelity to the algorithm or departure from the algorithm was subsequently measured in both study units using a manualized checklist completed by a research assistant (RA).
Algorithm intervention
The MICU RN conducted the ventilator algorithm processes with support for ventilator changes and cuff-leak testing from the RT. RDOS measurements were obtained at baseline, at each ventilator change, when the ventilator was turned off, and every 15 minutes of spontaneous breathing for up to 2 hours after mechanical ventilation ceased. Observation for the development of post-extubation stridor began immediately after extubation and every 15 minutes for up to one hour after extubation.
Control group
Ventilator withdrawal was conducted by the usual personnel. RDOS assessment corresponded to the intervals as in the intervention group. In the event a single-step terminal extubation approach was used, the RA measured the RDOS at baseline, immediately after the ventilator was turned off, and every 15 minutes for up to 2 hours. Observation for the development of stridor corresponded to the procedure in the intervention unit.
The algorithm has three decision processes: (1) pre-medication; (2) withdrawal method; and (3) extubation considerations. The full algorithm with decision trees is not included with this article because it has only undergone pilot testing and is not generalizable.
Pre-medication
Pre-medication was administered if respiratory distress could be anticipated. 14 The doses in the algorithm are standard adult doses; guidelines for titration to patient effect are included.
Withdrawal method
We used rapid, staggered reduction in oxygen and ventilation in cases where the patient was likely to experience distress, as this method affords an opportunity to restore the patient to a previous ventilator setting while distress is relieved. The algorithmic guideline for treating distress entailed morphine intravenous boluses and took into consideration the timing of the peak effect of intravenous opioids.
Extubation considerations
Airway obstruction after extubation occurs secondary to laryngeal edema and is difficult to predict. A cuff-leak test entails measuring the volume of air loss when the endotracheal tube cuff is deflated prior to extubation. Air loss of less than 180 cc predicts post-extubation stridor. 4 Maintaining the endotracheal tube in the presence of a swollen or protuberant tongue or a failed cuff-leak test will minimize the occurrence of partial or complete airway obstruction and stridor, which may be a source of patient and/or family distress. Stridor is treated effectively with racemic epinephrine.15,16
Analysis
A descriptive analysis of all variables was done including measures of frequency and central tendency. Comparisons of continuous data were done with t test. Analysis of frequency of post-extubation stridor across groups was done with Pearson's χ2.
Results
Aims 1 and 2: Fidelity to algorithm and enrollment
RNs and RTs from the intervention MICU underwent training for the study in one-hour sessions. Fidelity to the algorithm was confirmed during the trial with 100% of the intervention unit nurses following all the steps in the algorithm completely. The control unit did not have access to the algorithm and conducted usual care; the processes used in the control unit departed from the algorithm. Consent to enroll in the study was obtained from 14 of 22 (64%) of the eligible patients' family members; most gave no reason for declining, one reported distrust of research and one Muslim family wanted a male RA, and one was not available.
Aim 2: Patient characteristics, respiratory comfort, and stridor
Fourteen patients enrolled in and completed the study with eight patients in the control group and six in the intervention group. There were no significant differences between patients' characteristics (Table 1). All patients in the control group had ventilation withdrawn as a terminal extubation (one-step in<1 minute) process with no cuff-leak testing. All patients in the intervention group underwent terminal weaning with an average duration time of 18 minutes (n=5), with one patient requiring 2 hours to complete the withdrawal.
NS, not significant; RLS85, Reaction Level Scale; SAPS II, Simplified Acute Physiology Score; SpO2/FiO2, peripheral oxygen saturation/fraction of inspired oxygen ratio.
All patients in the intervention group (n=5) met extubation criteria and no stridor was identified; one patient had a tracheostomy. Cuff-leak testing was not done in the control group and three (38%) patients experienced stridor; two patients displayed stridor immediately after extubation with one patient developing stridor at 15 minutes after extubation. Stridor persisted throughout the observation interval and no racemic epinephrine was administered. Of note, patients in the control group with stridor had higher average RDOS scores in the distress range compared with those with no stridor, although in this small sample the difference is not statistically significant (Fig. 1.).
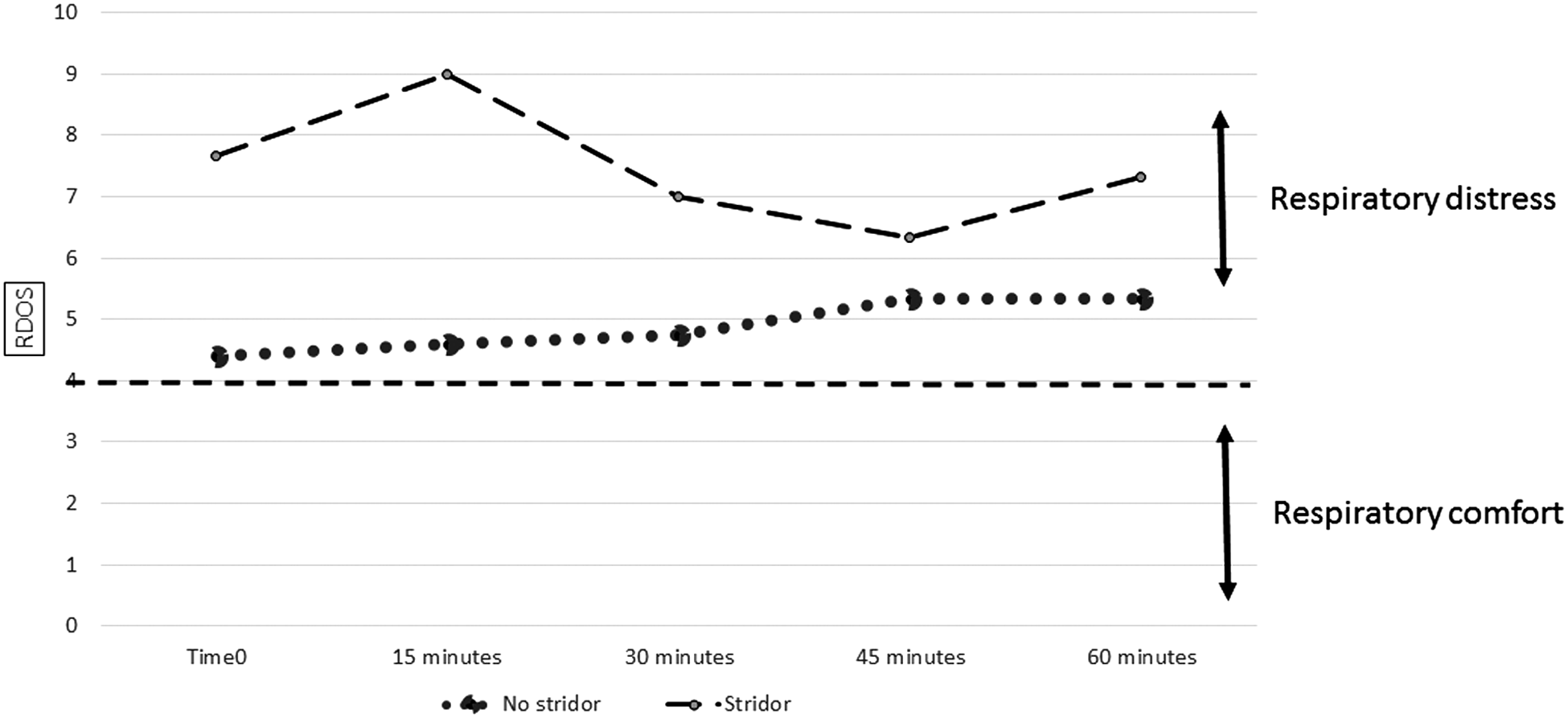
Change in Respiratory Distress Observation Scale over time among control patients with and without stridor.
All patients in the control group were pre-medicated. Of patients in the intervention group four (67%) met algorithmic criteria for pre-medication and were thus medicated. Clinically significant differences that were not statistically significant for morphine (t=0.89, p=0.40) and lorazepam (t=−1.16, p=0.27) in medication use between groups were found with more morphine administered in the intervention group and lorazepam favored in the control group (Table 2).
mg, milligrams; PME, parenteral morphine equivalents.
Differences in patient respiratory comfort between groups were found. Comparisons were possible at baseline, at time0 (which was when the ventilator was turned off), and 15 minutes after time0 (Table 3 and Fig. 2). One patient in the intervention group died during withdrawal and two others at 3 and 28 minutes after time0 obviating further comparisons.
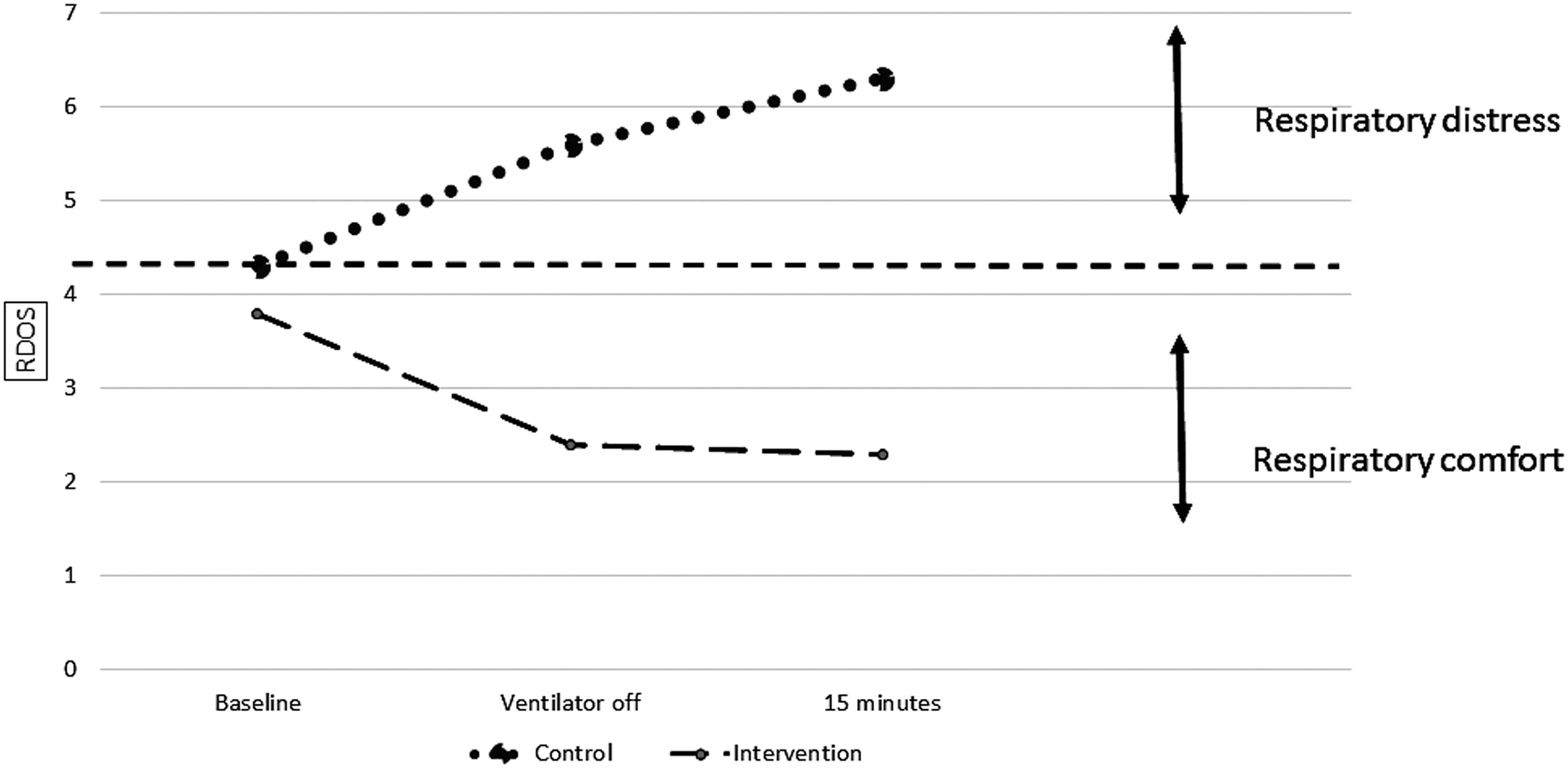
Change in Respiratory Distress Observation Scale over time.
NS, not significant; RDOS, Respiratory Distress Observation Scale; Time0, time when the ventilator was turned off.
Discussion
One aim of this pilot study was to determine if the design and method were feasible. We established that MICU RNs and RTs had the skills to conduct a nurse-led algorithmic approach to terminal ventilator withdrawal after about one hour of training. Further, we were encouraged by the high percentage of family members who provided consent for their loved one to participate. We attribute this to the rigorous RA training we did about how to conduct a discrete and sensitive approach to grieving family members. 17
Our second and third aims were to ascertain proof of concept regarding patient comfort and use of medications. This pilot study is the first to compare methods for terminal withdrawal of mechanical ventilation using a nurse-led algorithm. Although a relatively common palliative end-of-life procedure in the MICU, standardization of the process with measures of patient comfort are not evident in reported studies. 1 Treece et al. found unit support for a standardized ventilator withdrawal protocol, although patient outcomes were not measured. 18 We found statistically significant differences in patient comfort and post-extubation stridor, with clinically significant medication use differences between groups of similar MICU patients.
The algorithmic approach is predicated on recognizing that patients undergoing terminal ventilator withdrawal are a heterogeneous population with regard to consciousness, ability to experience respiratory distress, and illness severity. The algorithm afforded standardization of the ventilator withdrawal processes (distress assessment, medication use, withdrawal method, and extubation decisions) while tailoring the process to the individual patient. This contrasted sharply with the usual care unit where we found a local custom for routine pre-medication, routine terminal extubation in a single-step process, and a preference for benzodiazepines.
A rapid, staggered reduction in oxygen and ventilation affords an opportunity to cease the withdrawal when the patient displays distress and resume withdrawal after medicating the patient.1,3 A one-step withdrawal takes a patient with normal blood gases and subjects them immediately, in the face of respiratory failure, to spontaneous breathing and a high risk for respiratory distress. We found evidence for this among the control group patients who rapidly displayed a change from baseline respiratory comfort to respiratory distress, whereas the intervention patients remained comfortable.
The algorithm promotes morphine as the evidence-based drug of choice for treating dyspnea. 19 We found greater use of benzodiazepines in the control unit compared with the algorithmic approach unit; this preference for benzodiazepines was reported in a descriptive study from a long-term acute care facility. 2 Respiratory distress observed in the control group may be a factor of overuse of lorazepam and insufficient administration of morphine or may be due to the aforementioned rapidity of withdrawal or both.
No patient in the intervention group was predicted to develop stridor; the prediction was confirmed. The cuff-leak test was not used in the control unit and routine extubation was the universal method employed for ventilator withdrawal. Our results suggest that unrelieved stridor contributes to respiratory distress.
This study was a pilot and the small sample size does not afford generalization. In addition, the pilot was conducted at a single hospital and practice customs for ventilator withdrawal may vary in other settings. We established proof of concept for the positive patient outcomes associated with the algorithmic approach, which affords planning a larger, well-powered, randomized controlled trial.
Conclusions
Nurse training and subsequent fidelity to a nurse-led terminal ventilator withdrawal algorithm was established. More than half the families who were approached for consent agreed to study participation even under high emotional circumstances. This pilot test suggests that the algorithm yields better patient results regarding respiratory comfort than unstandardized usual care.
Footnotes
Acknowledgment
This work was supported by American Association of Critical-Care Nurses, Impact Research Grant #20105.
Author Disclosure Statement
No competing financial interests exist.