
Abstract
Abstract
Background:
Criteria for selecting patients with advanced cancer for palliative surgery (PS) remains poorly defined. Decision making for PS requires realistic treatment goals with well-defined criteria. Here we discuss a 71-year-old Jehovah's Witness with advanced stage renal cell carcinoma (RCC) who presented with profound anemia due to intractable bleeding from gastric metastasis. After repeated attempts with endoscopic and angiographic management, she underwent surgical palliation. Through this case, we developed 10-item evidence-based criteria for selecting patients for PS.
Objective:
The study objective was to provide a review of pertinent literature for PS and identify evidence-based criteria for patient selection. These criteria were relevant for selecting this patient with metastatic RCC and may prove beneficial for selecting advanced cancer patients for PS.
Methods:
A MEDLINE search revealed 175 publications relevant to PS. Among these, 17 articles defining patient selection criteria (PSC) were reviewed. A frequency-based analysis of each criterion was performed. Another search returned 30 cases of RCC gastric metastases from 25 published reports. Outcome analysis was determined by the Kaplan-Meier actuarial method.
Results:
Ten criteria were identified: symptom control, prognosis, preoperative performance status, quality of life (QoL), tumor burden amenable to palliation, procedure-related morbidity and mortality, feasibility of nonsurgical therapies, anticipated hospitalization, requirement for additional palliation, and cost. This patient met all inclusion criteria and underwent a successful gastrectomy. Median survival for patients with RCC gastric metastasis was 20 months.
Conclusions:
This report illustrates an example of implementation of evidence-based criteria for selecting advanced cancer patients for PS. Validation of these criteria is warranted.
Introduction
W
While palliation primarily concerns reducing or easing the intensity of disease, rather than extending overall survival, 4 much of the PS literature only assesses the extent to which PS prolongs survival. 5 Importantly, in surgical oncology, scoring systems are now well established to assist in decision making strategies for patient care.6–8 However, decision making strategies for PS remain poorly defined.2,5,9,10 Previous research suggests that patient selection is the most important factor in determining the success of surgical palliation. 11 There are few prospective studies concerning PS. 3
Here we present the case of a patient with isolated gastric metastases from renal cell carcinoma (RCC). Approximately one-third of patients have metastasis at the time of diagnosis. 12 Disease-related morbidity and mortality are usually secondary to distant metastases rather than primary disease. 13 Metastases to the stomach are rare and usually present secondary to pancreatic or other locoregional involvement. There are no clear recommendations in the literature for how patients with metastatic RCC should be treated. 14
This paper provides a comprehensive review of the literature concerning patient selection for PS and identifies 10 specific criteria to guide patient selection. These evidence-based patient selection criteria for PS are applied to the case example.
Case Report
The patient is a 71-year-old African-American woman who presented with a several month history of upper GI bleeding, fatigue, and weight loss. Her past medical and surgical history included hypertension, benign breast disease, radical left nephrectomy for RCC, left frontal lobe resection for a metastatic lesion, and IVC filter placement. One year after nephrectomy, she was diagnosed with lung and brain RCC metastases. She was treated with sunitinib malate and stereotactic radiation. Remarkably, her disease burden remained minimal and was well controlled with sunitinib malate.
When she presented with fatigue, subsequent evaluation revealed significant anemia. Her Eastern Cooperative Oncology Group (ECOG) performance status was optimal (zero). 15 Computed tomography (CT) imaging demonstrated thickening of the stomach consistent with tumor infiltration (see Fig. 1). Upper endoscopy (esophagogastroduodenoscopy, EGD) identified a 5 cm oblong, nodular, hypervascular, ulcerated mass along the greater curvature (see Fig. 2). Biopsies revealed clear-cell metastatic RCC. She subsequently underwent endoscopic epinephrine injection and hemoclip placement. The bleeding persisted and several weeks later she underwent a celiac and superior mesenteric angiogram with microcoil embolization of the left gastric, right gastric, and gastroduodenal arteries. Despite this multidisciplinary approach, she bled again. Hemostasis was achieved endoscopically as a temporizing measure. Palliative resection for definitive control of continued bleeding was considered after multidisciplinary review. Evidence-based patient selection criteria (10 points) were developed, which deemed the patient amenable for PS.
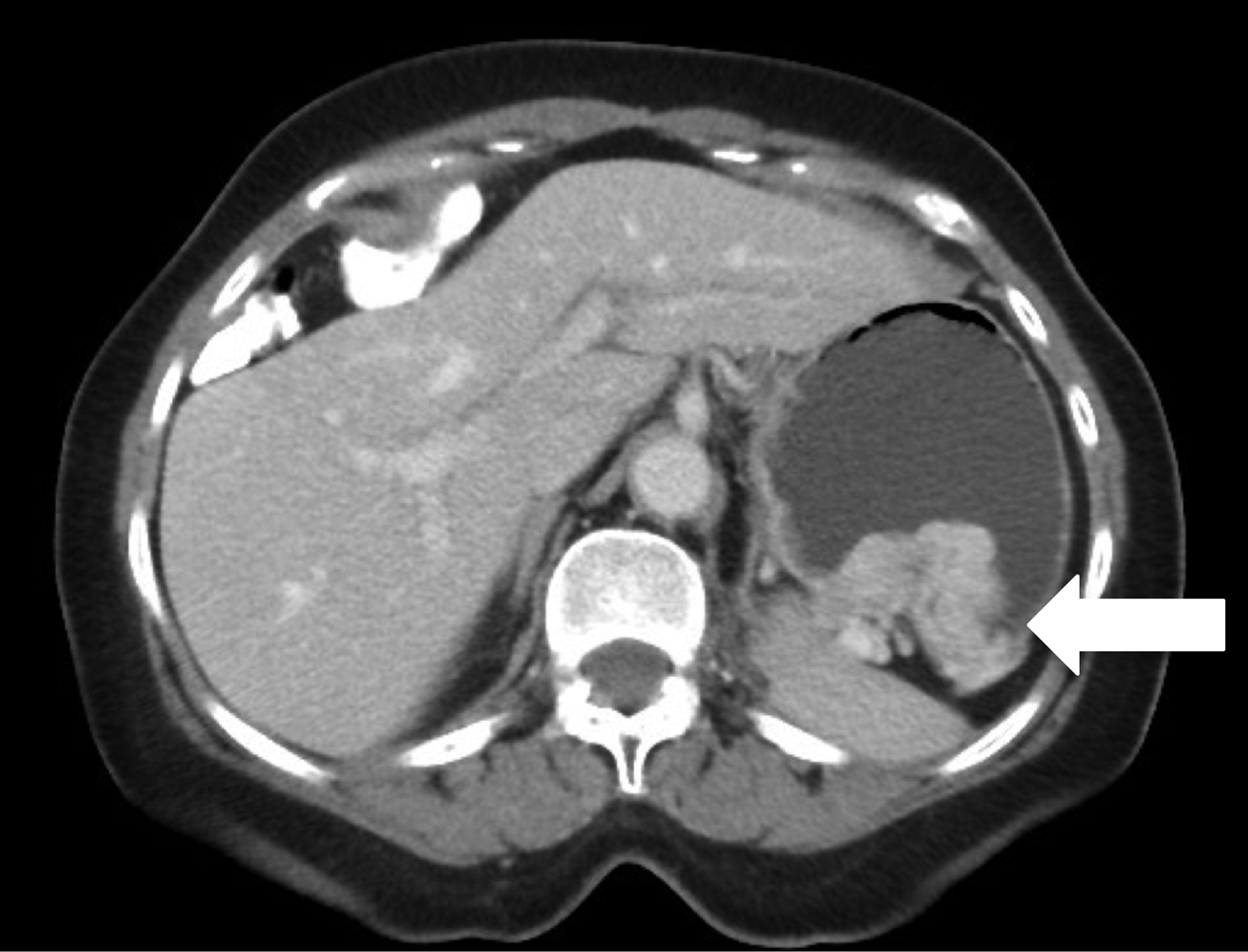
Axial computed tomography scan shows 5×3×11 cm wide, hypervascular, lobulated mass in the lesser curvature of the stomach (arrow points to mass).

Esophagogastroduodenoscopy image shows spontaneous bleeding of gastric mass.
The patient underwent an exploratory laparotomy and palliative partial gastrectomy. During the procedure, therapeutic endoscopy was used to assist in localizing the gastric mass as well as to rule out any other sources of bleeding. The metachronous metastasis involved the stomach exclusively; there was no evidence of intraperitoneal disease or local extension into the pancreas or spleen. The patient did well postoperatively. She was discharged home with no further symptoms.
Methods
A search of English-language literature published in the last 15 years (1999–2014) was performed on MEDLINE using the Medical Subject Headings (MeSH) terms “Palliative Care,” “Surgical Procedures,” and “Patient Selection.” Limiting the search to human studies, it returned 175 publications. All abstracts were reviewed and both primary and review articles that suggested specific PS selection criteria were selected (n = 14). Articles were most commonly excluded from review when the endpoint of surgical procedure was for survival benefit, not palliation. 3 References from the aforementioned papers were also explored, which identified three additional relevant publications. All selected articles were fully reviewed (n = 17) (see Fig. 3). Patient selection criteria were extracted and counted (see Fig. 4). Criteria were only included if they were recommended in at least two independent publications. We developed a scoring system based on these criteria with a range of possible scores from 0 to 10, 10 signifying most optimal suitability for PS. Each criterion was assigned a score of 0 or 1, 0 if the patient does not meet the criterion and one if the patient does meet the criterion (see Table 1). These criteria were then applied to the case example of metastatic RCC to the stomach.
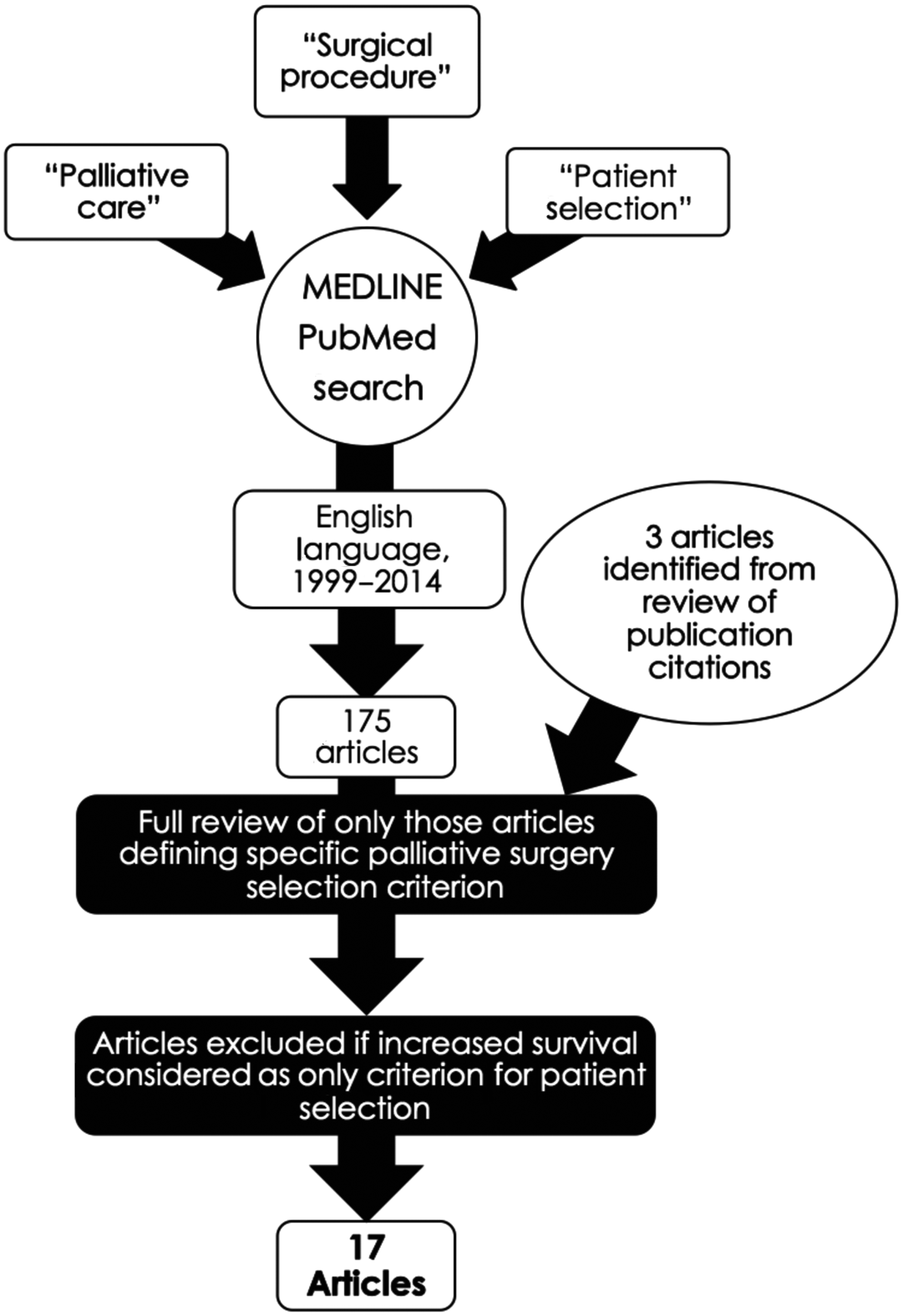
Algorithm for selection of papers reviewed regarding patient selection criteria for palliative surgery; quotations indicate MeSH terms used. MeSH, Medical Subject Headings.
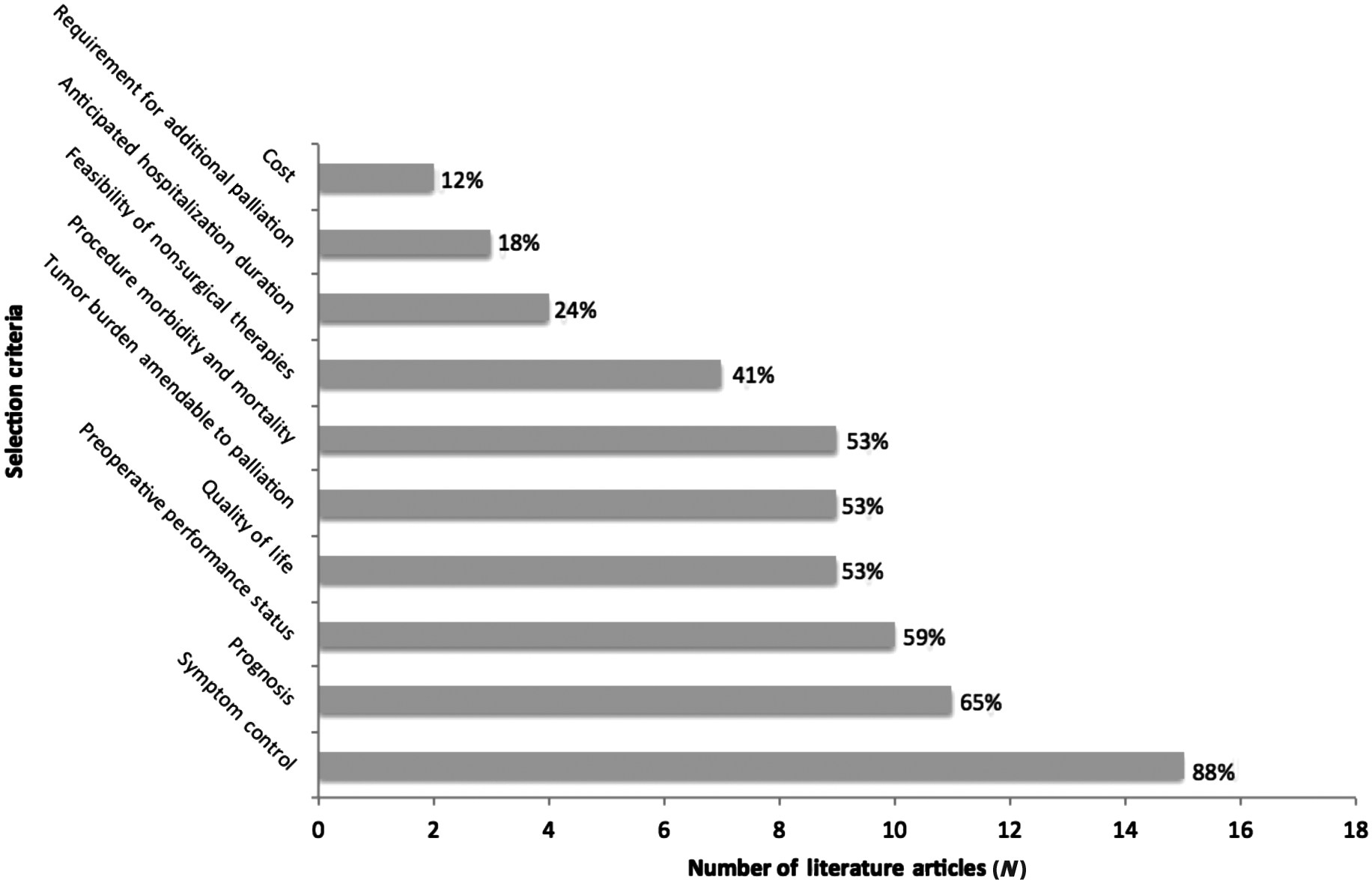
Patient selection criteria for palliative surgical procedures were derived from 17 publications. N = number of papers mentioning each selection factor; percentage of total papers reviewed.
ECOG, Eastern Cooperative Oncology Group; PS, palliative surgery; QoL, quality of life.
Concerning metastatic RCC to the stomach, another literature search was performed on MEDLINE using MeSH terms “Renal Cell Carcinoma” and “Stomach.” The search returned 15 English-language articles. References from these papers were also explored, which returned 10 additional relevant publications. These 25 publications provided a total of 30 cases in 25 published reports that specifically describe RCC metastases to the stomach.
Cumulative overall survival curve was calculated using the Kaplan-Meier method based on the length of time between identification of gastric RCC metastasis and final follow-up reported or death. The statistical analysis was performed using SPSS 22.0 (IBM, Armonk, NY).
Results
An extensive review of the English language literature generated 17 publications suggesting specific patient selection criteria for PS. These criteria included symptom control (mentioned in n = 15 of the 17 articles reviewed, 88%);3–5,10,11,16–25 prognosis or life expectancy (n = 11/17, 65%);3–5,10,11–19,21–25 preoperative performance status (n = 10/17, 59%);4,11,17–19,22–26 QoL (n = 9/17, 53%);3–5,11,20–22,24,25 tumor burden (n = 9/17, 53%);3,10,11,17,18,22–25 procedure-related morbidity and mortality (n = 9/17, 53%);5,10,16,17,19,21–23,27 feasibility of nonsurgical therapies (n = 7/17, 41%);3,11,16,18,22,23,25 anticipated hospitalization duration (n = 4/17, 24%);19,21,22,27 requirement for additional palliation (n = 3/17, 18%);5,16,27 and cost (n = 2/17, 12%)3,11 (see Fig. 4). Based on these 10 criteria, the aforementioned scoring system was assigned to our case example of metastatic RCC to the stomach. An optimal score of 10 was determined for our case example, making her an acceptable candidate for PS (see Table 2).
Summary of the application of the literature-derived patient selection to the case of metastatic RCC to the stomach presented here.
ECOG, Eastern Cooperative Oncology Group; MCS, Medical Outcome Study mental component summary; PCS, Medical Outcome Study physical component summary; PS, palliative surgery; QoL, quality of life; RCC, renal cell carcinoma.
Metastatic RCC to the stomach is a rare disease entity. A thorough search of the literature revealed 30 cases in 25 published reports.12–14,28–49 Of the cases reviewed, 22 of the patients presented with either isolated gastric metastases or gastric metastases with stable distant disease (lung and/or brain metastases) (n = 22/30, 73%). Survival data was reported for 25 patients. Kaplan-Meier cumulative survival estimates revealed a median overall survival estimate of 20 months (range 1–60 months), with a median follow-up time of six months (see Fig. 5). None of the publications reviewed provide an established treatment protocol for affected patients.
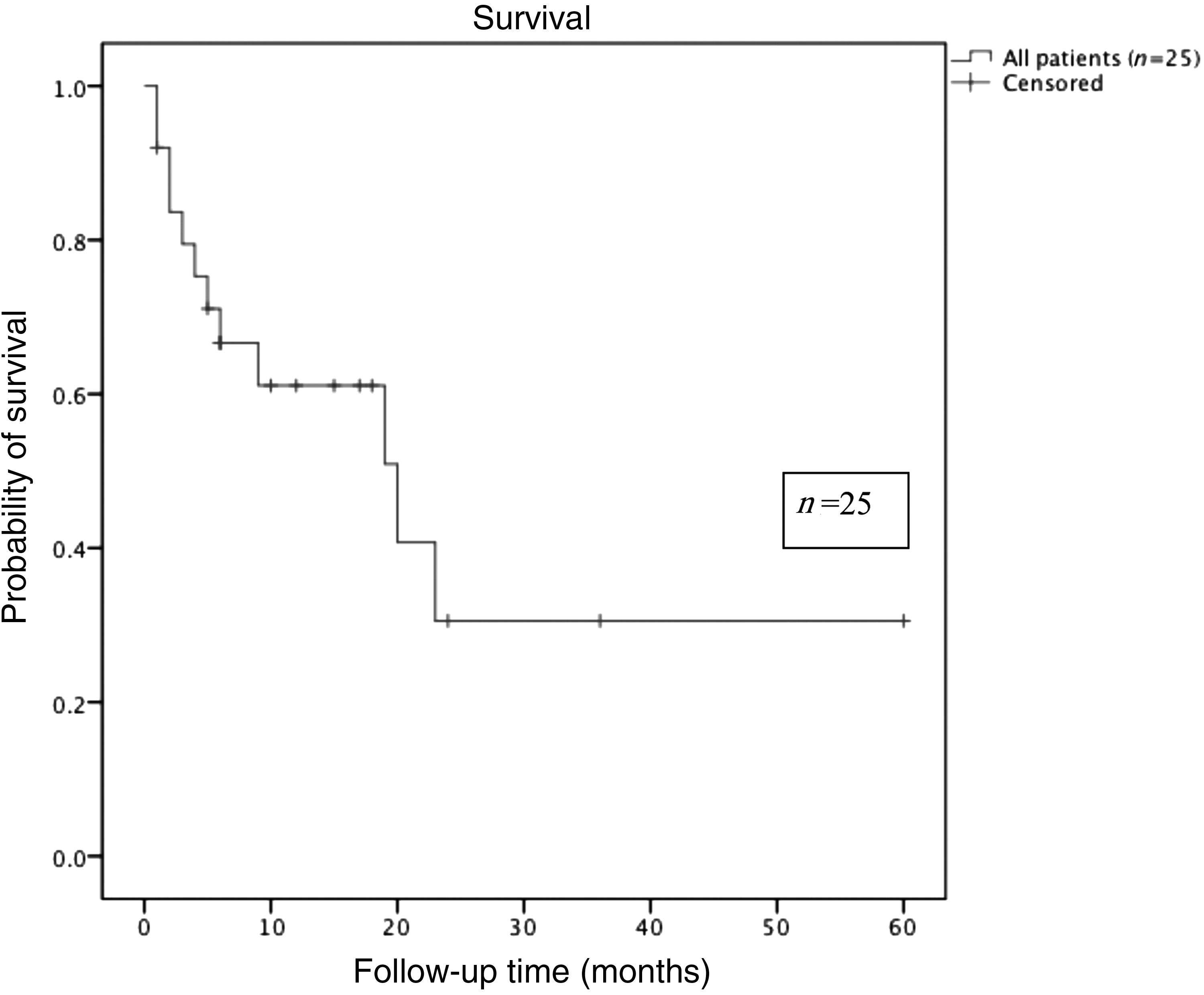
Kaplan-Meier survival curve for metastatic RCC to the stomach: Estimation of cumulative survival for 25 cases of metastatic RCC to the stomach; median overall survival estimate of 20 months (range 1–60 months); median follow-up time of 6 months. RCC, renal cell carcinoma.
Discussion
Palliation is primarily concerned with easing the intensity and reducing the symptoms of disease, with no intention of extending overall survival. 4 Surgery is a critical component of palliation in select patients. Patient selection is the most important factor in determining the success of surgical palliation. 11 While scoring systems are well established in surgical oncology for patient selection and predicting outcomes,6–8 decision making strategies for selecting patients for PS remain poorly defined.2,5,9,10 Without the benefit of established decision making strategies, inadvertent delays may occur proceeding to PS. Such delays can adversely affect the surgeon's ability to effectively intervene with palliative intent.
This paper presents the case of a 71-year-old woman with previously stable metastatic RCC status post–radical nephrectomy who presented with fatigue and anemia and was found to have a bleeding gastric metastasis. Given the lack of symptom resolution with endoscopic and angiographic interventions, surgery was the next logical therapeutic modality. Moreover, her existing anemia and inability to transfuse blood put even greater demands and risks, further substantiating the need for well-defined patient selection criteria.
As follows, each of the patient selection criteria for PS is described in detail.
Symptom control
Symptom control, including pain control, was found to be the most commonly reported factor for selecting patients for PS.3–5,10,11,16,25 In previous studies, selected patients' symptom resolution was significantly better with operative management. 11 In one particular study, symptom resolution was seen in up to 80% of patients who underwent surgical palliation. 9 Symptom control was identified as the primary factor influencing the decision to proceed with PS in this case. Our patient had active bleeding, was significantly anemic, and refused transfusion of blood products. In the proposed scoring system, a patient should receive one point if significant symptom(s) are likely to be resolved with surgical intervention.
Prognosis
As previously discussed, prognosis alone should not guide the decision to pursue a palliative surgical procedure. However, life expectancy is a relevant consideration for patient selection. 5 Based on our experience and review of the literature, at least one month of life expectancy is required to consider a patient for palliative surgery.3,11 In this case, the patient had a reasonable life expectancy (see Fig. 5). Life expectancy did not preclude palliative surgical intent, which gives a patient one point in our scoring system.
Preoperative performance status
This patient had an ECOG Performance Status equivalent to 0. 50 The ECOG Performance Status metric is an objective scale used to assess how a patient's disease is affecting their daily living. Grade 0 equates to the patient being fully active with no restrictions. Grade 1 indicates restrictions only with strenuous activities. Grade 2 equates to a patient who is able to conduct self-care but unable to work. Grade 3 indicates capacity for limited self-care only and being bed or chair bound more than 50% of waking hours. Grade 4 equates to total disability with confinement to bed or chair. Grade 5 is deceased. In our proposed scoring system, a patient should receive one point if baseline ECOG performance status is ECOG 0, 1, or 2, whereas an ECOG score of 3 or greater earns 0 points. 51
Quality of life
QoL is a general measure concerning physical, emotional, and social health. There are a number of QoL measurement tools available for use. When deciding whether or not to operate on an advanced stage cancer patient for palliation, the surgeon should consider premorbid QoL prior to the onset of acute issues requiring palliation. Those patients that have a greater premorbid QoL may stand to benefit the most from palliation. For example, a bedbound demented patient with longstanding nonhealing sacral pressure ulcers who now has a malignant obstruction is a different patient than someone who lives independently with minimal assistance with the same acute problem. Our scoring system gives more weight to palliating the latter rather than the former.
A standardized QoL measurement tool was not applied to this patient initially. However, on review of this case, such a tool was highly applicable. One such tool is the Medical Outcomes Study 36-Item Short Form Version 2 (SF-36v2), a QoL assessment tool based on work from the International Quality of Life Assessment project and the Veterans Health Survey. It is composed of eight multi-item scales (physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and mental health), combined into physical and mental component summaries (termed PCS and MCS, respectively). 52 The tool uses norm-based scoring (derived from the 1998 National Survey of Functional Health Status and designed to be representative of the noninstitutionalized, adult, U.S. population) with a mean of 50 and a standard deviation of 10 in the US general population. 53 Higher scores represent better QoL. The SF-36v2 assessment was applied retrospectively to the patient presented here. She received a PCS of 56.6 and a MCS of 62.4, which is well above the average U.S. population. In our proposed scoring system, one point is given for a score greater than the general population mean (score ≥50).
Tumor burden amenable to palliation
Tumor biology and extent of disease was also considered. The patient had clear-cell type RCC, which carries a worse prognosis than other subtypes of RCC. 54 However, her metastatic disease was well controlled on sunitinib malate and was stable for several years prior to the onset of gastric bleeding. As she had only one focus of bleeding metastasis, her symptomatic tumor burden was amenable to surgical intervention. A patient should receive one point in the scoring system if his or her symptomatic tumor burden does not preclude safe intervention and is likely to be managed by proposed PS.
Procedure-related morbidity and mortality
In a previous study concerning noncurative gastric resection, the operative morbidity and mortality were found to be 54% and 6%, respectively. 5 Procedure morbidity was considered in this case and was anticipated to be less than published data. The least invasive operative option was selected for this patient. In the scoring system, a patient should receive one point if the proposed PS has a lower anticipated morbidity and mortality than the published data. As a number of patient-, surgeon,- and institution-related factors can influence morbidty and mortality, the decision on whether a particular procedure has “acceptable” risk ultimately rests with the operating surgeon.
Feasibility of nonsurgical therapies
For this patient, her religious beliefs precluded blood transfusion as a temporizing strategy, necessitating multiple interventions, successively more invasive. Multiple attempts at endoscopic and angiographic hemostasis were not successful, which left no nonoperative options for intervention. In the proposed scoring system, one point is given if there is no alternative, nonsurgical option available.
Anticipated hospitalization
With ongoing gastric bleeding and persistent, symptomatic anemia, the patient presented here was not safe for discharge. Given her refusal of blood products, she would have faced a lengthy hospitalization if definitive intervention was not pursued. One point is given if there is anticipated decreased length of hospital stay with surgery compared to nonsurgical management.
Requirement for additional palliation
This patient was previously living independently with stable metastatic disease and there was no clear need for additional palliation. One point is given if no immediate additional requirements for palliation are anticipated.
Cost
Cost was also an applicable consideration with this case, in that if the patient did not undergo any intervention, she would remain hospitalized indefinitely, which would have incurred a significantly higher cost than if she were stable for discharge after PS. One point is given if anticipated cost of care is less with PS than without.
Important considerations
To date, there is a lack of evidence-based data to guide patient selection for PS. Clearly, PS has significant inherent risks for morbidity and mortality. 9 Therefore, patient selection is of paramount importance. 11 Secondly, the goal of PS needs to be clearly established. In our experience we try to achieve a single goal when offering PS, be it for resolution of obstruction, bleeding, or perforation. However, patient selection is always multifactorial and should be taken into account. Our evidence-based 10-point scoring system addresses a broad range of multidisciplinary concerns. We propose a scoring system to select patients for palliative surgery: Low risk would be ≥ 7 points, moderate risk would be ≥5 points, and high risk would be < 5 points. Ultimately, validation of our scoring system in a prospective study is required to determine broad applicability to patient selection for PS for advanced stage cancer. This study is currently underway at our institution. We anticipate that our study will stratify suitability into high, medium, and low for PS based on assigned scores.
Importantly, the goal of PS is for palliation of symptom(s) and not for prolongation of survival. 4 As surgical oncologists, we believe,
“Biology is King, [patient] selection is Queen. … [Surgeons] are the Prince and Princesses of the realm who frequently try to overthrow the powerful forces of the King or Queen, with some temporary apparent victories, but usually to no long-term avail.” —Blake Cady, MD. 55
We believe this distinction is important when defining clinical intent for this patient population. However, as advances in oncology and personalized approaches to cancer care develop, palliative intent may translate to survival benefit in the future.
Conclusions
This paper explores patient selection criteria for PS. We propose a set of 10 evidence-based criteria for patient selection and then apply these criteria to a patient with bleeding gastric metastasis from metastatic RCC, a rare disease entity without well-established management strategies in the literature. This high-risk, bloodless patient was selected for a palliative partial gastrectomy. This case illustrates an example of implementation of evidence-based data for selecting appropriate PS in advanced cancer patients. The 10-criteria scoring system provides a foundation for future prospective studies, one of which is currently underway at our institution. To our knowledge, this is the first evidence-based scoring system applied for patient selection in PS.
Footnotes
Acknowledgments
We appreciate the willingness of the patient to be featured in this publication. Our thanks also to Janelle Kennedy, RN, from the Bloodless Medicine Center who played an advisory role with regards to the management of a bloodless patient. Senior author, WBB, acknowledges Daniel G. Coit, MD for his insight and expertise in the palliative management of patients with advanced cancer.
Author Disclosure Statement
All authors are in agreement with the content of this manuscript. No competing financial interests exist for any authors.