
Abstract
Abstract
Background:
Many patients with cancer involving the respiratory system suffer from the frequent recurrence of significant, submassive hemoptysis, which may result in invasive procedures, hospital stays, and a reduction in quality of life. Currently, there are no widely accepted noninvasive therapeutic options. Few case studies have looked at the benefit of tranexamic acid (TXA) as a noninvasive therapy in the treatment of hemoptysis.
Methods:
A patient with an invasive airway malignancy presented to the emergency department with substantial hemoptysis. A nebulized TXA solution was used as a noninvasive therapy to control the hemorrhage.
Results:
The patient's hemoptysis resolved fifteen minutes after the nebulized TXA therapy was initiated. There were no known adverse events.
Conclusion:
Nebulized TXA seems to be a safe, effective, and noninvasive method for controlling, or at least temporizing, hemoptysis in select patients. Nebulized TXA may be useful as a palliative therapy for chronic hemoptysis and as a tool in the acute stabilization of hemoptysis.
Introduction
N
Tranexamic acid (TXA), a synthetic antifibrinolytic agent, is commonly used during surgical procedures to prevent excessive blood loss. 13 Many studies have evaluated its use to treat various bleeding complications via oral, intravenous, and topical administration, but few have analyzed its potential benefit in nebulized form.9,14–18 A small number of case reports have analyzed the effectiveness of TXA in patients with hemoptysis in a controlled environment.9,14,15 However, this is the first case report describing the use of nebulized TXA in an acute care setting.
Case Presentation and Discussion
A 46-year-old cachectic man with a history of stage IV piriform sinus and thyroid squamous cell carcinoma presented to the emergency department with hemoptysis per tracheostomy tube. Chart and imaging review revealed that the patient's malignancy invaded the airway above the tracheostomy site, and that he presented to our emergency department for the same problem multiple times in the past. He had undergone two cycles of palliative chemotherapy, the last of which was two weeks prior to presentation. His initial vitals were temperature of 98.8° F, blood pressure of 132/83 mmHg, heart rate of 105 beats per minute, respiratory rate of 21 breaths per minute, and oxygen saturation of 99%. The patient was in moderate respiratory distress, repeatedly coughing up small amounts of projectile blood through his tracheostomy tube. Direct pressure was applied to the tracheostomy site and sternal notch, and the cuff on the tracheostomy tube was hyperinflated in an attempt to tamponade the bleeding. The hemorrhage did not resolve. His oropharynx would intermittently fill with blood that he would spit up. The bleeding was likely coming from his known invasive laryngotracheal tumor above his tracheostomy site. Endotracheal or endobronchial intubation was not indicated, since the patient was oxygenating and ventilating well. The patient was placed on oxygen via a nonrebreather mask at 15 liters per minute, and intravenous access was established. A portable chest x-ray showed the tracheostomy tube in proper position and was otherwise unremarkable. The patient had a hemoglobin of 9.3 g/dL, platelet count of 24,000/μL, and an INR of 1.6. The patient had 100 ml of hemoptysis over the first hour.
We decided to try nebulized TXA as a temporizing solution, given TXA has been shown to reduce or resolve bleeding from mucosal surfaces.9,14–18 One case report described using 500 mg TXA orally three times a day for hemoptysis, where the morning dose was increased to one gram and bleeding resolved after one week of therapy. 9 Solomonov et al. used either a bolus of 500 mg/ml TXA through a bronchoscope or aerosolized 500 mg/5 ml 3–4 times a day, and in most cases bleeding resolved within minutes. 14 We chose to prepare a 10 mg/ml solution by diluting one gram of TXA intravenous formulation in 100 ml of 0.9% normal saline. The TXA solution was nebulized and delivered to the patient's mouth and tracheostomy tube via facemask (see Figs. 1 and 2). The hemoptysis completely resolved over a period of 15 minutes with continuous nebulized TXA solution. We delivered the entire one gram of TXA via continuous nebulizer over the course of 30 to 45 minutes, even though the bleeding had resolved. ENT was consulted and performed flexible fiberoptic laryngoscopy showing a malignant airway wound above the tracheostomy as the likely culprit, which was no longer bleeding. The patient was transfused with one unit of platelets. His hemoglobin and vital signs remained stable. There was no recurrence of hemoptysis while he was boarding in the emergency department. The patient was admitted to the medical intensive care unit for airway observation and evaluation for interventional radiology bronchial artery embolization.
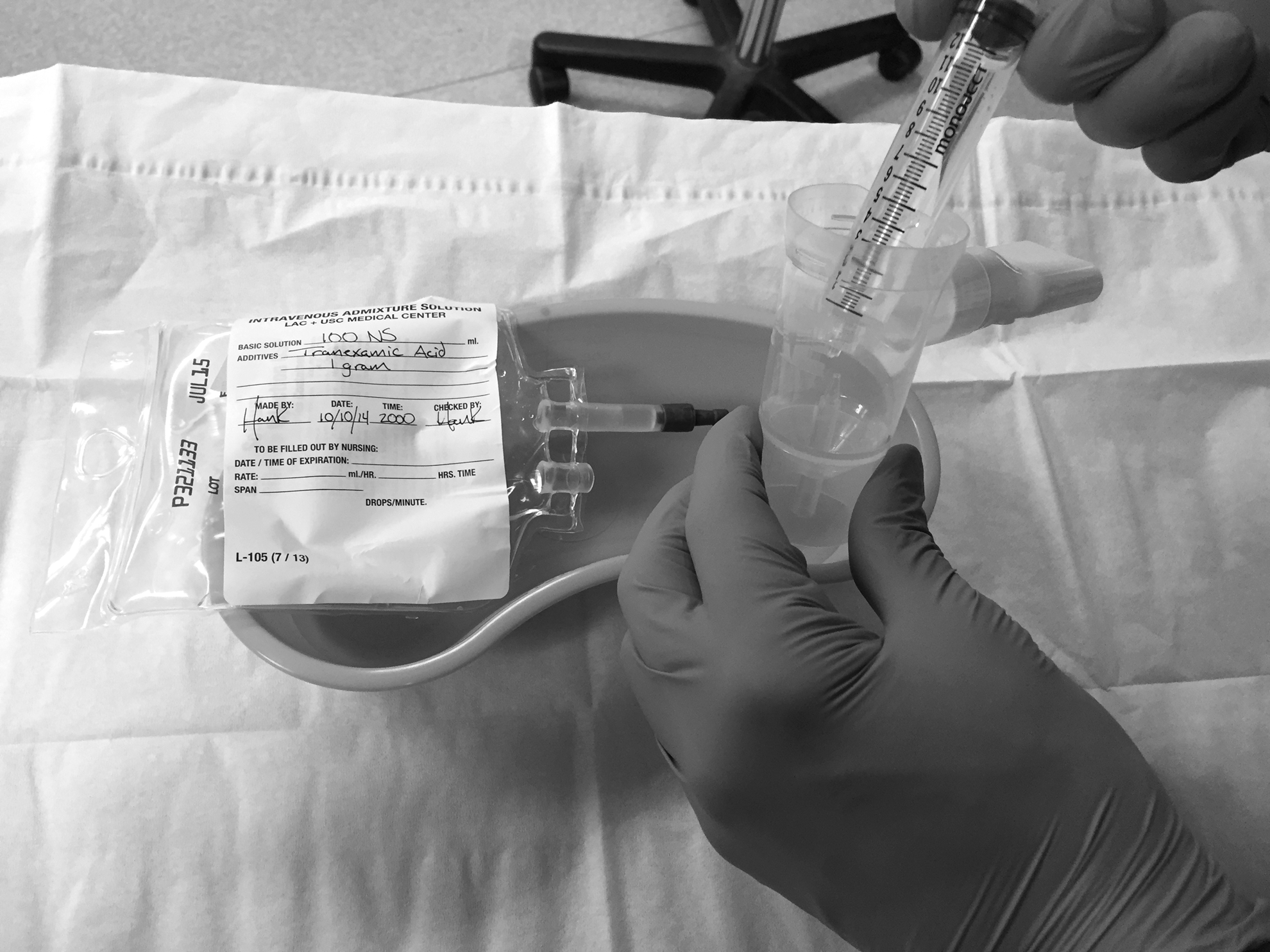
10 mg/ml tranexamic acid (TXA) solution being placed in nebulizer cup.

Patient receiving continuous nebulized 10 mg/ml tranexamic acid (TXA) solution via facemask.
Conclusion
Chronic hemoptysis can cause significant morbidity, and if the bleeding becomes substantial it often requires the use of acute care services. Management in the acute setting is primarily limited to supportive care secondary to the inability to directly identify the source of bleeding. Nebulized TXA has the potential to be a noninvasive therapy for hemoptysis, a temporizing agent for significant hemoptysis until definitive intervention can be arranged, and a hemostatic agent for bleeding encountered during bronchoscopy. In patients that are near the end of life and do not desire invasive procedures or surgeries, nebulized TXA may be an attractive palliative option.
TXA is inexpensive and has a favorable safety profile. There were no reported side effects in the case series using aerosolized TXA. 14 Our patient did not experience any known adverse effects. Side effects appear to be rare with TXA use in general, but there have been reported seizures that are most common in patients undergoing cardiac surgery, patients postcardiopulmonary bypass, and patients who were mistakenly given TXA intrathecally. 19 Currently there is no evidence to suggest that TXA increases the risk for thromboembolic events (e.g., myocardial infarction, stroke, pulmonary embolism), but there is a theoretical risk based on its mechanism of action. 19 One must also consider the possibility of bronchospasm when TXA is delivered via nebulizer, but thus far this has not been shown to occur. Other minor side effects include gastrointestinal disturbance, allergic skin reaction, and visual disturbance. 19 In retrospect, if we used a more concentrated TXA solution similar to the 500 mg/5 ml preparation used by Solomonov et al., it would have likely been safe, and we may have reached hemostasis more quickly. 14
In patients with significant active hemoptysis, it appears that the benefit tends to outweigh the rare risks associated with TXA use. Complications are more common and severe in patients undergoing invasive procedures or surgeries to identify and treat the bleeding.1,2,7–12 That being said, there are patients that would not do well with our conservative approach, mainly those with life-threatening hemoptysis who require emergent invasive or surgical interventions.
This case report describes a novel noninvasive therapy for hemoptysis. We believe that nebulized TXA has the potential to be useful as both a palliative option in chronic hemoptysis and as a directed therapy for use in acute care. A prospective trial is needed to determine the efficacy, safety, and optimal dose of nebulized TXA in treating hemoptysis.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.