
Abstract
Abstract
Background:
The extent of unmet need for palliative care in U.S. hospitals remains largely unknown. We conducted a multisite cross-sectional, retrospective point prevalence analysis to determine the size and characteristics of the population of inpatients at 33 U.S. hospitals who were appropriate for palliative care referral, as well as the percentage of these patients who were referred for and/or received palliative care services. We also conducted a qualitative assessment of barriers and facilitators to referral, focusing on organizational characteristics that might influence palliative care referral practices.
Methods:
Patients appropriate for palliative care referral were defined as adult (≥18 years) patients with any diagnosis of a poor-prognosis cancer, New York Heart Association class IV congestive heart failure, or oxygen-dependent chronic obstructive pulmonary disease who had inpatient status in 1 of 33 hospitals on May 13, 2014. Qualitative assessment involved interviews of palliative care team members and nonpalliative care frontline providers.
Results:
Nearly 19% of inpatients on the point prevalence day were deemed appropriate for palliative care referral. Of these, approximately 39% received a palliative care referral or services. Delivery of palliative care services to these patients varied widely among participating hospitals, ranging from approximately 12% to more than 90%. Factors influencing differences in referral practices included nonstandardized perceptions of referral criteria and variation in palliative care service structures.
Conclusion:
This study provides useful information to guide providers, administrators, researchers, and policy experts in planning for optimal provision of palliative care services to those in need.
Introduction
T
The delivery of palliative care services has become a practice standard in high-performing health care organizations. Multiple certification, accreditation, and training options exist. 3 Efforts to expand palliative care services through new care delivery and value-based payment models are evolving as a result of the Affordable Care Act of 2010, and the development of standardized measures13,14 allows assessment of care effectiveness. However, research to support the growth of the field and to guide delivery model development is in its early stages.
One as yet unanswered question concerns the extent of unmet need for palliative care in the United States. Estimates of the prevalence of patients admitted to intensive care units (ICUs) and a cancer center who met at least one clinical characteristic suggestive of palliative care needs have ranged from 14% to 88%.15–18 Studies from Europe yielded similar results.19,20 It is estimated that U.S. palliative care teams care for 4%–7% of annual hospital admissions, or approximately 6 million Americans. 2 The level of uptake around the world varies substantially.16,17,20–24 Potential barriers to the provision of palliative care services have been well documented25–32 and include the quality of communication among providers25,27–32 and varied perceptions about what palliative care is.30–32 The impact of organizational structural factors has not been as well studied.
To improve our understanding of the current demand for inpatient palliative care services and the reasons for varying palliative care referral practices, our study aimed to (1) estimate the prevalence of U.S. hospital inpatients who, based on diagnostic triggers, are appropriate for palliative care referral and to describe their demographic and disease-related characteristics; (2) determine the proportion of these patients who receive a referral for palliative care consultation; and (3) explore the role of organizational characteristics in influencing palliative care referral.
Methods
Study design
A cross-sectional, retrospective point prevalence design was used to estimate the size and determine the characteristics of the population of U.S. hospital inpatients who, based on a set of diagnostic triggers, were determined to be appropriate for palliative care referral.
Data were obtained from the University HealthSystem Consortium (UHC) Clinical Data Base/Resource Manager™ (CDB), a large administrative database to which UHC members submit comprehensive administrative data files. The CDB includes primary and secondary diagnoses using International Classification of Diseases, Ninth Revision (ICD-9) 17 codes. UHC's principal members include approximately 120 U.S. academic medical centers with an average of 647 acute care beds delivering tertiary and quaternary care across the country. Thirty-three UHC member hospitals participated in the study (Appendix A).
Study definitions
The definition of patients appropriate for palliative care referral was developed to align with definitions used by other researchers in the field (C. Grudzen, personal communication, May 12, 2014). 33 We included adult patients (≥18 years) with any diagnosis of a poor-prognosis cancer (ICD-9 codes listed in Appendix B) 34 ; advanced congestive heart failure (CHF) as evidenced by documented New York Heart Association 35 class IV or other classification of advanced heart failure, including intensive cardiac interventions (e.g., left ventricular assist device [LVAD]), or ejection fraction <35%; or advanced chronic obstructive pulmonary disease (COPD) as evidenced by documented oxygen dependency/chronic oxygen use, or forced expiratory volume in 1 second (FEV1) <30%.
The CDB was used to identify patients meeting diagnostic triggers who were admitted to, had inpatient status, died, or were discharged from participating hospitals on Tuesday, May 13, 2014. The date was randomly selected from all days (excluding weekends and holidays) in May 2014, the most recent month for which complete data were available in the CDB at the time the study was begun.
Each participating hospital was provided with a list of patients meeting diagnostic criteria on the prevalence day: either all patients meeting criteria or a randomly selected sample of 50 patients, if preferred. Data elements collected from the CDB included ICD-9 diagnosis codes for all diagnoses, age on admission, race, gender, payer type, admission source, do-not-resuscitate (DNR) status, discharge disposition, and presence of the ICD-9 code V66.7 (palliative care). Given that the ICD-9 diagnosis codes for CHF and COPD do not identify disease stage, a designee from each hospital reviewed charts using a study-specific data collection tool to determine eligibility for inclusion in the study cohort. Chart review was also used to collect data on palliative care referral, consultation, and service provision. Chart reviewers were provided with a detailed data collection guide (Appendix C; Appendices C–F are available online at www.liebertpub.com/jpm), a prestudy training call, and ongoing access to study personnel. All participating hospitals received individualized poststudy profiles reporting their site-specific results (Appendix D).
Statistical analysis
We used descriptive statistics for continuous data and percentages for categorical data. The percentages of patients identified as meeting the study definition were used to extrapolate to the total number of inpatients from participating hospitals to determine the overall prevalence of patients appropriate for referral. To evaluate associations, we used χ2 tests for categorical variables and t-tests for continuous variables.
Qualitative study design
We next conducted a qualitative study to understand barriers and facilitators to early palliative care referral better in the inpatient setting. We developed two semi-structured interview guides (one for palliative care teams and one for physicians and nurses) based on a review of the literature and input from three palliative care experts (L.C., C.G., M.N.), focusing on organizational characteristics such as program structure, culture, and communication practices (Appendices E and F). Purposive sampling was used to recruit four of the academic medical centers that participated in the quantitative phase of the study, based on characteristics of interest (e.g., palliative care provision at the high or low end of the range, atypical service delivery patterns). Phone interviews were conducted with a multidisciplinary palliative care team and frontline physicians and nurses from each of the four hospitals. Seven physicians and six frontline nursing staff from areas including cardiology, intensive care, and oncology, as well as four multidisciplinary palliative care teams, were interviewed between December 2014 and January 2015. All interviews were recorded and transcribed. Transcriptions were coded independently by two UHC researchers using accepted qualitative emerging themes methods, and agreement was reached on themes and findings.
The quantitative and qualitative arms of the project both received determinations of exemption from Institutional Review Board review under 45 CFR 46.102(d) by Western Institutional Review Board.
Results
Thirty-three UHC member hospitals participated in the study (27% of invited hospitals), including 29 academic medical centers, 3 affiliated general member community hospitals, and 1 stand-alone cancer facility (Appendix A). These hospitals were from 19 states, and had an average of 680 beds. All participants had submitted complete administrative data to the CDB for the second quarter of 2014 and had palliative care consult services in place. Six hospitals voluntarily reviewed all eligible charts and the remainder reviewed a random selection of 50 charts. A total of 2,119 charts were reviewed for the study (34.2% of the total that would have been reviewed if each participant had reviewed all eligible charts). These patients had a total of 2,618 study inclusion ICD-9 diagnoses (Appendix B); those meeting study criteria are shown in Figure 1.
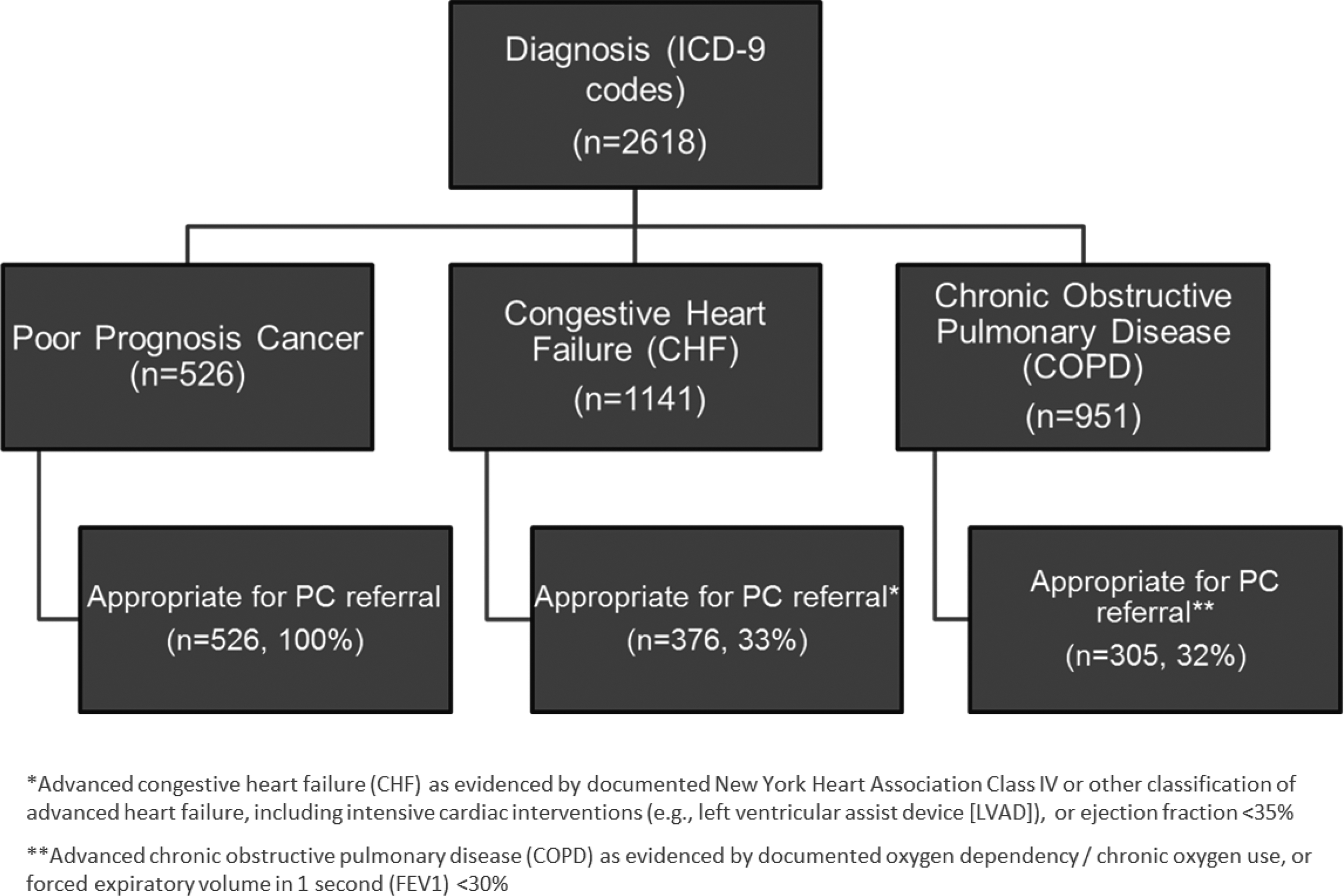
Diagnoses meeting study criteria for advanced disease and appropriate for palliative care referral.
Approximately 19% of all inpatients hospitalized in the 33 participating hospitals on May 13, 2014, met the study definition of being appropriate for palliative care referral. Among hospitals, this ranged from 9.8% to 37.3%; three-quarters of the hospitals had prevalence rates between 15% and 21%. Of these patients, 42.3% had a diagnosis of poor-prognosis cancer only, 29.5% advanced CHF only, 21.7% advanced COPD only, and 6.5% two or more conditions.
Among those appropriate for referral, 29.8% received a referral and 31.6% received palliative care services, although in some cases these services (such as physical therapy or psychological counseling) were provided without a referral to or consultation with the palliative care team. The majority of those appropriate for referral—60.9%—received neither a referral nor services (Fig. 2). Patients with two or more conditions were most likely to receive a palliative care referral (40.5% versus 35.8% for patients with poor-prognosis cancer only, 26.1% for patients with advanced COPD only, and 21.6% for patients with advanced CHF only).

Prevalence and palliative care referral and service delivery rates of patients appropriate for referral.
Palliative care referral rates varied widely among hospitals (range, 12.5% to 58.8%; median, 28.3%), as did the mix of referred patients by diagnosis (Fig. 3). The proportion of patients receiving referrals was fairly consistent across age groups, with the exception of patients over the age of 84, who were referred more often (Fig. 4). Rates of service delivery also ranged widely among hospitals, from 11.5% to 95.0%. Services provided are shown in Figure 5.
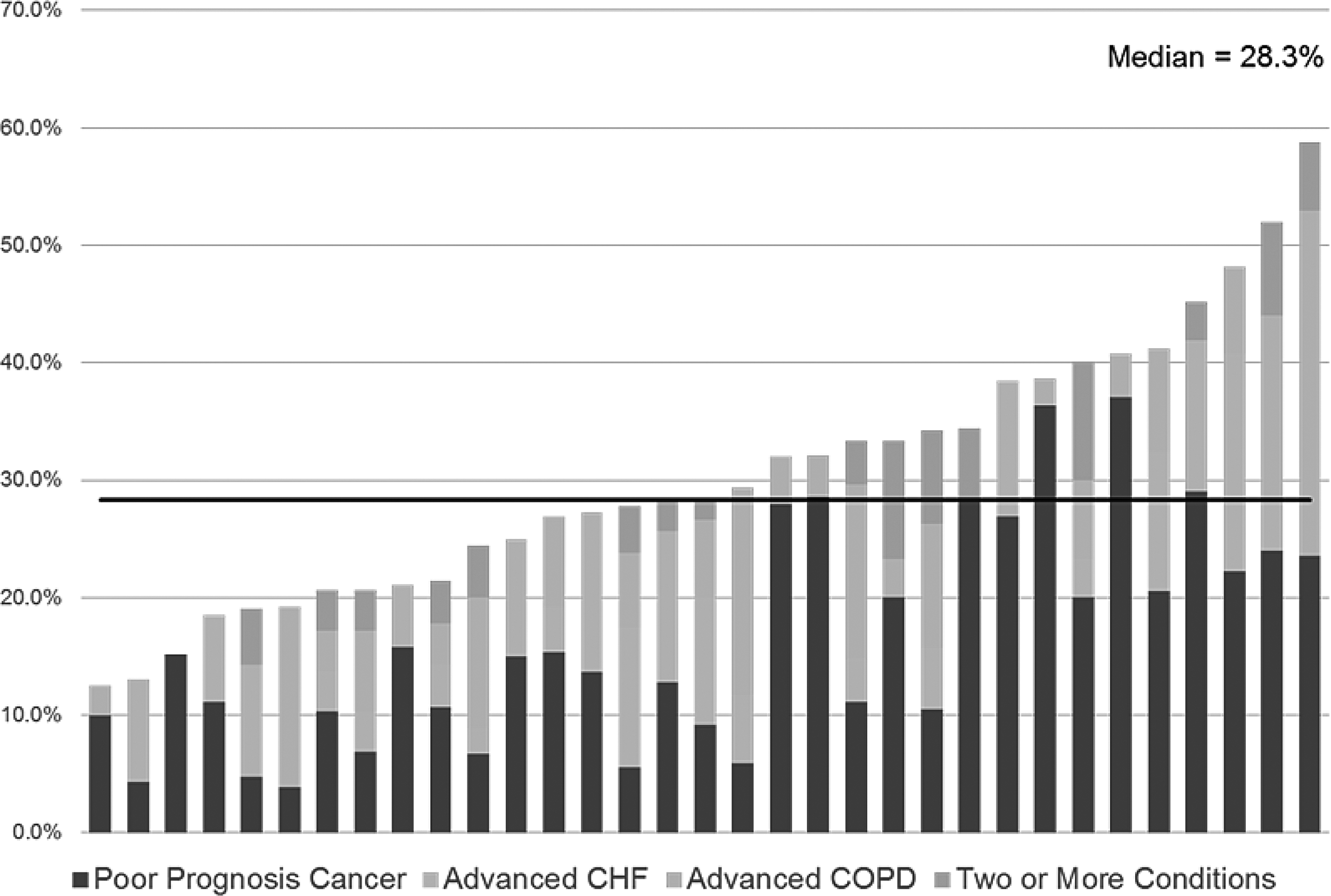
Proportion of patients appropriate for referral who received a referral by hospital by diagnosis.
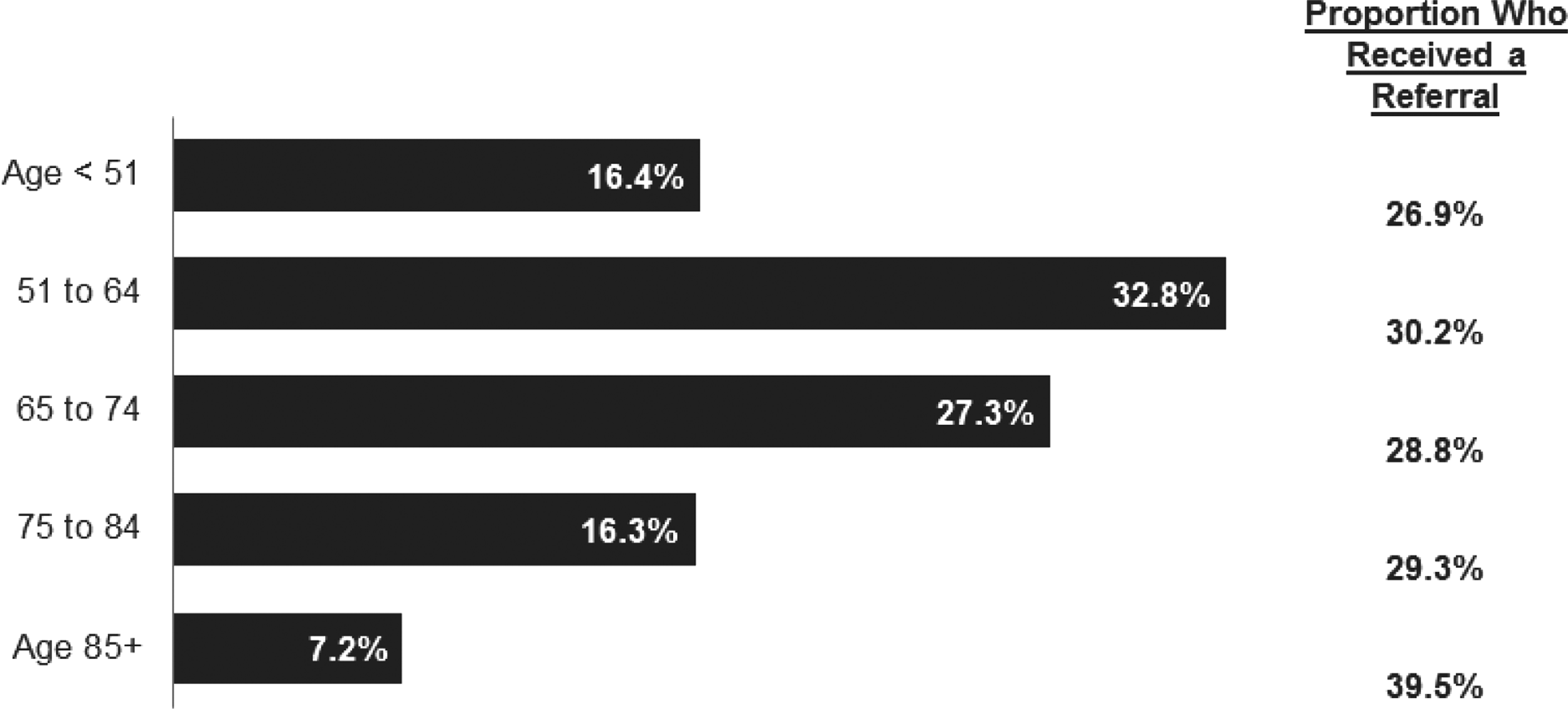
Distribution of patients appropriate for palliative care referral by age group.

Proportion of patients who received palliative care services by type of service (includes only patients for whom service data were reported).
Referral practices varied by U.S. geographic region. We found that 36.4% of patients appropriate for referral received a referral at hospitals located in the Northeast, compared with 31.9% at hospitals in the West, 25.8% in the South, and 25.3% in the Midwest (p ≤ 0.05 comparing Northeast and South and comparing Northeast and Midwest; Appendix A).
Of patients appropriate for referral, almost 80% had either Medicare (57.3%) or commercial health care (22.2%) coverage. Nearly 9% died during their study admission, 7% were discharged to hospice, and 54.8% were discharged to home. Only 29.1% had a DNR order in place (Fig. 6). Patients with DNR orders and patients who were discharged to hospice or who died during the study admission were more likely to have received a referral (p ≤ 0.05 for both).
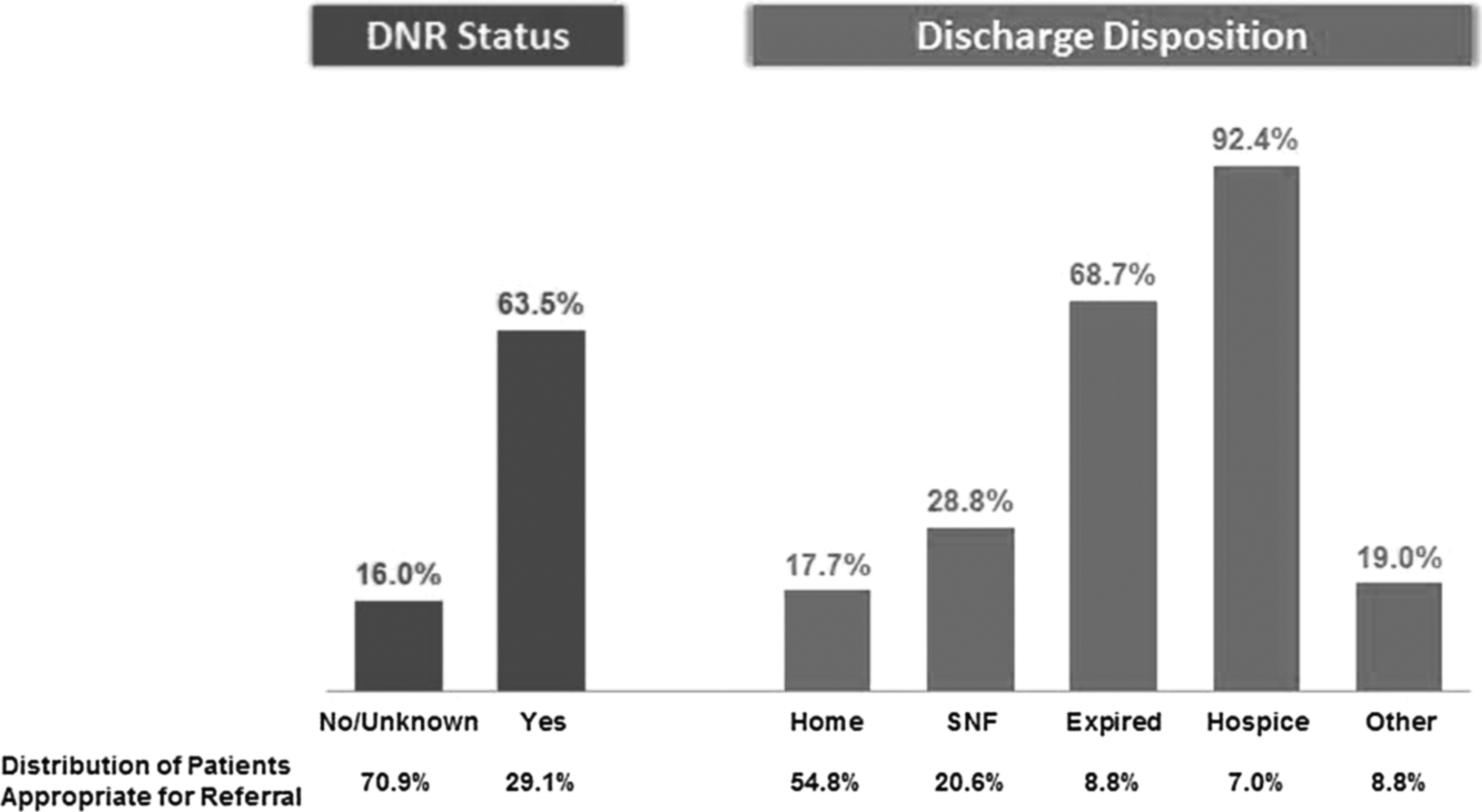
Referral rates of patients appropriate for referral.
A review of coding practices revealed that of the 29.1% of patients with a documented DNR order, 67.8% had a documented ICD-9 V49.86 (DNR) code, and of the 26% of patients reported to have received a palliative care consult, 47.6% had a documented ICD-9 V66.7 (palliative care encounter) code (range, 0%–100%; median 50%)
The qualitative phase of the study elicited barriers and facilitators to palliative care referral in the inpatient setting. Four major barriers were identified. 1) There was no standard definition of palliative care—even within organizations. Criteria for referral were subjective and clinicians varied widely in their referral practices. Available resources influenced perceptions as well; in hospitals with inpatient palliative care units, palliative care was seen as an option for discharge disposition for patients thought to have a life expectancy of 2 weeks or less. 2) Some nonpalliative care specialists were reluctant to consult palliative care because of long-standing relationships with patients and their desire to manage end-of-life care independently. 3) While it was recognized that training is necessary for clinicians to gain skills in primary palliative care, educational opportunities varied and were rarely mandatory. 4) Academic medical centers have a mission of providing advanced specialty care and access to cutting edge therapies that may limit patients' and families' acceptance of not “doing everything.”
Identified facilitators were: 1) Time and history: Referrals increased over time as teams developed relationships with frontline physicians and physicians became aware of the value of palliative care services. 2) Palliative care teams were seen as expert at handling complex symptom management and at resolving difficult patient and family dynamics and were called in for complicated cases, even by clinicians experienced at handling end-of-life care. 3) The support of palliative care services by hospital leadership who recognize its role in achieving other strategic goals increased program visibility and adoption. 4) Increasing public awareness and appreciation of palliative care. 5) Academic medical centers' mission of providing patient-centered care, setting the standard for performance on quality and financial outcomes, and educating the next generation of clinicians.
General findings included: 1) End-of-life care was frequently delivered by nonpalliative care specialist providers (e.g., oncologists, intensivists) independently of the palliative care team. 2) Referrals were seen as what is done when there are no other options for the patient and came near the end of life. 3) Perceptions of organizational capacity varied. While palliative care teams reported feeling understaffed, frontline providers reported that palliative care teams were highly responsive, spent ample time with patients, and provided excellent service. 4) Palliative care teams typically operate on a traditional consult service basis, relying on referrals and providing input only on the issues on which they are consulted.
Discussion
Our findings indicate a large unmet need in U.S. hospitals for the provision of palliative care services to patients with serious, life-limiting illnesses. This gap in care is in some ways related to the availability of palliative care resources; every palliative care team interviewed for the study reported that they were operating at maximum capacity, while realizing that many hospitalized patients had unmet palliative care needs. And while it is widely understood that much palliative care—particularly discussions about goals of care and management of uncomplicated pain and other symptoms—can be delivered by frontline, nonspecialist providers,36,37 in most cases, those providers have not received the education needed to provide care effectively, even for patients with uncomplicated needs. Improved models of care would include frontline providers trained in palliative care skills (most importantly, how to conduct an effective and patient-centered goals of care discussion), reliable methods of early identification of patients appropriate for a discussion about goals of care, and an efficient method for distinguishing patients with complex needs for whom palliative care specialty care is needed.
Our estimate of prevalence is nearly identical to that of Hua et al., 15 who used a comprehensive model of multiple trigger sets and found that 19.7% of patients in 179 ICUs were appropriate for palliative care consultation. Our findings also paralleled those reported to the National Palliative Care Registry™, indicating that U.S. palliative care teams care for between 4% and 7% of annual hospital admissions. 2 Using our study's 19% prevalence estimate, with approximately 30% of those patients receiving a referral, we found that 5.7% of inpatients in the participating hospitals had contact with a palliative care team member.
Geographic differences have been previously documented.38,39 Our finding of geographically based differences in referral levels mirrors that of the Center to Advance Palliative Care in showing high levels in the Northeast and low levels in the South, a possible reflection of regional cultural beliefs. 39
In our sample, only approximately half of the patients with a documented palliative care consult had a coded ICD-9 (V66.7) code. Coding practices are highly variable, ranging from 0% to 100% among participating hospitals. This variability limits the usefulness of administrative data for billing, quality improvement, and research purposes.
We know that our definition is not exhaustive in estimating the prevalence of patients appropriate for palliative care referral; patients with other diagnoses clearly qualify for palliative or hospice care, and a number of other sets of criteria exist. In fact, our data revealed a set of patients not meeting our study criteria but receiving a referral or services. As with the patients in our study cohort who received a referral, these patients appear to have been near the end of life; more than half died during the hospitalization or were discharged to hospice. However, patients with the three study conditions have been found to constitute 60%–80% of palliative care or hospice patients.33,40,41 Heart disease, cancer, and COPD are the top three leading causes of death in the United States.42,43
Weissman and Meier 36 created a definition of patients in need of a palliative care assessment in which the “starting point for all criteria chosen was the identification of patients with a potentially life-limiting or life-threatening condition.” Our definition is consistent with this and with those of other authors, and any limitations are outweighed by our ability to utilize our comprehensive database as a data source for the entire population.
Findings from the qualitative study also reflected findings of others. A lack of standard definitions for terminology in palliative care in oncology has been documented. 44 Education and interest in end-of-life issues has been found to be associated with practice among intensive care physicians. 45 An additional article will provide further examination of the qualitative study findings.
Limitations
Our estimated prevalence is a conservative figure and underestimates the unmet need for palliative care. Because our three definition conditions constitute only 60%–80% of palliative care or hospice patients,33,40,41 the actual prevalence of patients appropriate for palliative care referral in U.S. hospitals may be as high as 23% to 27%, indicating an even larger opportunity to improve care for these vulnerable patients.
Our findings reflect bias related to differences among hospitals in charting and coding practices. Also, despite our efforts to increase reliability, there was variation in chart reviewers' interpretations of what constitutes a palliative care service, particularly regarding services delivered as primary palliative care without input from a palliative care team member. Last, palliative care service offerings (e.g., inpatient beds, ambulatory services) differed among participating hospitals.
The number of organizations included in our qualitative study was small, which strictly limits our ability to generalize our findings. However, our analysis yielded saturation; highly consistent ideas and opinions were expressed by clinicians across each of the four participating hospitals.
Conclusion
This is the first multisite study designed to estimate the prevalence of hospitalized patients appropriate for palliative care referral in U.S. hospitals. The findings demonstrate the need to expand the availability of palliative care services, including primary palliative care delivered by frontline providers. We hope this information is useful for those who are striving to advance the timely delivery of high quality and high value palliative care services for patients with serious, life-limiting illness.
Footnotes
Acknowledgments
We would like to acknowledge the generous contributions of Stephen Thomas, Vern Herbener, Lynn Ceronsky, Corita Grudzen, Katherine Henderson, Stephen Howell, and Monique Neault to the development and completion of this project.
None of the authors of this manuscript have any current or foreseeable financial or personal relationships that might inappropriately influence their actions and create a conflict of interest with respect to this work.
Author Disclosure Statement
No competing financial interests exist.
Appendix A
APPENDIX B
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.