
Abstract
Abstract
Background:
Congenital anomalies account for 20% of neonatal and infant deaths in the United States. Perinatal palliative care is a recent addition to palliative care and is meant to meet the needs of families who choose to continue a pregnancy affected by a life-limiting diagnosis.
Objective:
To examine characteristics of programs and services provided, assess alignment with the National Consensus Project domains of care, and identify providers and disciplines involved in programs.
Design:
A cross-sectional survey design included 48 items addressing funding and domains of quality care.
Subjects:
Program representatives from 30 states (n = 75).
Principal results:
Perinatal palliative care programs are housed in academic medical centers, regional or community hospitals, local hospices, or community-based organizations. Significant differences by program setting were observed for type of fetal diagnoses seen, formal training in communicating bad news to parents, mechanisms to ensure continuity of care, and reimbursement mechanisms. One hundred percent of programs provided attention to spiritual needs and bereavement services; 70% of programs are less than 10 years old. Follow-up with parents to assess whether goals were met occurs at 43% of the perinatal palliative care programs. Formal measures of quality assessment were articulated in 38% of programs.
Conclusion:
This study dramatically adds to the literature available on perinatal palliative care program settings, types, and domains of care. It is clear that there are a variety of types of programs and that the field is still developing. More work is needed to determine which quality measures are needed to address perinatal care needs in this population.
Introduction
C
Although recommendations are emerging from research and practice regarding care for parents who choose to continue pregnancy after a life-limiting fetal diagnosis,4,5 data are lacking on what actually constitutes high-quality care during pregnancy under these circumstances. The American College of Obstetricians and Gynecologists Committee on Ethics and the American Academy of Pediatrics Committee on Bioethics 6 underscore the need for a thorough informed consent process involving exhaustive discussion of possible risks and benefits of various perinatal care options when the fetus is impaired. Well-informed communication between parents and care providers facilitates parental autonomy and freedom of choice in perinatal palliative care. Denney-Koelsch and colleagues 7 emphasized the role of ultrasound and obstetrical care providers in improving communication with parents by sharing valuable knowledge and facilitating parents' understanding. Other recommendations include respecting the baby as a person8,9; providing supportive, empathic counseling for parents,10, 11 and providing consistent care by perinatal palliative care team members. 9
Several experts have published their insights into perinatal palliative care program development with services that begin antenatally and continue after birth with follow-up bereavement support.12–15 These publications describe the roles of stakeholders, give practical guidance and tools, and introduce the concept of a care coordinator.13–15 Leaders from successful programs can guide the development of new programs, which may be based on existing bereavement care services. 15
Current literature and the work of the experts on the National Consensus Project (NCP) for Quality Palliative Care 16 guided this study. In the NCP structure, palliative care resides in eight domains, each with specific guidelines that serve as the basis for comprehensive and high quality care. Domain 1 contains nine guidelines that focus on holistic care delivered by an interdisciplinary team trained in palliative care and supported in their work. Interdisciplinary teams in which different types of staff work together to share expertise, knowledge, and skills are expected to improve patient care. 17 Care is to be delivered in a safe environment with respect for the patient and family values and wishes. Health care providers are supported in collaborating with patients in the development of care plans based on families' needs, preferences, values, and goals. Domain 2 addresses assessment of pain and symptom management and the development of treatment plans for physical symptoms. Domain 3 addresses the psychosocial and psychologic implications of end-of-life issues as well as the need for grief and bereavement services.
In Domain 4 the family's social fabric is assessed; this domain, similar to all domains, promotes coping and advance care planning, individualized goals of care, and cultural preferences. Domain 5 directs the interdisciplinary team to assess and address spiritual dimensions of care, and to facilitate any special rituals desired by the patient and family. Domain 6 addresses the provision of care in a culturally and linguistically appropriate manner, and to maximize accessibility and responsiveness to a multicultural population. Domain 7 specifies care for patients at the end of life. Domain 8, entitled Legal and Ethical Aspects of Care, mandates that goals be developed in accordance with state and federal law and current standards of care. This domain includes policy development and practice based on professional codes of ethics, scopes of practice, and standards of care for all relevant disciplines. The interdisciplinary team is expected to identify, acknowledge and address ethical issues.
Because perinatal palliative care is a relatively new model of care with little evidence as yet to inform practices and interventions, we conducted an extensive survey of perinatal palliative care programs in the United States to address these questions: (1) Are characteristics of perinatal palliative care programs aligned with the NCP domains of care?; (2) Which providers and disciplines are involved in perinatal palliative care?; and (3) What services do perinatal palliative care programs provide?
Methods
Survey creation
After a thorough review of existing evidence regarding perinatal palliative care and examination of the NCP guidelines, we—five perinatal and palliative care experts from nursing and medicine—developed a survey with the goal of describing services provided by perinatal palliative care programs, reaching consensus on survey items after several iterations. We piloted the survey with a cohort of physicians and perinatal palliative care program administrators to gauge clarity, relevancy, and completion time. The survey was modified based on pilot data. The final survey included 48 items addressing the 8 domains of quality palliative care recommended by the NCP along with items addressing program funding. The Institutional Review Board at the University of North Carolina, Greensboro determined that this survey involved program evaluation and was not human subjects research.
Sampling
Using the website www.perinatalhospice.org as our initial platform, we identified existing perinatal palliative care programs in the United States that provide care for pregnant women who have a life-limiting fetal diagnosis and their families. Subsequently, we performed Internet searches by state using keywords “perinatal palliative care” and “perinatal hospice.” We searched two pediatric palliative care listservs for perinatal palliative care programs. We contacted 136 program administrators from 42 states by phone to inform them of the survey, identify an individual to complete the survey, and verify e-mail addresses. The survey was deployed via a link embedded in an e-mail describing the survey. Qualtrics, an online Web-based platform, was used to collect data. Program administrators were sent three e-mail reminders during the 5 weeks during which the survey was open. Participants were encouraged to provide both quantitative data and narrative feedback. The return rate was 55% (75 responses).
Statistical analysis
Frequencies and percentages were used to summarize data from all respondents. Characteristics of programs by setting were examined using Chi-square or Fisher's exact tests. All analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC). A two-sided p value <0.05 was considered statistically significant.
Results
Results by program setting
Parents learn of perinatal palliative care programs from many sources, and services are provided in a variety of locations (Table 1). Figure 1 reflects participation by state. Settings included academic medical centers, regional or community hospitals, local hospice or palliative care organization, or community-based support systems. Table 2 shows differences in survey participation by program setting. Significant differences by program setting were observed for several variables, as follows: type of fetal diagnoses seen; training for personnel in the communication of bad news; mechanisms to ensure continuity of care; reimbursement mechanisms; availability of an ethics board; and website presence. All settings reported at least 94% of the diagnoses seen were “clearly fatal” except for community-based support systems (83%; p = 0.04). All perinatal palliative care program settings saw patients with fetal diagnosis with “expected short life span” (100%) except for community-based support systems (83%; p = 0.03).
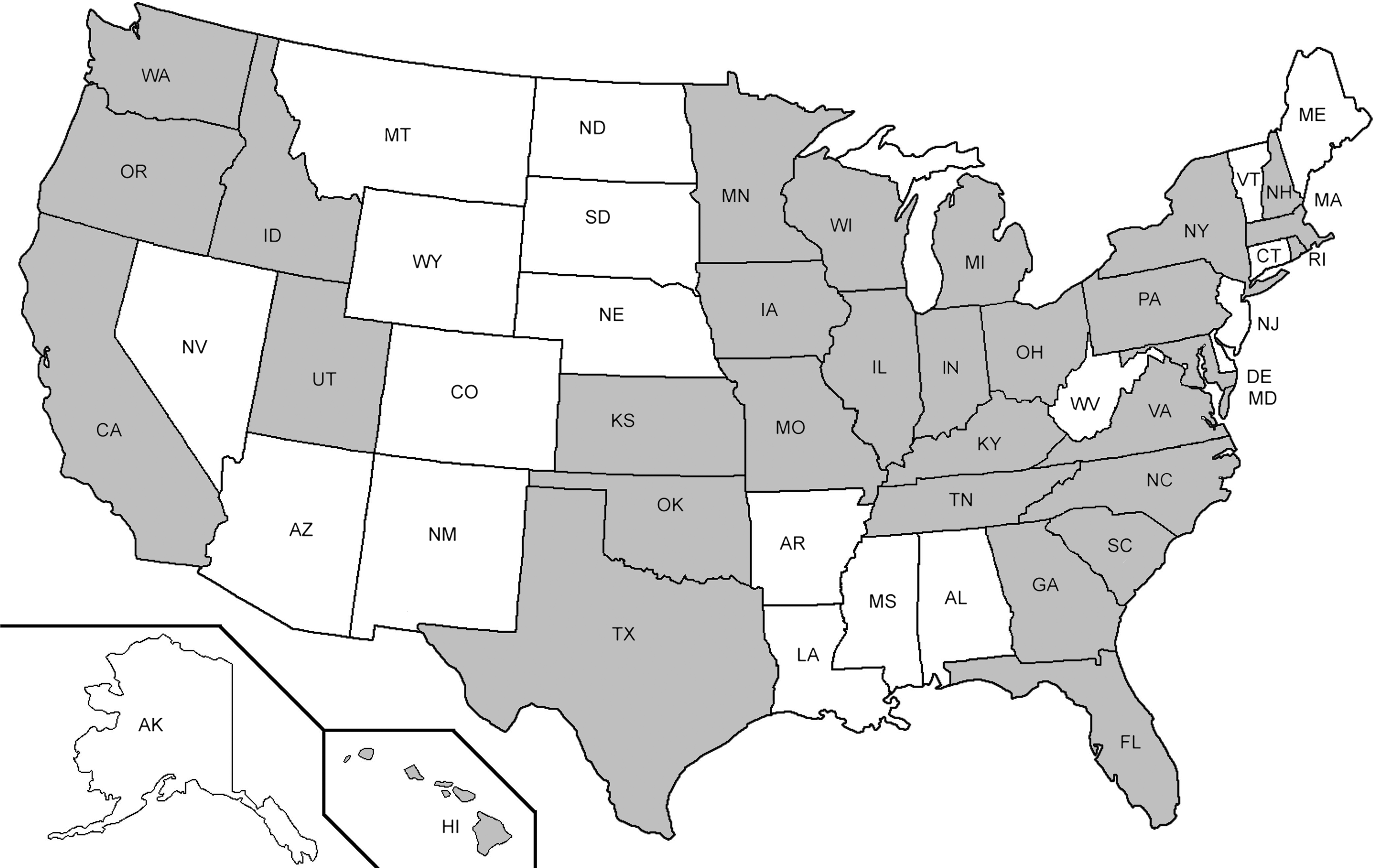
Participating states.
Respondents encouraged to check all that apply.
Numbers are n (%). Frequencies do not always sum to column n due to missing responses.
National Consensus Project domains indicated where applicable.
IDT, interdisciplinary team; EOL, end-of-life.
Community-based support systems were more likely than other program settings to have no formal end-of-life training in communicating bad news in a compassionate way (p = 0.01). Mechanisms to ensure continuity of care were also significantly different by setting (p = 0.02).
Perinatal palliative care program settings differed significantly in their reimbursement mechanisms: billing insurance for consultation (academic medical center 56%, regional or community hospital 12%, local hospice or palliative care organization 19%, and community-based support systems 0%; (p < 0.01) and grant or philanthropic funding (academic medical center 44%, regional or community hospital 24%, local hospice or palliative care organization 75%, and community-based support systems 67%; p = 0.02).
Domain 1: Structure and processes of care
Perinatal palliative care programs were characterized by care rendered by an interdisciplinary team. The most prevalent types of disciplines were spiritual care (89%), medicine (87%), nursing (84%), social workers (83%), and hospice providers (79%). Other perinatal palliative care team members included genetic counselors, volunteers, child life specialists, case managers, ethicists, midwives, and developmental experts. The majority (83%) of programs reported having a coordinator of care who were nurses (48%), social workers (22%), or was a role shared by more than one person (10%). Genetic counselors, physicians, and a child life manager were also listed as coordinators. Coordinators worked an average of 18 hours per week (standard deviation [SD] = 15.6), but data did not capture compensation mechanisms for coordinators' time. Eighty-two percent of the programs had a designated person available around the clock for parents to contact for urgent issues.
Families receiving services from perinatal palliative care programs are assisted with developing goals of care. Programs report facilitating goals of care when fetal prognosis is unclear (95%); for pregnancy-related goals (82%); labor and birth (97%); and postnatally, for a stillborn infant (95%) or a live-born infant (99%).
The majority (88%) of programs reported that documentation processes are in place with the use of electronic medical records, consultations, and access to the mother's chart. Programs had wide variation in their methods to promote continuity of care, such as regular meetings, e-mail updates, dissemination of information via a specific individual on the interdisciplinary team, and standard charting. The interdisciplinary team met regularly in 83% of the programs. Meetings are held in-person, via phone conferences, and sometimes information is exchanged via e-mail. Timing of meetings varied from weekly to monthly or as required based on parental needs. Meetings between the interdisciplinary team and parents are also offered in 86% of the programs.
Forty-one percent of the programs reported that all perinatal palliative care providers had formal training; 54% had some training, and 5% had none. Methods of training included board certification, advanced practice nursing, and formal programs such as End-of-life Nursing Education Consortium (ELNEC).
NCP Domain 1 includes the guideline 16 for ongoing quality assessment and performance improvement reviews; 43% of the perinatal palliative care programs have procedures (e.g., surveys, phone calls, individual meetings) to assess whether parents' goals were met. Formal quality assessment measures (e.g., Press Ganey surveys, internal surveys, meetings) were used by 38% of programs. One organization with advanced certification in palliative care collected quality measures based on Joint Commission requirements.
Domain 2: Physical aspects of care
All except one program provided assistance to parents to develop goals of care if their infant was live-born. Based on families' needs, programs provided a variety of support services, such as referrals to home hospice care, addressing nutritional requirements, laboratory testing, comfort measures for the infant including use of medications, and neonatal intensive care.
Domain 3: Psychological and psychiatric aspects of care
Grief and bereavement services are considered foundational to palliative care. Programs provided numerous bereavement interventions to support grieving parents and family members (Fig. 2).

Bereavement services.
Domain 4: Social aspects of care
Many perinatal palliative care programs provided information to parents about support groups led by other parents and online or community-based support networks as a part of bereavement services (Fig. 2). One program reported assisting parents with setting up an Internet site that allowed them to share health updates and garner support from their family and friends. Eighty percent of providers also provided support for the siblings of the expected infant.
Domain 5: Spiritual, religious, and existential aspects of care
All programs reported addressing spiritual or religious needs, typically hospital chaplains or pastoral care providers, some specifically trained in issues surrounding perinatal loss. Based on staff assessments, family spiritual needs were addressed by appropriate religious literature, facilitation of rituals (blessings, prayers, dedications, baptisms) and coordination of referrals to spiritual care providers in the parents' communities.
Domain 6: Cultural aspects of care
With one exception, all programs conducted assessments to ascertain cultural needs and wishes of the parents. These needs are met in a variety of ways across the United States, including the provision of culturally appropriate written materials and documentation of parental preferences into the plan of care. Some programs cite the importance of cultural brokers, that is, experts within ethnic and/or cultural communities who mediated communication between families and providers. One program reported specifically about how the staff helps families find alternatives for cultural traditions that cannot be honored in the clinical setting, such as the burning of incense. Documents were translated by 69% of the programs. The use of interpreter services was reported by 99%, through telephone language lines, in-person translators, iPad translators, peer volunteers, interpreter agencies, local university personnel, or faith-based organizations.
Domain 7: Care of the imminently dying patient
Guidance was provided to parents in most programs (92%) on what to expect during the dying process. Participants reported facilitating presence of extended family, honoring cultural and spiritual preferences, and treating the infant with respect and dignity. Parents were provided with opportunities to parent (bathing, holding, comforting baby) and participate in memory-making activities.
Domain 8: Ethical and legal aspects of care
Policies and protocols were available in more than half (55%) of perinatal palliative care programs and were based on recommendations from national organizations, position papers, textbooks, organizational algorithms and process maps, and internal program-specific guidelines. In 95%, an ethics board or consultation service was available for providers faced with difficult end-of-life decisions.
Discussion
Until now, little has been published that features existing perinatal palliative care programs and the services they offer. This study is a significant contribution to the literature on perinatal palliative care program settings, types and domains of care. From our findings, it is clear that there are a variety of perinatal palliative care programs with different characteristics and that the field is still developing; more than 70% of programs are less than 10 years old.
Standardization of practice is required for successful outcomes of care. 15 The Institute of Medicine (IOM) 18 provides recommendations including person-centered, family-oriented end-of-life care; comprehensive care; clinician–patient communication and advance care planning. The IOM provides definitions to assist professionals in achieving optimal outcomes, 18 however, more work is needed to apply these recommendations to the perinatal community. Although more research is needed, our findings are an important first step in highlighting key areas of strengths that align with NCP and IOM recommendations.16,18 Clinicians reported giving parents guidance and facilitating delivery of family-centered goals. Comprehensive assessment and conveyance of spiritual and cultural care based on families' values and goals are evident in our findings. Grief and bereavement support is delivered in a variety of ways from the time of diagnosis of a fetal defect, throughout pregnancy, and after the infant's birth. Assistance with goals of care and advance care planning is reported in almost every program.
The majority of the programs do not have formal training for all care providers. This is a key finding, one that underscores the lack of adequate preparation to provide palliative and end-of-life care by providers in perinatal settings. Not limited to perinatal settings, the IOM recommends including more palliative care content in clinical education, licensure, and certification examinations. 18
Compared to hospice care, which is billable through Medicare Part A, non-hospice palliative care can be incorporated simultaneously with curative and disease-focused treatments across the care continuum.18,19 Routine maternity care for women during pregnancy and birth is reimbursable, as is medical care for unhealthy infants. However, our findings suggest a gap in the reimbursement available for perinatal palliative care providers. Many programs receive support from donors or grants, which may be difficult to sustain over time. Although the costs of delivering palliative care during the pregnancy, birth, and postnatal period are yet to be determined, financial reimbursements must eventually align with the care provided under these difficult circumstances.
Fewer than half of the perinatal palliative care programs assess quality-driven outcomes. Although regulatory bodies and national palliative care organizations reached consensus on the importance of quality-driven health care and value-based care,16,20–22 standardized measurement tools are limited for perinatal palliative care.23,24 This situation of a life-limiting fetal diagnosis poses an interesting challenge to clarify and describe the needs of otherwise healthy pregnant women who face the almost certain death of their expected infant, and the long-term impact this loss may have on her family. More research is needed to identify what essential components should be measured to determine what constitutes quality patient-centered care under these distressing circumstances. 25
Limitations
Data were collected by self-report, and although a strong method to garner information directly from the source, responses depend upon perceptions of the participants. 26 The response rate was somewhat lower than we had anticipated and could be explained by the length of the questionnaire. Although we did not get responses from programs in all 50 states, we did get data from programs in the most densely populated areas of the United States, specifically the East and West Coasts. We recognize that programs may differ regionally; hence we caution that the generalizability of our findings may be limited. Although we used several access points to identify as many palliative care programs as possible in our study, a comprehensive clearinghouse of information about perinatal palliative care programs with contact information currently does not exist.
Conclusion
Results from this study give insight into the work of 75 perinatal palliative care programs in the United States. By describing the variety of settings and forms of care that currently constitute perinatal palliative care, we have taken the first step in our goal of establishing consistent interdisciplinary evidence-based practice. There is no doubt that the existing perinatal palliative care programs are addressing the significant challenges of care for pregnant women with life-limiting fetal diagnoses and their families; with additional research to undergird clinical guidelines, more families can benefit from consistent, appropriate family-centered care.
Footnotes
Acknowledgments
The authors would like to thank Tom McCoy for his assistance with statistical analyses. Partial support for this study was provided by the Elizabeth Schotanus Professor of Pediatric Nursing fund.
Author Disclosure Statement
No competing financial interests exists.