
Abstract
Abstract
Background:
Cancer-related neuropathic pain is resistant to treatment with multiple medications and results in reduced patient quality of life.
Objective:
The aim was to find a new curative to treat neuropathic pain without using adjuvant analgesics.
Design:
This was a retrospective study that used the FACES Pain Scale (FPS) to measure pain intensity and pain relief.
Setting/Subjects:
Twenty-eight inpatients who were treated with other strong opioids and who consulted the palliative care team about their pain relief.
Results:
In 22 (78.6%) out of 28 patients who successfully switched to methadone from other strong opioids, such as oxycodone and fentanyl, within two weeks, the mean FPS score was significantly reduced from 4.43 to 1.86, and methadone switching either reduced the number of prescriptions or stopped them entirely in 12 out of 17 (70.5%) patients who had used adjuvant analgesics before switching to methadone.
Conclusions:
These results suggest that opioid switching to oral methadone not only achieves pain relief but also curtails substantial adjuvant analgesic use.
Introduction
I
The International Association for the Study of Pain defined neuropathic pain as “pain initiated or caused by a primary lesion or dysfunction in the nervous system.” 3 In 2008, this definition changed to “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system.” 4 Treatment of cancer-related neuropathic pain frequently requires multiple or higher doses of medications, such as adjuvant analgesics.5,6 Patients with cancer-related neuropathic pain often feel somnolence and dizziness after taking pregabalin, which is most commonly prescribed to treat neuropathic pain in Japanese palliative care wards. 7 Since this adverse effect of pregabalin is possibly related to high-dose usage, treatment with adjuvant analgesics does not achieve sufficient analgesia for neuropathic pain. Therefore, we must find new curatives to treat neuropathic pain without using adjuvant analgesics.
Methadone plays an important role in the management of severe cancer pain. 2 In Japan, since 2013, methadone has been distributed. 8 Previous reports indicated that when compared with morphine and other opioids, methadone has a number of advantages, including being inexpensive, high oral bioavailability, long half-life, lack of active metabolites, and perceived benefit in difficult pain control scenarios. 9 Methadone possesses opioid analgesic properties with adjuvant analgesics and might ameliorate the neuropathic pain that is resistant to opioid analgesics clinically. Thus, we conducted a retrospective study to investigate the effect of the methadone switch on pain relief and adjuvant analgesic use.
Patients and Methods
Trial design, randomization, and masking
This retrospective study was undertaken with 30 consecutive advanced cancer inpatients with severe cancer-related neuropathic pain who consulted the palliative care team for more effective pain analgesia. The randomization was not stratified, but allocation was concealed. Clinicians who were allowed to use methadone for severe cancer-related pain were observed. The ethics committee of Nagoya City University (No. 1178) approved the study, which was undertaken from October 2013 to May 2015.
Patients and setting
Participants were cancer patients aged older than 18 years who were treated with fentanyl or oxycodone, untreatable using other methods, and did not have severe opioid-related side effects. All consulted inpatients, who were recruited from Nagoya City University Hospital by the primary oncologist, had ineffective analgesia and had received previous opioid and other nonopioid analgesic medication for an average of 321 days (2–1857 days). The original protocols of opioid switching from transdermal fentanyl or oral oxycodone to oral methadone were demonstrated (Fig. 1).

CONSORT flowchart.
Switching procedure
Some patients using the recommended Stop-and-Go protocol received great pain and suffering during switching immediately after the official methadone release. Therefore, we designed an original protocol that modified the three-day switch described by Moksnes et al. 10 This original protocol was based on previously reported methods, including the conversion ratio, switching period, and so forth.10,11 They used a numerical rating scale for the pain scale, but our hospital introduced the FACES Pain Scale (FPS) to assess older adult patients' and children's pain intensity and suffering12,13; so, all patients were assessed using this. 14 The preswitching conversion ratio of methadone was fixed at 5:1 (oral equivalent morphine dose:oral methadone), 10:1 (low-dose fentanyl:oral methadone), and 20:1 (high-dose fentanyl:oral methadone), taking into consideration the effect of fentanyl pharmacokinetics, toxicity to avoid adverse effects during titration, 11 Japanese (Asian) ethnicity, and genetics on methadone pharmacokinetics. 15
The previous opioid dose was substituted with an equivalent analgesic dose of methadone and then discontinued (Figs. 2–4). Racemic methadone was administered every 8 or 12 hours as a tablet. The rescue dose—which previously used opioids before switching—was one-sixth or more of the baseline opioid dose. In Japan, the Ministry of Welfare forbids the use of methadone as a rescue dosage and no titration was recommended until seven days after the switch because of its long half-life. Adjuvant nonopioid analgesics and anti-cancer treatment were maintained.
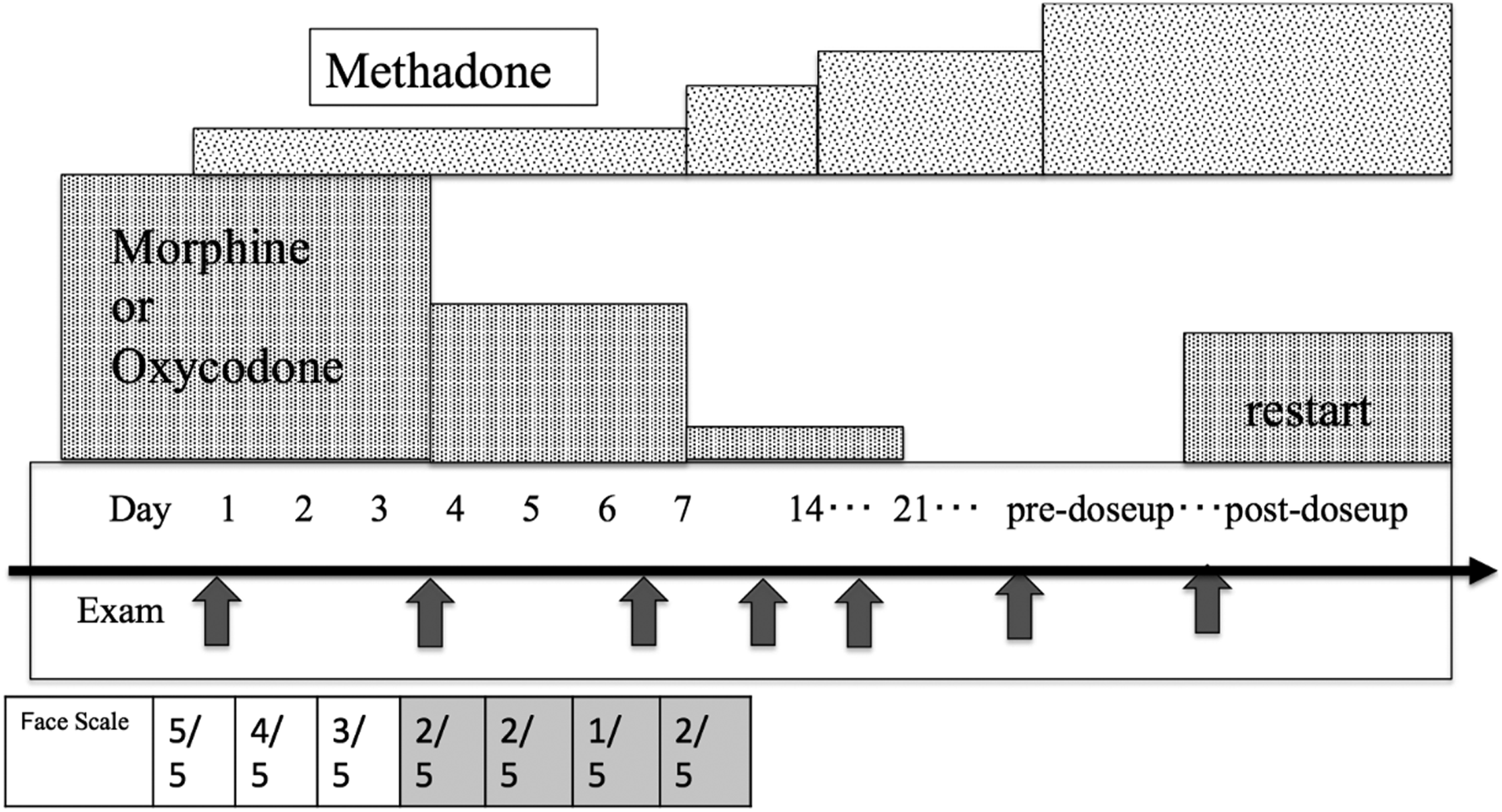
The protocol for switching from oral morphine or oxycodone to oral methadone, which is similar to the partial (gradual) approach. The conversion ratio of daily oral doses of morphine (oxycodone) to methadone was 5:1. 10 The equivalent analgesic dose was individualized by comprehensive evaluation of the FACES Pain Scale and the severity of adverse events (blood chemistry and electrocardiogram data).
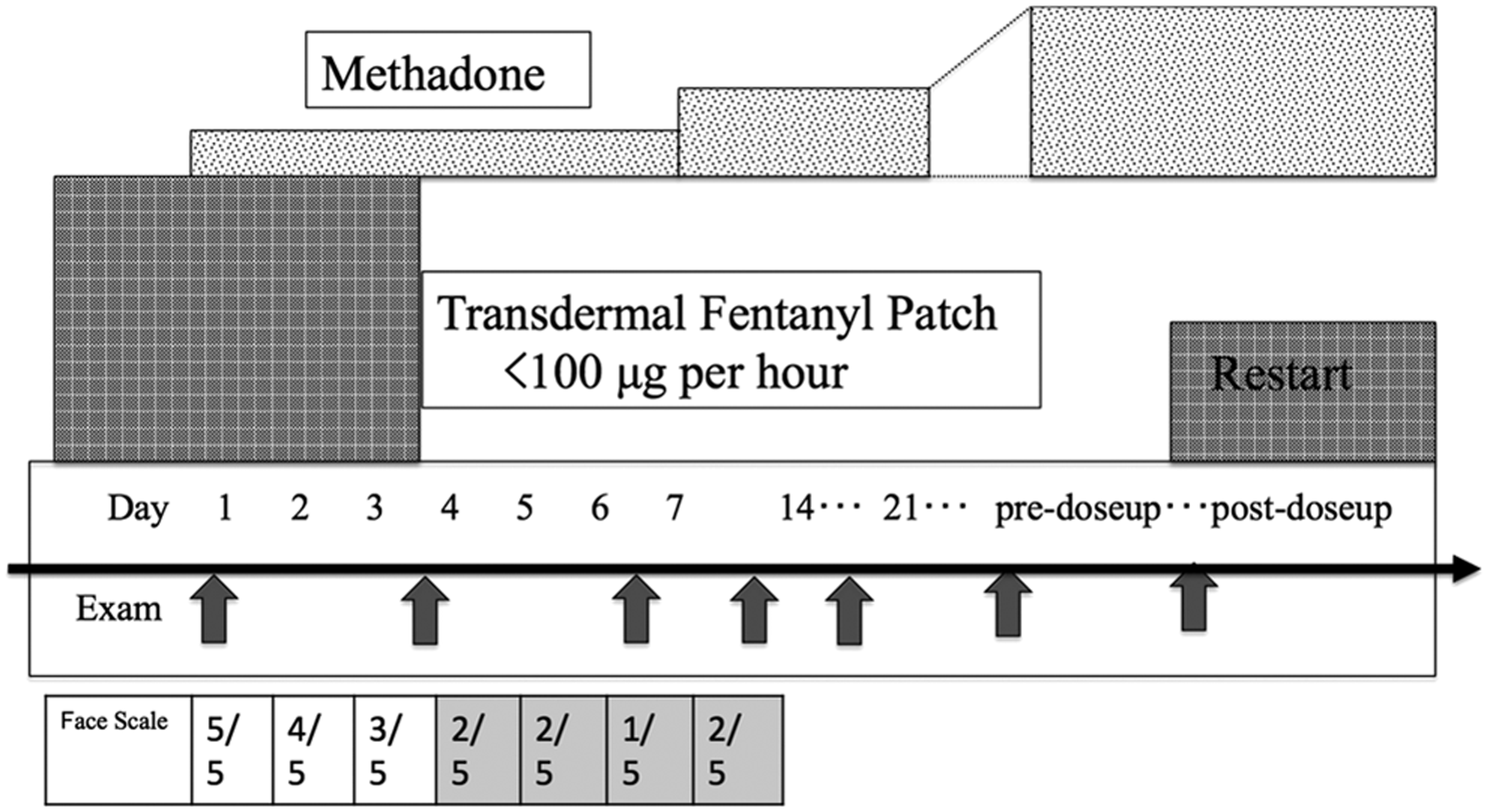
The protocol for switching from low-dose transdermal fentanyl to oral methadone, which is similar to the partial (gradual) approach or three-day switch. 26 The initial conversion ratio of daily doses of fentanyl to methadone was 10:1. 10 The equivalent analgesic dose was individualized by comprehensive evaluation of the FACES Pain Scale and the severity of adverse events (blood chemistry and electrocardiogram data).

The protocol for switching from high-dose transdermal fentanyl to oral methadone, which is similar to the partial (gradual) approach or three-day switch. 26 The conversion ratio of daily doses of fentanyl to methadone was 20:1. 10 The equivalent analgesic dose was individualized by comprehensive evaluation of the FACES Pain Scale and the severity of adverse events (blood chemistry and electrocardiogram data).
Data collection
Throughout the switching, each patient underwent clinical assessment by one or more of the palliative care team's experienced full-time physicians, nurses, and a pharmacist. The following data were collected for each patient on days 0 and 14: age, gender, preswitching Eastern Cooperative Oncology Group (ECOG) Performance Status (PS), 16 Palliative Performance Status, 17 Palliative Prognostic Index (PPI), 18 primary tumor type, type and intensity of pain,19,20 primary opioids and their dose, primary oral methadone dose, number of rescue doses, adjuvant analgesic prescriptions, and the outcome of opioid switching and its adverse events (delirium, somnolence, dyspnea, etc.). Pain intensity was assessed on a daily basis using the FPS, which comprises six grades (0: no pain, 1: hurts little bit, 2: hurts little more, 3: hurts even more, 4: hurts a whole lot, 5: hurts worst) based on patients' subjective estimations.12,21–23 We evaluated patients' pain relief via the FPS and considered further interventions if patients reported greater than grade 3 pain and no aggravation of grade. Since the FPS was reportedly correlated with the numeric scale, 24 the pain intensity was evaluated by the FPS for all patients. Electrocardiogram was checked at the preswitching and postswitching phases—once or twice per week during titration—to supervise QT prolongation. If patients had QT prolongation, mechanical recorded, or a QTc interval above 500 milliseconds in the preswitching phase, those patients were excluded before switching. If these occurred after methadone initiation, either switching stopped or there was a decreased methadone dose. 11
The outcome of opioid switching was determined on day 14 as per the clinical evaluation of the pain relief: If it was effective, patients reported no pain at rest or improvement of FPS to 1 or 0; partially effective, patients reported a little pain at rest or improvement of FPS to 2; no change meant no significant deterioration of pain; or ineffective, which meant a deterioration of pain. We assessed successful opioid switching as effective, and partially effective, no change, and unsuccessful as ineffective. 11 Any potential adverse events were noted and classified using the Common Terminology Criteria for Adverse Events v4.03/MedDRA/J v16.0. 25
Data analysis
All data were reported as means with 95% confidence intervals (CIs), ranges, medians, or frequencies (%), as appropriate. We used Welch's t-test to compare the means of the two populations, and Wilcoxon signed-rank test for the dependent variables: pain intensity (FPS), number of daily rescue doses, and number of adjuvant analgesics at preswitching versus postswitching. A p-value less than 0.05 was regarded as statistically significant, and all reported p-values were two tailed. Statistical procedures were conducted using SPSS version 22.0J for Macintosh (SPSS, Inc.).
Results
Patients
Thirty patients underwent methadone switching in the Palliative Care Consultation in Nagoya City University Hospital (Table 1). Two patients were excluded from this study because of other switching methods: the immediate approach, and Stop and Go. Twenty-eight patients underwent switching—partial approach: three-day switch. 26 A total of 22 patients (78.6%) could successfully switch from previous opioids to methadone in two weeks, and two patients (7.1%) could experience pain relief but died of cancer two weeks later; therefore, 24 patients (85.7%) could get pain relief because of switching to methadone. The mean morphine equivalent daily dose before methadone initiation was 259.0 mg/day (30–3000). The mean methadone dose at starting titration was 19.2 mg/day (7.5–40). After titration, it was 31.8 mg/day (7.5–150) (95% CI −21.9 to −2.0; paired t(23) = −2.493, p = 0.02) and the mean morphine equivalent dose with combined opioid [44.6 mg (0–600)] was 203.1 mg/day. In the 24 successfully switched cases, the mean initial methadone dose was 18.8 mg/day; afterward, it was 30.1 mg/day (95% CI −22.0 to −0.47; paired t(21) = −2.17, p = 0.042). The mean initial morphine equivalent dose, including methadone, was 156.2 mg/day; afterward, it was 169.2 mg/day (95% CI −83.6 to 57.7; paired t(21) = −0.381 p = 0.707). There were no significant differences in the mean postswitching methadone dose with/without adjuvant analgesics of 25.8 and 35.2 mg/day (95% CI −18.7 to 37.5; paired t(20) = 00.698, p = 0.187). We initially used a fixed conversion ratio: morphine (oxycodone) to methadone (5:1) and fentanyl to methadone (20:1). However, the real conversion ratio before the titration was 8.6:1 in 19 cases of successful titration for two weeks without previous opioid combination use. The final real conversion ratio after titration was 7.27:1. The mean preswitching ECOG PS was 2.71 ± 0.14, and PPI was 3.054 ± 0.54; therefore, patients anticipated only a short life expectancy.17,18
ECOG PS, Eastern Cooperative Oncology Group Performance Status.
Pain and rescue
The mean FPS scores significantly decreased after methadone switching compared with preswitching (preswitching: 4.00 ± 0.189; day 7: 2.48 ± 0.263; day 14: 2.13 ± 0.236; day 28: 1.95 ± 0.301) (day 0–7: 95% CI 1.009–2.176; paired t(26) = 5.613, p = 0.000) (day 0–14: 95% CI 1.334–2.50; paired t(23) = 6.802, p = 0.000) (day 0–28: 95% CI 1.537–2.884; paired t(18) = 6.894, p = 0.000).21–23 The mean number of rescue doses also significantly decreased from 5.62 ± 4.79 to 3.31 ± 3.12 times per day (95% CI 0.297–4.318; paired t(25) = 2.364, p = 0.026).
Severe adverse effects defined as CTCAE 25 ≥grade 3 were detected in 10 cases (Table 3). In other minor adverse effects defined as CTCAE 25 ≤grade 2, we frequently detected insomnia, but only one patient needed to decrease the methadone dosage because of an adverse effect (Table 4).
We had checked all adverse effects, caused by all situations, during titration.
Relieving severe cancer-related neuropathic pain
We evaluated the cancer-related neuropathic pain according to the Revised Edmonton Staging System19,20 and the NeuPSIG grading system. 3 Using a computed tomography scan, we checked tumor growth compressing the nervous structure innervating the relevant painful region. However, almost all patients underwent an additional objective confirmatory test. In this study, we classified types of pain into three categories: any nociceptive combination of visceral and/or bone or soft tissue pain, neuropathic pain syndrome with/without any combination of nociceptive pain, and unknown pain syndrome (Table 1). 20 Sixteen patients received concomitant adjuvant analgesics, such as pregabalin, corticosteroids, tramadol, duloxetine, and neurotropin, with previous opioids. After methadone switching, 12 patients successfully terminated the concomitant adjuvant analgesics treatment (p < 0.01, Z = −3.219) (Table 2 and Figs. 5 and 6).
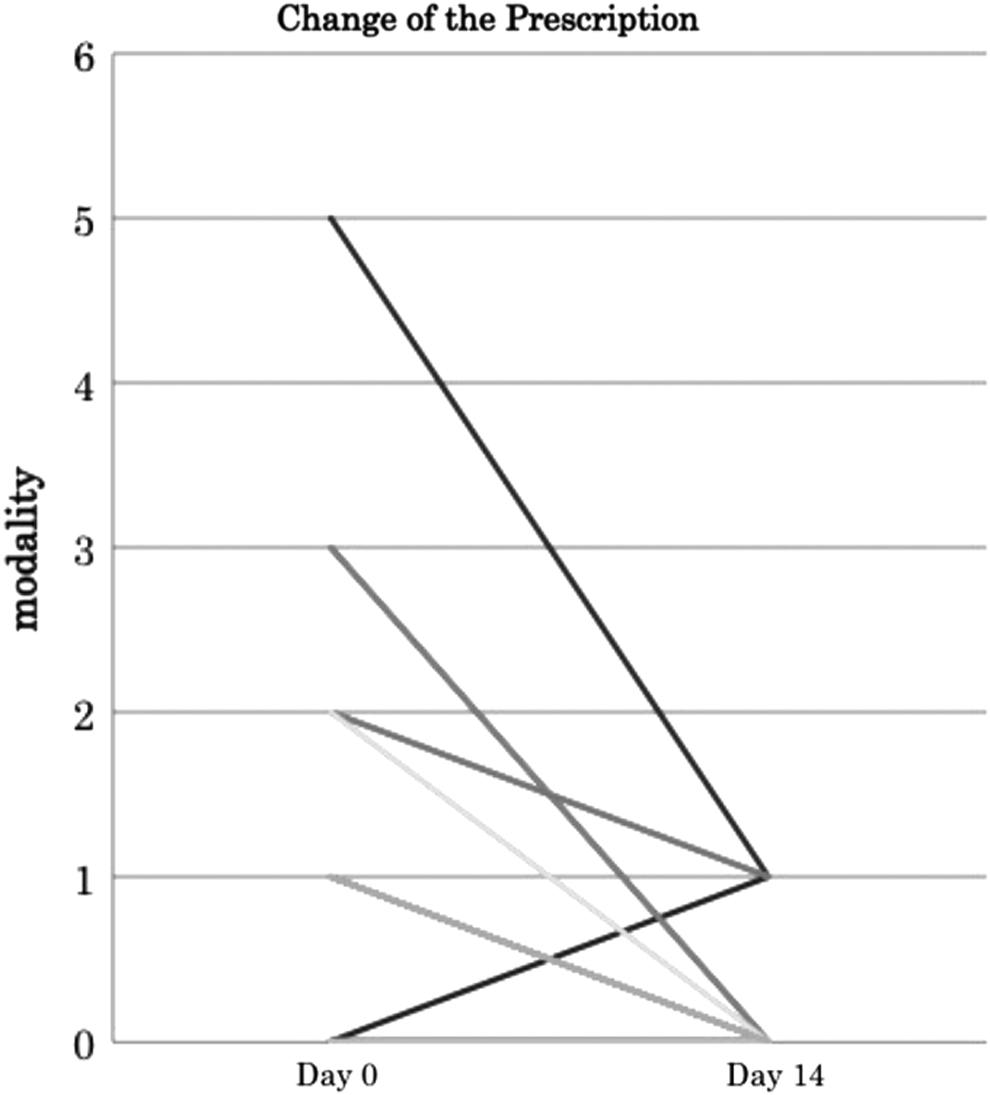
The change in the number of prescription of the adjuvant drugs both before and after the use of methadone. Multiple prescriptions of adjuvant drugs (one kind of prescription is eight patients; two kinds is six; three kinds is one; and five kinds is one) were used before starting the methadone titration. However, a single prescription of adjuvant drugs—pregabalin, neurotropin, or corticosteroids—was used alone after titration. Only one patient started corticosteroids during titration because of primary tumor events.
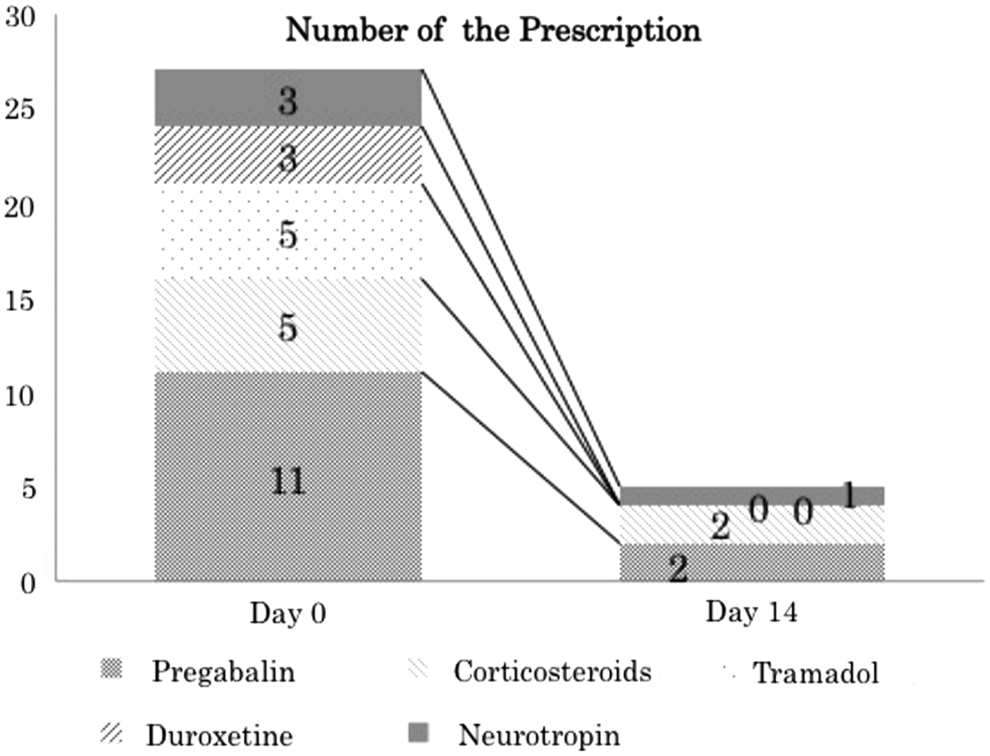
The change of the kind of adjuvant drugs used both before and after titration of methadone. Prescription of pregabalin—mainly used before titration—tramadol, and duloxetine was stopped. Prescription of corticosteroids decreased from five to two; that of neurotropin decreased from three to one. Therefore, it is possible that methadone has a reduction effect on adjuvant drugs. A total of 5.4 patients ±3.2 (mean ± SD) used adjuvant drugs at day 0, and 1.0 patients ±1.0 used them at day 14; the p-value is 0.024 (95% CI 0.932–7.868; paired t(4) = 3.523, p = 0.024). CI, confidence interval.
All cases of data of previous opioid, switching result, methadone dose at day 0, 14 (mg), the FACES Pain Scale at day 0, 14 (grade). Previous morphine dose at day 0 (mg). Equivalent morphine dose at day 14 (mg), prescription number of adjuvant drugs at day 0–14. The FACES Pain Scale was scored as follows: 0, no hurt; 1, hurts little bit; 2, hurts little more; 3, hurts even more; 4, hurts a whole lot; 5, hurts the worst.
The FACES Pain Scale was scored as follows: 0, no pain; 1, a little pain; 2, a little more pain; 3, even more pain; 4, a lot of pain; 5, the most pain.
Introduced for treatment of the tumor.
Switching was cancelled because of severe pain; the patient received intravenous opioids and sedation.
Titration was achieved, but the patient died by day 14.
Titration was finally achieved by day 28.
The patient considered pregabalin as effective and wanted to continue it. For conversion: parenteral morphine: oral morphine = 1:2, parenteral oxycodone: oral morphine = 1:2, oral oxycodone:oral mor phine = 2:3, fentanyl: morphine = 1:100.
Discussion
The present study revealed that opioid switching to methadone from other strong opioids effectively reduced the adjuvant analgesic prescriptions in cancer patients with/without neuropathic pain. Methadone switching significantly attenuated the FPS, suggesting that methadone alleviates severe pain that is difficult to treat with strong opioids with/without neuropathic pain.
Methadone produces its pharmacological action through not only μ-opioid receptor stimulation but also N-methyl-
Methadone switching decreased the concomitant use of adjuvant analgesics in 12 out of 16 patients. Adjuvant analgesics induce their analgesic activity through the different action sites. Our patients used pregabalin, 29 corticosteroids, 30 tramadol, duroxetine, 31 and neurotropin®. 32 Pregabalin produces its analgesic action through the inhibition of the α2δ subunit of voltage-dependent calcium channels. 33 Duloxetine inhibits noradrenalin and serotonin uptake to induce analgesia. 34 Almost all adjuvant analgesics would make patients sleepy, and multiple prescriptions deteriorate quality of life. In this study, somnolence was the most frequent adverse effect—detected in 11 cases—when patients having adjuvant analgesics switched to methadone. We could stop adjuvant analgesics on the way to complete titration, three to seven days after starting switching, because of pain relief improvement and the prevention of feeling extra sleepy. To the best of our knowledge, this is the first indication that the methadone switching dramatically reduced the prescription of the concomitant adjuvant analgesics in the moderate-to-severe pain of cancer patients.
In the present study, the difference between the fixed conversion ratio and the real conversion ratio before the titration was to avoid the adverse effects and to protect patients from suffering during opioid switching. Then, we adjusted the methadone dose on day 7 for patients with adverse effects and to relieve severe pain. Therefore, the increased amount of the postmethadone dosage might also account for the improved pain relief, in addition to the pharmacological properties.
At the commencement of the study, we had difficulty with opioid switching to methadone according to the Stop-and-Go protocol for patients who used a large amount of fentanyl or oxycodone. Primary oncologists often increased the dose of the opioid where the cancer-related neuropathic pain, such as malignant psoas syndrome, was regarded as a good adaptation to methadone. We considered that a large amount of opioid frequently meant difficulty in switching, especially with the Stop-and-Go protocol. With our original protocol (Figs. 2–4), patients could switch relatively safely, but they needed at least two weeks' admission for titration. Therefore, we needed to ascertain the best clinical adaptations and introduce safe switching to methadone earlier.
A serious factor limiting methadone prescription is the fatal adverse effect on cardiovascular systems. Methadone showed the QT interval prolongation in electrocardiograms. For this methadone-specific adverse effect, palliative care doctors avoid prescribing methadone in Japan. This QT interval prolongation is induced by the blockade of hERG (human ether-a-go-go-related gene) voltage-gated potassium channels in the heart. 35 Methadone-induced inhibition of hERG potassium channels results in sudden death due to severe life-threatening arrhythmias (so-called torsades de pointes). In the present study, we never observed arrhythmias after methadone switching 26 ; however, we stopped rotation for only one patient because of dyspnea and chest discomfort in a suspicious case of unstable angina after the first methadone dose. We usually checked the patients' regular drugs, preexisting QT interval (QTc) prolongation in electrocardiograms, and history of any heart diseases. In this study, only one case had preexisting QT interval (QTc) prolongation, QTc ≥450 milliseconds, and only high-dose oral oxycodone (2000 mg/day) without co-medications influencing methadone pharmacokinetics. Therefore, the methadone doses commonly used for cancer pain relief could be used safely with attention to preexisting problems, such as co-medications, history of heart disease, and preexisting QT interval (QTc) prolongation.
This was a retrospective study; therefore, bias could not be excluded. In all patients, we measured pain intensity using the FPS.12,21 This pain scale was introduced in our hospital to evaluate patients' suffering, including their pain; however, originally, the FPS was evaluated based on its assessment of pediatric patients' pain intensity. Thus, the FPS was not the best tool to use, as our study included a middle-aged group; instead, an equivalent assessment tool as per recent reports could have been used.13,14,23
This study aimed at evaluating the effectiveness of curtailing adjuvant analgesic use; however, a reduction in opioid costs could also be noted. In Japan, 10 mg of methadone (tablet) costs about 3 dollars, 40 mg of oxycodone (tablet) costs about 7.9 dollars, and 25 μg/hour of transdermal fentanyl (patch) costs about 9.4 dollars. We can achieve a cost reduction of 7.2 dollars per day per person by opioid switching to methadone only, and about 9.8 dollars per day per person in the 24 cases of successful opioid switching except for other analgesic use. However, although we could easily reduce or stop the adjuvant analgesics in the process of switching to methadone, this could not explain the dominant effect—the increase in the amount of opioid analgesics or the characteristics of methadone. A double-blind prospective study with a larger sample size is needed to validate the effectiveness of methadone use for cancer-related neuropathic pain relief.
Very few reports exist on the effectiveness of methadone switching in patients with cancer-related neuropathic pain. One report indicated that the addition of methadone was improved pain control for patients with moderate-to-severe cancer-related neuropathic pain who were on other opioids. 36 Another report indicated that methadone use was significantly associated with neuropathic cancer pain. 37 In the present study, we indicated that methadone switching successfully improved cancer-related neuropathic pain that was uncontrolled by other opioids or other methods. Moreover, adjuvant analgesic use decreased after methadone switching. Therefore, it is possible that methadone effectively improves cancer-related neuropathic pain in patients compared with other strong opioids.
Conclusion
The present study demonstrated that methadone switching effectively relieves the suffering of cancer patients and reduces the use of adjuvant analgesics in cancer patients with neuropathic pain. Methadone switching from other strong opioids improves patient quality of life, such as through the reduction of medication, pain relief, and not-so-severe adverse effects. Moreover, treatment with oral methadone may be an alternative opioid for managing mild-to-severe cancer-related neuropathic pain.
Footnotes
Acknowledgments
The authors deeply appreciate the assistance rendered by Professor Shigeki Yamaguchi (Department of Anesthesiology, Dokkyo University School of Medicine) regarding the use of methadone. This study was supported in part by a Grant-in-Aid for the KIDANI Memorial Trust Cancer Treatment Project.
Author Disclosure Statement
The corresponding author has received speaking fees from Kyowa Hakko Kirin Co., Ltd., Terumo Corporation, Taiho Pharmaceutical Co., Ltd., Teikoku Seiyaku Co., Ltd., and Shionogi & Co., Ltd.