
Abstract
Abstract
Background:
Despite growing efforts to facilitate advance care planning (ACP) to decrease health disparities in palliative care, low completion rates of advance directives (AD) have been consistently found among African Americans.
Objective:
The objective was to examine the feasibility of a multicomponent ACP intervention program that integrates motivational interviewing, evidence-based ACP facilitation program (Respecting Choices®), and health-literacy adjusted AD. This pilot study aims to address the unique barriers to ACP engagement among African Americans in the Deep South.
Methods:
The design was a mixed-method randomized controlled trial design. Analysis of covariance (ANCOVA) and thematic content analysis (TCA) were conducted to identify barriers and facilitators for ACP engagement and to assess feasibility, knowledge, and intention to complete an AD. Thirty community-dwelling African Americans (mean age M = 55.43, SD = 6.71, range = 47–73) were recruited from the Deep South and randomly assigned to receive intervention (n = 15) or educational material (n = 15) at a local university medical center.
Results:
All participants (n = 30) reported high satisfaction (M = 4.81, SD = 0.44, max score = 5) and increased intent to complete an AD at postintervention. A significant increase in knowledge on AD from baseline to postintervention was observed in the intervention group—t(14) = −3.06, p = 0.01, d = 1.67); no significant change was found for control. Lack of information, mistrust of doctors, and avoidance of discussing death were primary barriers to ACP discussions. Facilitators include ACP education, decreased mistrust, and proactive initiation of ongoing ACP discussions.
Conclusions:
Feasibility data revealed successful implementation of a brief intervention to increase ACP engagement and willingness to complete an AD among southern African Americans.
Introduction
A
Prior research reveals that multifaceted factors contribute to the existing racial disparities in ACP.15–17 The Tuskegee study and other well-documented historical injustices such as slavery, segregation, socioeconomic inequality, and racial discrimination cultivate the longstanding issue of medical mistrust.18,19 The suspicion of not being offered optimal treatments has been found to be associated with an individual's hesitancy to complete an advance directive (AD) and preference to pursue aggressive life-sustaining treatment over comfort care.5,20 When facing uncertainty related to physical illness and death, religious/spiritual coping are commonly observed among African Americans in the Deep South.6,15 Patient autonomy, however, may be perceived as contradictory to the spiritual value of trusting God's sovereignty. 21 Additionally, low health literacy makes ACP a greater challenge, as nearly 60% of African American adults have either a below basic or basic health literacy level.7,22 Generally, an intermediate health literacy level is necessary to make informed medical decisions; therefore, the ability to understand the standard AD form is significantly compromised among this population. 23
A multicomponent intervention to address barriers
Over the past decade, several intervention programs have been developed to facilitate ACP among racial/ethnic minorities in other regions of the United States.24–28 For example, the SPIRIT (Sharing Patients' Illness Representations to Increase Trust) intervention demonstrated acceptance and enhanced ACP communications between African American dialysis patients and their surrogates 26 . Bonner et al. developed a group-based education intervention, ACT-Plan (Advance Care Treatment Plan), to enhance knowledge and skills in ACP among African American family caregivers. 24 Volandes and colleagues found that the use of video decision aids among Latino patients significantly decreased educational barriers to ACP. 27
Despite these growing efforts, there is a paucity of randomized studies evaluating the feasibility and acceptability of interventions that target African Americans from the Deep South where unique historical, cultural, spiritual, and socioeconomic characteristics may impact an individual's advance care decision making. To fill in the gap of the literature, we sought to (1) identify perceived barriers and facilitators to ACP engagement and (2) examine feasibility and acceptability of a multicomponent intervention that addresses the unique barriers of ACP engagement.
Building upon the Framework of Health Literacy and Health Action, 29 the Thinking Ahead Project (TAP) is a single-session, 90-minute intervention. As shown in Figure 1, the three components of TAP target psychological, cultural, and cognitive factors to enhance ACP engagement. The first component, motivational interviewing (MI), is an evidence-based, client-centered interviewing method aiming to enhance awareness and engagement of health behavior change.30,31 The second component, Respecting Choices®, is an evidence-based ACP facilitation program14,28 that is widely adopted in more than 30 states across the United States. The First Steps® ACP protocol 32 was chosen for its strength in motivating individuals to learn more about ACP, normalizing the concept of planning, and developing a plan to complete an AD. Two additional questions were added to the protocol to identify perceived barriers and facilitating strategies from the local community's standpoint. The third component, health literacy adapted AD, is a revised AD form designed to meet the literacy level of most U.S. adults. 23 Most sections are written at a fifth grade reading level, with concrete language and culturally diverse, text-enhancing graphics. 23
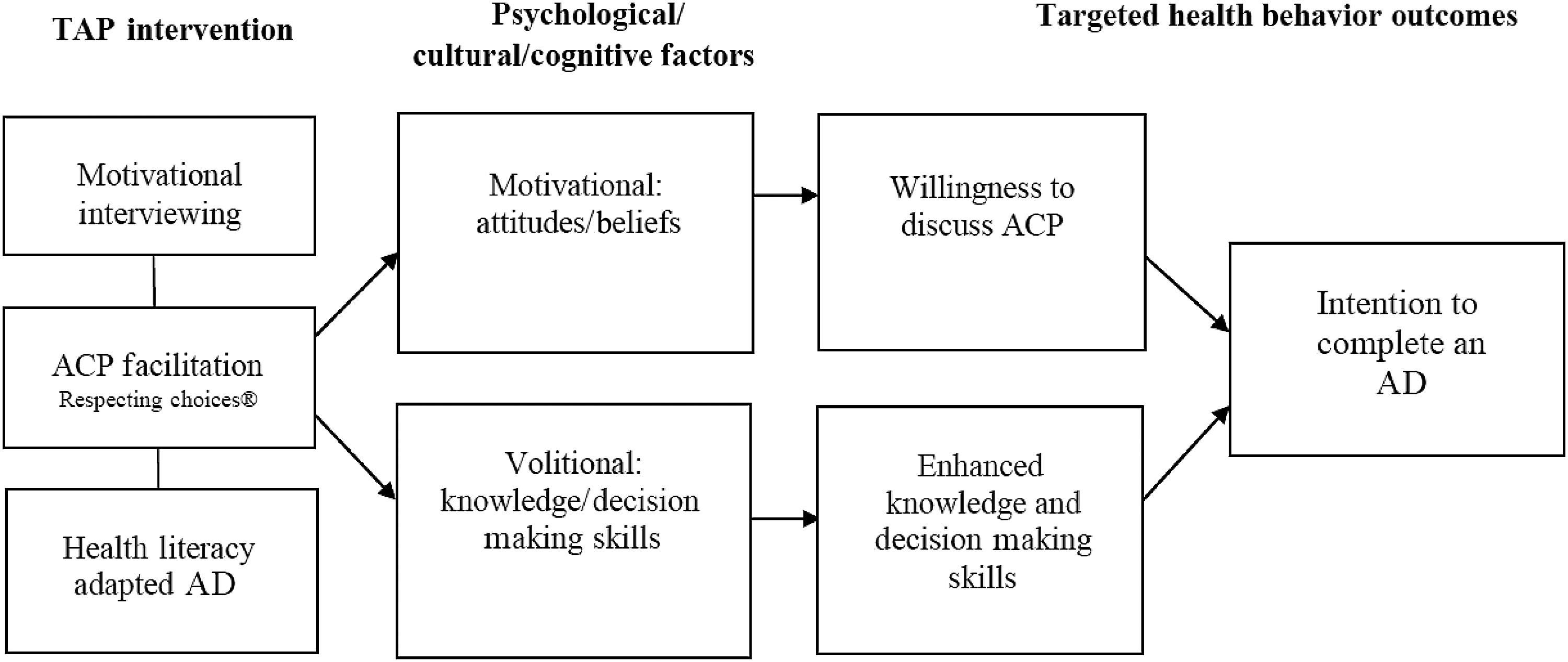
Theoretical framework of the Thinking Ahead Project. ACP, advance care planning; AD, advance directive; TAP, thinking ahead project.
Methods
Design and participants
A mixed-method randomized controlled trial (RCT) design was employed. Participant eligibility criteria include (1) African Americans aged 45 years and older, (2) English speaking, and (3) no evidence of cognitive impairment as indicated by a cut-off of ≤2 errors on a six-item cognitive screener. 33 Forty-eight community-dwelling participants from Deep South communities were recruited and screened via phone between March and May 2014. Participants were encouraged to identify acquaintances to participate; thus, both direct recruitment and snowball sampling were used. Thirty eligible participants were recruited and randomly assigned to one of two groups. One group received the TAP intervention (n = 15), and the second group (control group) received educational material (n = 15) at a local university medical center. Figure 2 presents the consort diagram of the study participants. The study was approved by the University of Alabama institution review board.
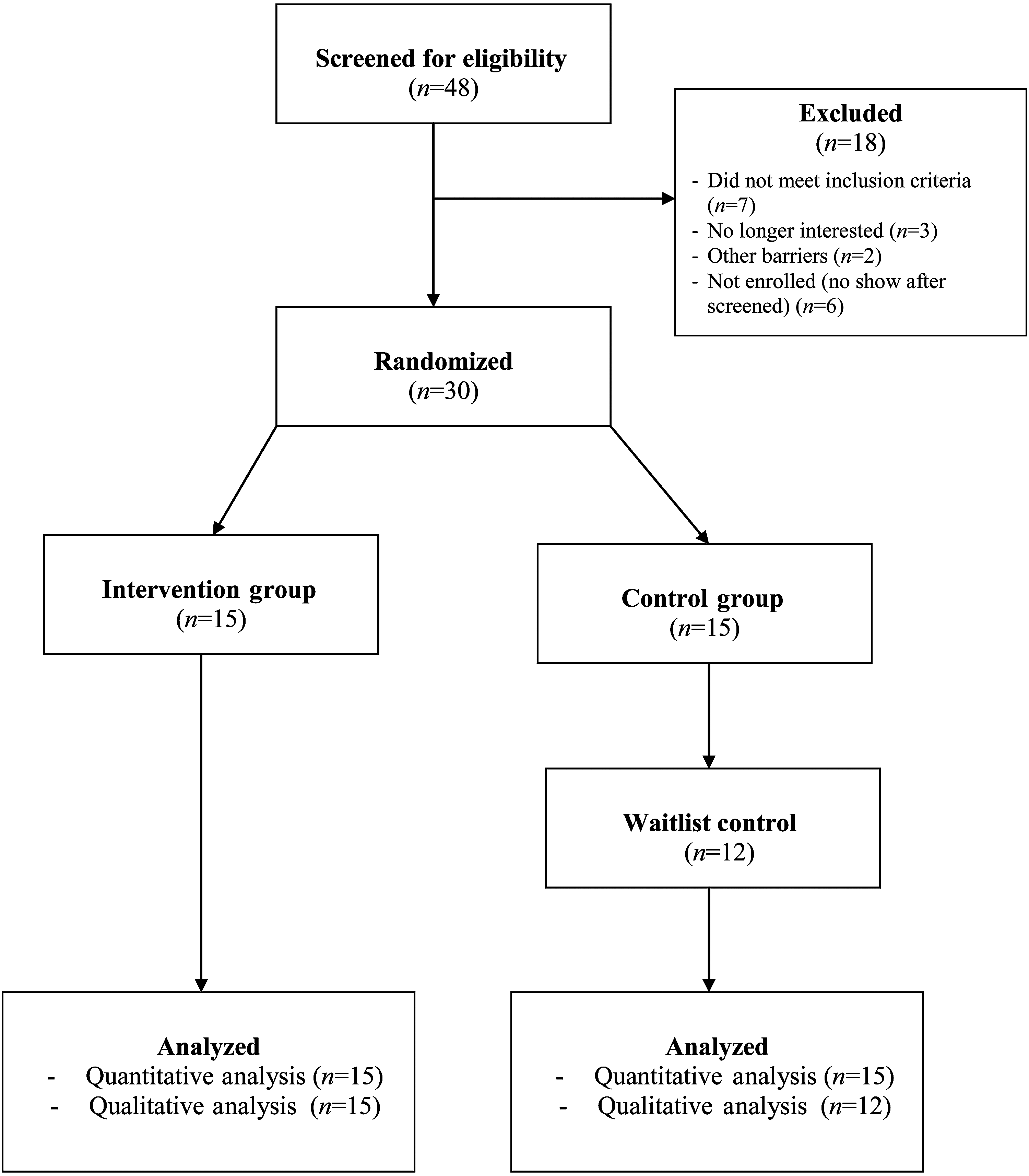
The consort diagram of study participants.
Procedure
All participants provided informed consent and completed pre- and postintervention assessment that evaluates demographic and health characteristics. Primary study outcomes are described in the measures section.
Intervention group
Participants received a 90-minute intervention comprised of a 60-minute semistructured interview adapted from the Respecting Choices First Steps® ACP protocol 32 and a 30-minute guided AD coaching. The interventionist is a certified Respecting Choice® Facilitator who completed a four-hour didactic, supervised MI training. MI techniques such as rolling with resistance, asking open-ended questions, using affirmation, and support autonomy were incorporated throughout the interview process. 30 A package of ACP educational material with both the standard and health literacy adapted AD was introduced during the guided AD coaching.
Control group
Participants were provided ACP educational materials and asked to review the material on their own for up to 30 minutes. This is to mimic real-life situations where ACP information is generally given without further guidance. The 30-minute timeframe was determined based on Sudore et al., 23 allowing sufficient time to review the AD forms. No motivational interviewing, facilitated ACP discussions, or guided coaching were provided. Upon completion of postintervention assessment participants in the control group were offered the opportunity to receive the TAP intervention. Eighty percent of the control group voluntarily participated in the TAP intervention as waitlist control (n = 12).
Measures
Background characteristics
Participants' background characteristics assessed prior to participation served as baseline measures (T1). Measures include self-reported health (SRH), 34 Charlson Comorbidity Index (CCI), 35 the Short Version of the Test of Functional Health Literacy in Adults (S-TOFHLA), 36 the Personal Health Questionnaire Depression Scale (PHQ-9), 37 and the Brief Multidimensional Measure of Religiousness and Spirituality (BMMRS). 38 The current study sample achieved a Cronbach alpha range 0.70–0.97 of baseline measures.
Primary outcomes
Feasibility was assessed with study completion rates, average length of intervention, and a five-item program satisfaction survey adapted from the Respecting Choices® Program Evaluation Questionnaire. 32 The first four items were rated on a five-point Likert scale (1 = not at all, 2 = limited, 3 = somewhat, 4 = fairly, 5 = very much/very confident). The fifth item was used to collect participants' qualitative feedback to improve the TAP intervention. Knowledge of AD was assessed with a 12-item scale developed by Sudore et al. 23 The response option for each item was either “True” (1) or “False” (0). A higher proportion of correct responses indicate a more accurate understanding of the purpose and content of an AD. Intention to complete an AD was assessed with a single-item question: “The health coaching session has helped increase my intention to complete an advance directive form.” Response option was either “Agree” (1) or “Disagree” (0). Preference for an AD form was assessed by asking, “After reviewing both forms of the advance directives, which form do you prefer to use?” Response options include (1) “the colored form (the health literacy adapted form)” and (2) “the black and white form (the standard AD form).” 23 Participants who stated a preference were asked to describe why they preferred a particular form.
Treatment fidelity
Intervention sessions were audiorecorded and transcribed verbatim. Twenty percent of the intervention sessions were randomly selected for evaluation to monitor the interventionist's adherence to the First Steps® ACP protocol and MI techniques. Content fidelity (the extent to which each of the seven components of the intervention was delivered) and process fidelity (the extent to which the MI skills were used) were evaluated and achieved high fidelity.
Data analysis
The convergent design of a mixed-method approach was employed to analyze the combined quantitative and qualitative data. 39 Quantitative analyses were conducted using SPSS 22.0 (IBM, Armonk, NY). Descriptive analyses of assessment data were used to examine the participant's background characteristics at baseline. Between-group analyses of covariance (ANCOVAs) were performed to assess the effect of intervention on knowledge of the AD. Within-group comparison of baseline and postintervention means for primary outcomes was made using paired sample t-tests. Semistructured interview data were analyzed using thematic content analysis (TCA). 40 Investigator triangulation was performed by a three-member analysis team (CSH, XA, and CA). Team members independently reviewed transcripts along with the major themes and subthemes generated through line-by-line coding. The triangulation achieved an inter-rater reliability of 0.93, providing evidence of the trustworthiness of the qualitative findings.
Results
Sociodemographic and health characteristics
Table 1 summarizes the background characteristics of the participants. The mean age of the study participants was 55.43 (SD = 6.71; range 47–73). Forty-three percent of the participants were female. Participants were mostly unmarried, unemployed, and lived with perceived inadequate income. The mean for the number of years of education of 12.3 (SD = 2.25). Ninety percent of the study sample demonstrated adequate functional health literacy, with a mean health literacy score of 29.40 (SD = 7.30). Of the study sample, 63.3% endorsed depression; 73.3% reported being moderately/very religious, while 83.3% endorsed being moderately/very spiritual. No between-group differences were found among any of the sociodemographic and health characteristics, although approximately 47% of the intervention group reported having health insurance compared with 73% of the control group. It may be that possession of health insurance exerted some influence on participants' perceived barriers and facilitators for ACP engagement.
M, mean; SD, standard deviation.
Number of errors on six-item cog was assessed using the six-item cognitive screener.
Health literacy was assessed using the Short Form test of Functional Literacy in Adults (s-TOFHLA).
Depression was measured using the Patient Health Questionnaire (PHQ-9).
Religiosity/spirituality was measured using the Brief Multidimensional Measure of Religiousness and Spirituality (BMMRS).
No between-group differences were found using t-tests or chi-square tests (p > 0.05).
Perceived barriers to advance care planning engagement
Table 2 presents six major themes of the perceived barriers. Findings revealed that one of the main reasons for low engagement in ACP among African Americans is the lack of information and patient education resources in the local community. Several participants noted:
“What kind of barriers? Mmm…I would, I would probably think uh a lack of education…uh… a lack of informed education.” [Participant #7] “Well, it's just about like everything. Its… they don't have that…the education, you know. The education gonna tell you, you know is not being placed in front of ’em.” [Participant #6] “Many times we-you don't know the right people or the right sources to go to, to help you with this this uh, planning for your future.” [Participant #20]
Suggested strategies to overcome the barriers
Table 3 displays major themes of identified strategies to enhance ACP engagement in the local community. It is noteworthy that participants expressed a strong desire to learn more about ACP and have education or information delivered to the local community to meet their health literacy needs. Participants suggested that ACP intervention providers should take a proactive approach by going to the community gathering place to meet people where they are:
“Actually communicating with the people on a face to face basis because that's what you really need to get their attention. Go to that gathering places, you know…. It would be very much help. They would be more trusting…. They may be more susceptible to accept.” [Participant #11]
Feasibility
All 30 participants completed the single-session intervention and related assessments. On average, each session lasted 85 minutes (SD = 7.23, range 64–92). As shown in Table 4, participants provided high satisfaction ratings, ranging 4.67–5 on a five-point Likert scale. More than 80% of study participants reported that the TAP intervention helped them “very much.” A greater portion of the participants in the intervention group (86.7%) endorsed that they felt “very much” prepared to make future care decisions for themselves compared to those in the waitlist control group (66.7%). Similarly, a greater portion (93.3%) of the intervention participants felt that their needs for ACP were “very much” met during the TAP intervention as compared to those in the waitlist control (83.3%). While participants reported an overall high level of confidence, all participants in the waitlist control group endorsed that they were “very confident” (100%) to complete an AD form..
ACP, advance care planning; AD, advance directive; KAD, Knowledge of Advance Directive; M, mean; SD, standard deviation.
As measured with the Program Satisfaction Survey on a five-point Likert Scale. Higher scores indicate higher level of satisfaction.
The overall percentage of 12 factual items about ADs answered.
A paired-samples t-test was conducted to evaluate the impact of intervention on KAD of the intervention group. There was a statistically significant increase in KAD from Time 1 to Time 2.
Group differences were compared using t-tests or ANCOVA.
p < 0.10.
p < 0.05.
Knowledge
A mixed-effect ANCOVA was conducted to assess the effect of intervention on Knowledge of Advance Directive (KAD) while controlling for baseline KAD scores. Findings revealed a trend for time by group interaction: Wilk's Lambda = 0.90, F(1, 28) = 2.98, p = 0.09, d = 0.59. This indicates that the change in KAD over time differs between the groups, as participants in the intervention group reported a marginal higher increase on KAD from baseline (T1) to postintervention (T2) as compared to those in the control group.
Paired-samples t-tests were conducted to evaluate the impact of the intervention on knowledge within the two groups. There was a statistically significant increase in KAD for the intervention group from T1 (M = 73.89, SD = 16.33) to T2 (M = 83.89, SD = 16.20), t(14) = −3.055, p = 0.01, d = 1.67, indicating a large effect. No significant increase in KAD change score was found for the control group. Other participants noted that the TAP intervention was “very well covered” [Participant #29] and helped to make ACP simpler to understand:
“You know what, this (ACP) is gettin’ more and more simpler then. You know, it used to be so complicated, to me, it was complicated.” [Participant #5]
Preference
Study participants with two different functional health literacy levels as measured by the S-TOFHLA (adequate versus limited) both reported a preference for a health literacy adaptive AD form over the standard AD form (56% versus 28% for adequate literacy, 100% versus 0% for limited adequacy). When asked why they prefer this form, one participant with limited literacy reported, “Because it has more pictures to help me understand more” [Participant #22].
Intention to complete an advance directive
When asked if the TAP session has increased her or his intention to complete an AD, participants agreed unanimously (100%) in both the intervention and the control group.
Revised framework of the intervention
Based on study findings and participants' feedback, a revised conceptual framework was developed to take contextual/health care system factors into account to facilitate ACP (see Fig. 3). This modification highlights the need to elicit organizational support from the health care system and the local community to promote ACP engagement through the provision of ACP facilitating interventions such as TAP.

Revised conceptual framework of the Thinking Ahead Project. ACP, advance care planning; AD, advance directive; TAP, thinking ahead project.
Discussion
This pilot study investigated the feasibility of an intervention designed to increase ACP engagement among African Americans in the Deep South. This study contributes to the existing literature by (1) identifying perceived barriers and strategies that address barriers to ACP and (2) demonstrating feasibility of a theory-driven, multicomponent ACP intervention.
Given the unique historical and cultural issues that may negatively impact an individual's willingness to engage in ACP discussion, this study found that participants who had never been exposed to ACP discussions demonstrated a high level of interest in open discussions and early engagement. Once presented with a multicomponent intervention that addresses cultural, psychological, and cognitive factors involved in ACP discussions, participants were able to move beyond the barriers and be actively involved in the ACP discussions. This is evidenced by the findings that all participants (n = 30) endorsed increased intention to complete an AD at postintervention.
Feasibility data from both qualitative and quantitative analyses demonstrated successful implementation of the TAP intervention. Specifically, participants reported high satisfaction and confidence in completing an AD, suggesting that the TAP was well received by the current study sample. Another important finding indicated that participants from both health literacy levels (adequate versus limited) endorsed a preference for health-literacy adapted AD forms over the standard forms. While the sample size of participants with limited health literacy was relatively small, the findings were shown to be in accordance with a larger-scale study. Sudore et al. 23 reported that the adapted AD form was preferred among primary care patients (N = 205), especially those with limited literacy. The need for more ACP education is further highlighted by the perceived barriers endorsed by study participants. The lack of “informed education” is considered to be one of the primary barriers to African Americans' ACP engagement.
Our findings corroborate prior studies, in that provision ACP intervention showed improved engagement among racial minorities.24–28 It may be that the TAP would be similarly effective with African Americans in other geographic regions of the United States or with other racial/ethnic subsets of the U.S. population. The purpose of this study, however, was to focus on ACP discussions in the Deep South where racial disparities and poor health outcomes are most pronounced.9,12 It can be argued that demonstrating the feasibility and success of this intervention within the unique subset of African Americans suggests the potential of this approach to reduce health disparities and enhance better patient-provider communication more broadly.13,18
Several limitations of this pilot study should be noted, including the small sample size and geographic specificity of the study population. These limit the generalizability of the findings. Another limitation is the lack of a usual care control group to simulate situations where no ACP educational material is offered.
Future studies should consider a larger sample size to achieve adequate power and effect size. Additionally, using a longitudinal design (i.e., adding booster sessions to involve family members or health care proxies, and integrating medical chart review as follow-ups) can help track ACP discussions, AD documentation, and concordance between treatment preferences listed in the AD and treatment decisions made at the end of life. Finally, including other racial/ethnic minorities would enable better understanding of the complex nature of the relation between psychological, cognitive, and contextual factors of ACP and help decrease health disparities in end-of-life care.