
Abstract
Abstract
Background:
For patients with traumatic paraplegia, the ability to push up is a prerequisite for basic movements, including the transfer from bed to wheelchair. However, this movement may be contraindicated in patients with advanced cancer with bone metastases because of the risk of pain and pathologic fractures and muscle weakness resulting from cancer cachexia and disuse syndrome.
Objective:
The purpose of this study was to develop a method for transferring paraplegic patients from bed to wheelchair taking into consideration the unique characteristics of patients with advanced cancer with bone metastases and investigate the usefulness of said method.
Methods:
We developed a system for safe transfer from bed to wheelchair of paraplegic patients with advanced cancer consisting of horizontal transfer of the patient with safety apparatus utilizing an electric motor and potential energy. This method was used in 25 patients with advanced cancer and paraplegia. The activities of daily living (ADL), success/failure of transfer, ability for overnight stays outside the hospital, and possibility of discharge were investigated.
Results:
Use of the newly developed transfer method caused no difficulties and the ADL scores were significantly increased (p < 0.001). In all, 64% of the subjects could be transferred successfully from bed to wheelchair; 60% had successful overnight stays outside the hospital, and 48% could be discharged.
Conclusion:
Our findings suggest that the use of our newly devised system enables transfer from bed to wheelchair of even those patients with advanced cancer who cannot resume walking in the upright position because of paraplegia.
Introduction
T
However, the ability to push up, which is generally encouraged during the transfer of paraplegic patients, may be harmful in patients with advanced cancer for the following two reasons. First, bone metastases can cause severe pain thus discouraging any movements. Even if the pain is relieved by drug therapy during rest, it may recur during movement and these patients often cannot move by themselves. Second, even if the patients ignore the pain and move, pathologic fractures may occur because of reduced bone strength caused by the bone metastases. 7
For these reasons, moving patients with advanced cancer and paraplegia requires approaches that differ from the long-established approaches for patients with paraplegia caused by traumatic spinal cord injury. However, few studies have focused on the transfer approaches for patients with advanced cancer and paraplegia. 8 We report here a method that we developed for transferring paraplegic patients taking into consideration the unique characteristics of patients with advanced cancer. Furthermore, the usefulness of this method was investigated from the standpoint of provision of support, as much as possible, of the patients' independence.
Methods
This study was conducted at the palliative care unit of a comprehensive cancer center, with the approval of the ethical review board of the institution.
Development of the transfer method
A horizontal movement system was developed to enable the transfer of patients from bed to wheelchair without needing the patient to push up. The principle of this system was functional compensation, and the horizontal movement system was constructed by introducing pieces of a safety apparatus. A transfer board was used for movement in the horizontal direction, basically with the patient in the sitting position, without pushing up. No generation of muscle force was required as the power source for transfer, with the potential energy arising from a difference in height between the bed and the chair being used instead. Therefore, a bed vertically movable by an electric motor was used. A 24-hour pressure ulcer prevention-type cushion was used to prevent the development of pressure ulcers while on the wheelchair, because of the inability of the patients to push up.
The transfer procedure is shown in Table 1 and Figure 1. An occupational therapist stood behind the patient, checked the positions of the pieces of the safety apparatus, and the patient's movement procedures to prevent accidental falls.
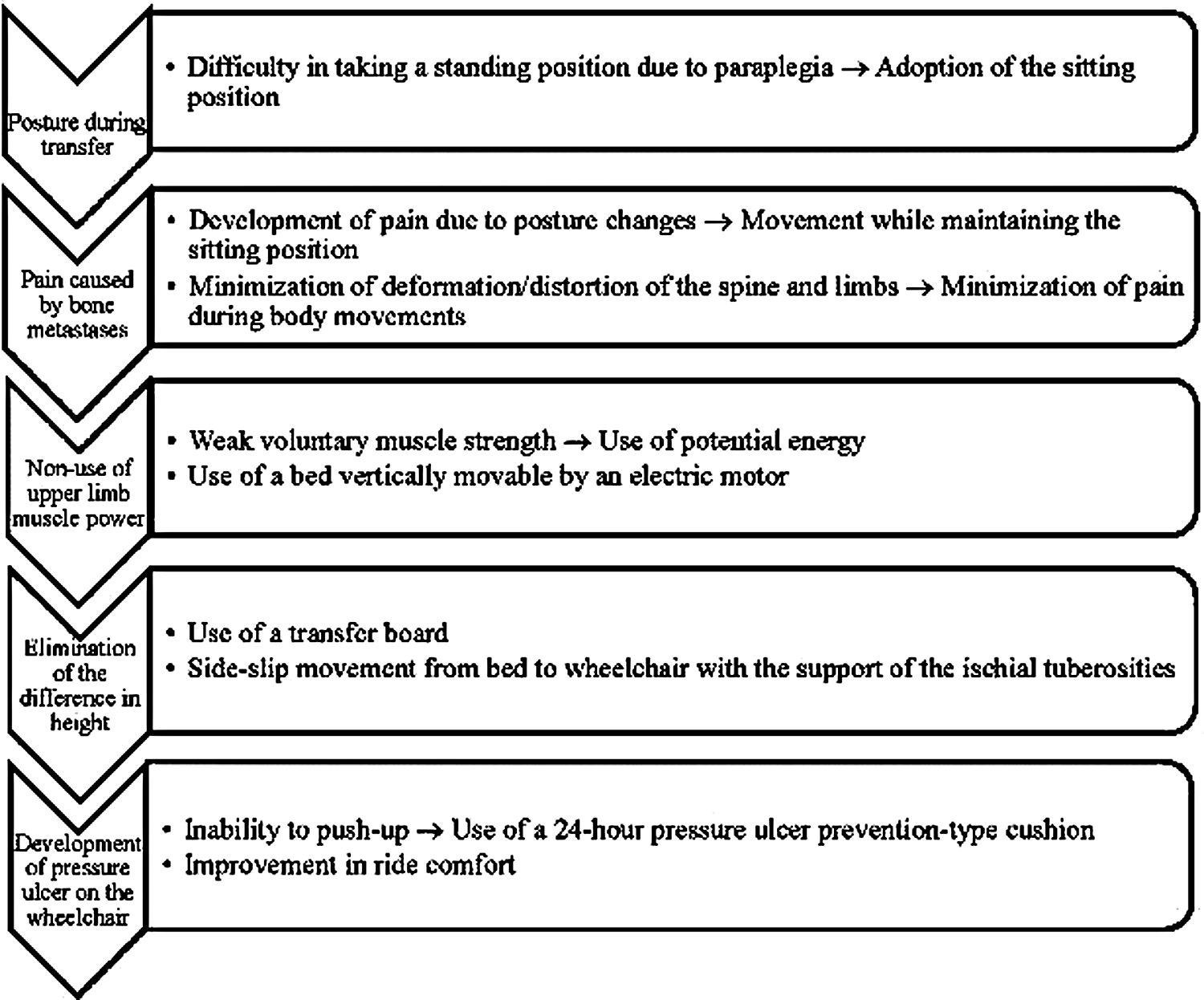
Steps to deliver a transfer method.
Subjects
The subjects were 25 patients with cancer hospitalized in the palliative care unit (11 males and 14 females; mean age, 50.8 years) who also had paraplegia caused by spinal metastases and were unable to transfer themselves from bed to wheelchair. The enrolled subjects had no disturbance of consciousness or cognitive impairment, could understand verbal explanations, and were not receiving any treatment that would prevent transfer. Prior to using this method, we confirmed that the subjects could remain in the sitting position at the edge of the bed and excluded those subjects who could not remain in this position for at least 1 second.
Evaluation methods
The Barthel index (BI) was used to evaluate the ADL. The BI is a widely used scale for assessing functional disability in basic ADLs. It comprises 10 basic activities (feeding, bathing, grooming, dressing, bowels, bladder, toilet use, transfers, mobility, stairs) with a total score ranging from 0 to 100 points. 9 A higher score means better capacity to perform daily living activities on the scale. In addition, we evaluated whether the subjects eventually became able to transfer themselves, could stay overnight outside the hospital, and could be discharged after they were trained in the use of this method.
The absence of normality in the data was confirmed and the changes in the BI scores after the intervention as compared with those before the intervention were evaluated using the Wilcoxon signed rank test. The probability value was two-sided, with a significance level of p < 0.05. The IBM SPSS Statistics, ver. 21.0 was used (IMB, Armonk, NY).
Results
The characteristics of the subjects and the results of the intervention are shown in Table 2.
Transfer from bed to wheelchair became possible for 23 of the 25 patients (92%); 16 (64%) eventually became able to transfer both from the bed to the wheelchair and from the wheelchair to the bed unassisted, while 7 (28%) could be transferred with assistance. In 2 of the 25 patients, the horizontal movement approach was unsuccessful: in the first case (case 4), the patient could maintain the sitting position at the edge of the bed for only 1 to 2 seconds and was actually unable to transfer himself in the sitting position. In the second case (case 13), the patient had severe ascites and the distended abdomen pressed against the diaphragm when the patient assumed the sitting position at the edge of the bed, causing dyspnea.
The BI scores increased after the intervention in all patients, and the median value increased significantly from 10.0 to 40.0 (p < 0.001).
Fifteen of the 25 patients (60%) had successful overnight stays outside the hospital. The primary reason why the remaining 10 patients could not stay was because they were not able to transfer from the wheelchair to the bed. On the other hand, only 12 patients (48%) could be discharged from the hospital. In most cases, the reason why the patient could not be discharged from the hospital was death from the primary disease. In addition, there were additional reasons other than the movement ability for the patients to be kept in the hospital, such as lack of acceptance by the family.
There were no adverse events associated with this intervention. When the transfer method using the transfer board was explained at the beginning of the intervention, half of the subjects expressed anxiety because they were unfamiliar with this method. However, they no longer expressed anxiety after the method was actually demonstrated to them. In addition, none of the patients complained of pain or developed pathologic fractures associated with the intervention.
Discussion
In recent years, the goal of maintenance and improvement of the environment for the treatment of patients with cancer has expanded the use of palliative care, and interventions with the aim of maintaining and improving the environment for treatment have also received attention in patients with advanced cancer.
Factors that prevent transfer movement from bed to wheelchair and vice versa in patients with advanced cancer include the pain associated with bone metastases 10 and risk of pathologic fractures caused by the physical stress caused by movement. 11 All 25 patients included in this study had well-controlled pain at rest and did not complain of pain before the start of the training for transfer. Pain in these patients is known to increase during body motion compared with that at rest, necessitating the use of rescue doses of analgesics. 12 However, such use of rescue doses may increase lightheadedness and sleepiness, making it difficult to perform the transfer movements. In the present method, none of the patients complained of pain or required rescue doses of analgesics during the intervention. Furthermore, none of the patients developed pathologic fractures in this study. This seems to be because the physical stress on both humeri, which are frequent sites of bone metastases, posed by pushing up was avoided, and furthermore, the body weight was dispersed by supporting the trunk on the two ischial tuberosities. Namely, it is likely to be because physical stress was decreased by provision of support at multiple points including the upper limbs and ischia, thereby decreasing bone distortion.
When a patient in the sitting position at the edge of the bed moves to a wheelchair, a horizontal plane has to be established to fill the difference in the height and the gap between the bed and the wheelchair. For this purpose, a transfer board that was developed in Sweden to transfer frail elderly was used.13–-15 Use of this board allows the patients to slide horizontally while maintaining the sitting position. Furthermore, because the horizontal plane of the board is smooth, frictional resistance is low during the horizontal movement, necessitating use of only a low level of energy for the transfer. Use of this horizontal movement system, the development of which took into consideration the unique characteristics of patients with advanced cancer, enabled transfer from bed to wheelchair for 23 of the 25 patients (92%) in this study. The patients got used to the movement method and no longer expressed anxiety after approximately three sessions, including the first that explained the transfer method. Of these, 28% could be transferred with the assistance of the staff during hospitalization, and 64% became able to transfer unassisted while the staff was only supervising them. The mean BI score for the item “transfer between wheelchair and bed” significantly increased from 10.2 before the intervention to 39.2 after the intervention. Furthermore, of the 23 patients who could be moved successfully with the use of the horizontal movement system, 60% were able to have successful overnight stays outside the hospital.
These results suggest that this method may improve the mobility and transfer of patients with cancer-related paraplegia who often express a desire to leave the bed, even at an advanced stage of the disease. Furthermore, the cost of the equipment is low, and it is also appropriate for home use if the patients can become proficient at this method.
There are, however, some limitations. First, one of the prerequisites for success of this transfer method is the patient's own ability to maintain the sitting position. When this method was developed, easy fatigability, which is a characteristic of patients with advanced cancer, could not be fully taken into account. Second, because patients have to learn a new method (i.e., horizontal transfer) that they have not experienced before, this method cannot be applied to patients with low learning ability and those with impaired consciousness. Finally, pieces of the safety apparatus, such as a bed, board, and wheelchair have to be prepared and adequate bedside space is required. Based on such a physical environment, the presence of staff who can educate patients about the transfer method is indispensable. While resolving these limitations, it will be necessary to expand the number of subjects and improve the validity and universality of this transfer method.
Footnotes
Author Disclosure Statement
No competing financial interests exist.