
Abstract
Abstract
Importance:
Evidence supports palliative care effectiveness. Given workforce constraints and the costs of new services, payers and providers need help to prioritize their investments. They need to know which patients to target, which personnel to hire, and which services best improve outcomes.
Objective:
To inform how payers and providers should identify patients with “advanced illness” and the specific interventions they should implement, we reviewed the evidence to identify (1) individuals appropriate for palliative care and (2) elements of health service interventions (personnel involved, use of multidisciplinary teams, and settings of care) effective in achieving better outcomes for patients, caregivers, and the healthcare system.
Evidence Review:
Systematic searches of MEDLINE, EMBASE, PsycINFO, Web of Science, and Cochrane Database of Systematic Reviews databases (1/1/2001-1/8/2015).
Results:
Randomized controlled trials (124) met inclusion criteria. The majority of studies in cancer (49%, 38 of 77 studies) demonstrated statistically significant patient or caregiver outcomes (e.g., p < 0.05), as did those in congestive heart failure (CHF) (62%, 13 of 21), chronic obstructive pulmonary disease (COPD; 58%, 11 of 19), and dementia (60%, 15 of 25). Most prognostic criteria used clinicians' judgment (73%, 22 of 30). Most interventions included a nurse (70%, 69 of 98), and many were nurse-only (39%, 27 of 69). Social workers were well represented, and home-based approaches were common (56%, 70 of 124). Home interventions with visits were more effective than those without (64%, 28 of 44; vs. 46%, 12 of 26). Interventions improved communication and care planning (70%, 12 of 18), psychosocial health (36%, 12 of 33, for depressive symptoms; 41%, 9 of 22, for anxiety), and patient (40%, 8 of 20) and caregiver experiences (63%, 5 of 8). Many interventions reduced hospital use (65%, 11 of 17), but most other economic outcomes, including costs, were poorly characterized. Palliative care teams did not reliably lower healthcare costs (20%, 2 of 10).
Conclusions:
Palliative care improves cancer, CHF, COPD, and dementia outcomes. Effective models include nurses, social workers, and home-based components, and a focus on communication, psychosocial support, and the patient or caregiver experience. High-quality research on intervention costs and cost outcomes in palliative care is limited.
Background
T
The term “palliative care” signifies both an approach to care and specific health services, including consultation and hospice, among many others. The Institute of Medicine (IOM) defines palliative care as “care that provides relief from pain and other symptoms, supports quality of life, and is focused on patients with serious advanced illness and their families” 1 and, in a seminal report on the quality of end-of-life care, 1 called for efforts to incorporate palliative care principles into education, payment and delivery models, and public awareness campaigns. The IOM report underscores the need for broad efforts to improve palliative care access for patients with advanced illness and their families.
To be successful, recommendations to improve access to palliative care will require specificity to inform how policymakers, payers, and providers should operationalize “advanced illness” and the specific interventions they should implement. Although there are good general recommendations for who should receive palliative care, it is often not clear how rigorously those recommendations have been tested in practice. To address these issues and inform policy, payment, and practice, we characterized the evidence base focusing on randomized controlled trials (RCTs) published since 2001. We addressed the following questions:
• What populations are appropriate for palliative care? • What health service interventions and intervention elements improve aspects of patient and/or caregiver quality of life, healthcare use, and healthcare costs?
Methods
To identify the most rigorous sources of published evidence to inform interventions, we systematically reviewed published RCTs that addressed (1) advanced illness populations of patients and/or caregivers for whom palliative and end-of-life care should be considered; (2) effective palliative and end-of-life care interventions, including specific intervention components; and (3) the impact of palliative and end-of-life interventions on quality of life, healthcare use, and healthcare costs. Our search encompassed January 1, 2001, to January 8, 2015.
Data sources and searches
A research librarian searched MEDLINE, EMBASE, PsycINFO, Cochrane Database of Systematic Reviews, Web of Sciences Databases (SCI-EXPANDED, SSCI, A&HCI, CPCI-S, and CPCI-SSH), and the CareSearch Palliative Care Knowledge Network Review Collection. 3 We derived our primary literature search strategy from the NIH State of the Science Meeting on End of Life Care in 2004 4 (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/jpm). The original search encompassed terms for (1) specific diseases and debility associated with advanced illness and (2) domains and specific terms for HRQOL; we expanded it to include economic outcomes, which we defined as healthcare use, healthcare costs, and site of death.
We conducted an original review covering 2001 to 2013 and later updated it to include 2013 to 2015. We originally searched from January 1, 2001, to March 8, 2013, and identified RCTs in four ways: (1) directly from literature searches; (2) from reference lists in systematic reviews identified in searches with AMSTAR ratings of at least six 5 ; (3) from accepted studies in reviews we had previously conducted for an American College of Physicians guideline 6 ; (4) from systematic reviews that informed the development of the Assessing Care of Vulnerable Elders (ACOVE) quality measures and the Cancer Quality Assessing Symptoms Side Effects and Indicators of Supportive Treatment (ASSIST) quality indicators.7–11
To update the review to January 2015, we reviewed title pages to identify all original research articles and systematic reviews published between March 2013 and January 8, 2015, in the New England Journal of Medicine, Journal of the American Medical Association, Annals of Internal Medicine, British Medical Journal (BMJ), Journal of Clinical Oncology, Journal of Pain and Symptom Management, Journal of the American Geriatrics Society, Journal of Palliative Medicine, Palliative Medicine, BioMed Central Palliative Care, and BMJ Supportive & Palliative Care. We identified RCTs published in these journals and from reference lists in systematic reviews with AMSTAR ratings of at least six. 5 We did not search gray literature. 2
Study selection
Inclusion criteria were as follows:
• Adults ≥18 years old with advanced illness, and/or their caregivers • Health service interventions addressing patient and/or caregiver quality-of-life-related elements in intervention design and/or as outcomes • Cancer, heart failure and other cardiac conditions, chronic pulmonary disease, dementia and other neurological conditions, end-stage liver disease, or end-stage renal disease, or any advanced illness populations receiving palliative care, hospice, or end-of-life care • Randomized controlled trials • Published between January 1, 2001, and January 8, 2015.
We used Cochrane Collaboration definitions of study designs and attributes. We defined health service interventions using the World Health Organization's definition of a health service. 12 We defined quality of life and its related elements consistent with, but expanding upon, our previous work on this topic. 4 In this study, we considered it to include HRQOL; pain, dyspnea, depressive symptoms, anxiety, and other symptoms; functional status; existential or spiritual well-being; communication with patients or families, including prognostication and care planning; continuity, defined as relationships with providers over time; experience or satisfaction; caregiving, including nonprofessional activities that address emotional, spiritual, practical, or medical aspects of support; and bereavement care for caregivers or other loved ones.
We excluded (1) non-English publications; (2) studies that were not conducted in the United States, Western Europe, Israel, Canada, Australia, or New Zealand; (3) studies with only qualitative data; (4) studies of economic outcomes only; (5) studies of drugs, devices, or technical care if they were not part of a health service intervention; and (6) studies of only support groups or psychological interventions unless they addressed an aspect of health service delivery (e.g., in-person versus remote support).
Data extraction and quality assessment
Our multidisciplinary review team possessed extensive experience in palliative care and review methods. Following definition of review goals, procedures, and inclusion and exclusion criteria, teams of paired reviewers conducted title, abstract, and full-text reviews on all RCTs and systematic reviews. Review forms reflected the study's aims and conceptual framework (i.e., population categories, quality-of-life-related elements, and intervention attributes). At all stages, review forms were reviewed and piloted. Weekly team discussions resolved conflicts and clarified review procedures, with adjudication by senior team leaders. A single reviewer screened all accepted RCTs for bias using a Cochrane risk of bias tool modified for a previous systematic review of palliative care.13–16
Data synthesis and analysis
Because of the heterogeneity of included studies and review outcomes, we determined that a meta-analysis was inappropriate. Instead, we qualitatively synthesized evidence according to the patient and caregiver populations, intervention elements, and quality-of-life-relevant and economic outcomes of included studies. We assessed consistency of evidence through the total numbers of studies that addressed each category of interest and the frequency of positive results within each category. We assessed directness of evidence by evaluating (1) the extent to and manner in which populations were characterized and (2) whether the literature shed light on quality-of-life-relevant outcomes. 17
We characterized “strength of evidence” for outcomes of interest by qualitatively synthesizing the number and quality of studies that addressed each outcome, study population sizes, and effect sizes. Our assessment of evidence strength is a relative one that compares outcomes within the body of accepted RCTs in this review.
Studies often analyzed more than one outcome (e.g., pain, depressive symptoms, and functional status) and operationalized outcomes using more than one measure (e.g., average pain, worst pain, and least pain). We considered an intervention to have a “significant” effect on an outcome if a majority of that outcome's measures were statistically significant (e.g., two of three pain measures were statistically significant). Similarly, we considered an intervention as a whole to be “significant” if it had statistically significant effects on a majority of its outcomes (e.g., a study that analyzed pain, depressive symptoms, and functional status, and pain and depressive symptoms were statistically significant).
Results
Literature flow
In our original review, we identified 14,961 titles from primary searches and reference mining. We identified 3342 potentially relevant abstracts and 629 potentially relevant articles, and accepted 99 RCTs. In our update review, we identified 3647 titles from the title pages of 11 major journals and reference mining of systematic reviews in these journals (Fig. 1). We identified 71 potentially relevant abstracts and 68 potentially relevant articles, and accepted 25 RCTs. We accepted a total of 124 RCTs in our original and update reviews combined. The summary characteristics of these studies, as well as a list of relevant acronyms used by these studies, are provided in Supplementary Tables 2 and 3; Supplementary Data are available online at www.liebertpub.com/jpm
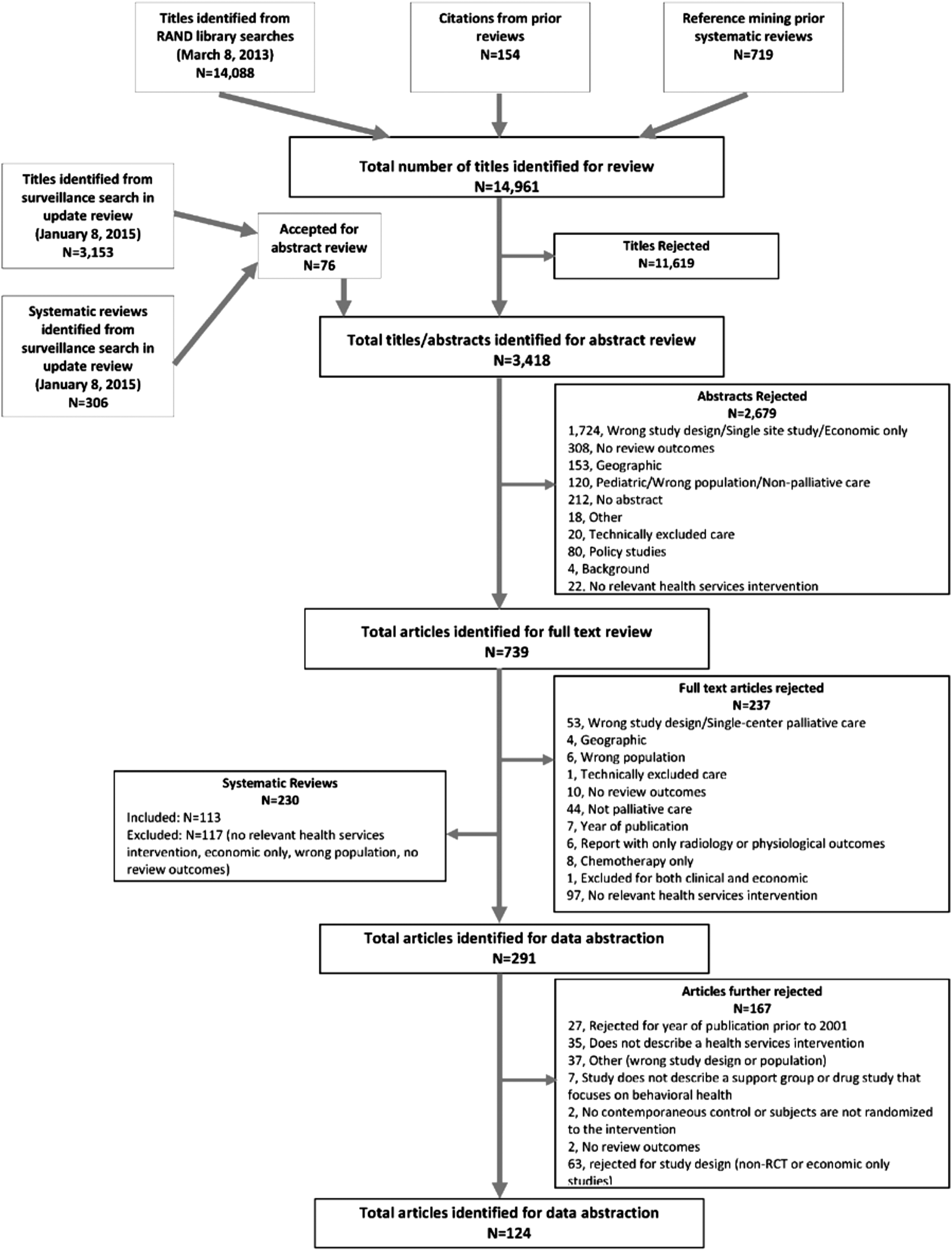
Literature flow. RCT, randomized controlled trial.
Intervention populations and characterizing advanced illness
Conditions of study participants
Table 1 presents the patient populations in the included studies. Ninety-three percent of all studies (115 of 124) described the conditions of their participants. Cancer was the most-studied condition, followed by dementia, congestive heart failure (CHF), and chronic obstructive pulmonary disease (COPD). Of the studies with conditions described, 83% (95 of 115) included only one condition. Cancer and dementia were overwhelmingly studied alone: 84% (65 of 77) and 88% (22 of 25), respectively, of studies that included these conditions did not include any other conditions. By contrast, 76% (16 of 21) and 84% (16 of 19), respectively, of studies that included CHF and COPD included at least one other condition.
Each percentage is calculated for each category in relation to its parent category.
CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease.
For the most commonly studied conditions, 62% (13 of 21) and 58% (11 of 19) of interventions for CHF and COPD, and 49% (38 of 77) and 60% (15 of 25) of interventions for cancer and dementia, had a majority of significant results.
Among cancer studies, interventions for metastatic cancer were more likely to have a majority of significant results than those for nonmetastatic cancer, as were interventions for patients receiving disease-directed treatment (curative chemotherapy and/or radiotherapy) compared with no treatment: 59% of interventions for metastatic cancer (20 of 34), compared with 42% of interventions for nonmetastatic cancer (18 of 43), demonstrated a majority of significant results; similarly, 58% of interventions for cancer being treated with chemotherapy and/or radiotherapy (15 of 26), compared with 45% of interventions for cancer not being treated with these modalities (23 of 51), had a majority of significant results.
Additional characterization of intervention populations may be found in the Appendix.
Intervention elements
Intervention personnel
Nurses, including advanced practice nurses, were the most common clinical discipline to deliver interventions: 70% (69 of 98) of interventions included a nurse, and 39% of these interventions (27 of 69) were delivered only by nurses (Table 2). Nurse-only interventions, or interventions with nurses in primary roles, involved palliative case management,18–25 education in symptom management and monitoring,26–40 and/or counseling and therapy,27,41,42 and were overwhelmingly delivered at home (85% of nurse-only interventions [23 of 27] included home visits and/or telephone calls).
Each percentage is calculated for each category in relation to its parent category.
“Other” includes a heterogeneous set of teams such as a heart failure management team and a multidisciplinary team for patients who did not yet qualify for palliative or hospice services. No two studies in this category used the same type of team.
“Other” includes a heterogeneous set of technological intervention components such as a technology-based heart failure monitoring system. No two studies included in the “other” category used the same technology component.
EHR, electronic health record; IQR, interquartile range.
Fifty-two percent of interventions that included a nurse (36 of 69) demonstrated a majority of significant results, compared with 58% of interventions that did not include a nurse (32 of 55). This pattern was similar for nurse-only interventions: 52% of interventions that were nurse-only (14 of 27) demonstrated a majority of significant results, compared with 56% of interventions that included nurses and other personnel (54 of 97).
Multidisciplinary teams
Twenty-six percent of studies (32 of 124) employed multidisciplinary teams. Sixty-six percent of teams (21 of 32) included three or more types of clinically trained individuals; 94% (30 of 32) included a nurse and 50% (16 of 32) included a social worker. Social workers were part of clinically diverse teams: 100% of multidisciplinary teams that included a social worker (16 of 16) included three or more different types of clinically trained individuals. Receiving care from a palliative care team (versus usual care) comprised 56% of all interventions involving palliative care teams (10 of 18)43–52 ; the remainder was a heterogeneous set of interventions delivered alongside palliative consultation or in the context of palliative care (e.g., delivering dignity therapy to patients already receiving care from a palliative care team, or delivering a multifaceted intervention of which a palliative care team was one component).53–60
Interventions without multidisciplinary teams often addressed more limited goals than team-based interventions (e.g., nurse-directed pain management versus comprehensive, team-based patient and family support). 61
Intervention settings
Home was the most common intervention setting, followed by outpatient clinics and inpatient hospitals (Table 2). In addition to the nurse-led, home-based interventions described above, interventions delivered at home also involved caregiver and family support and training.56,59,62–72 Sixty-six percent of home interventions (46 of 70) did not involve any other settings, 63% (44 of 70) involved home visits by intervention personnel, and 59% (41 of 70) involved the use of a telephone. Sixty-four percent of interventions that included home visits (28 of 44), compared with 46% of home interventions without visits (12 of 26), demonstrated a majority of significant results.
Sixty-one percent of interventions delivered in a hospital (11 of 18) involved at least one other setting, and 56% of interventions with a hospital component (10 of 18) were delivered by palliative care teams.43–48,51,52,54,58 Interventions delivered in outpatient clinics were heterogeneous, ranging from disease and symptom management education39,61,73–79 to counseling and therapy.41,42,77,80,81 Outpatient clinics were often one of many settings in multisetting, multicomponent interventions.
Supporting technology
Forty-eight percent of all interventions (59 of 124) involved a technology component, most often a telephone to enable remote delivery of interventions and/or supportive check-in calls. Only three studies used audio- or video-based telehealth technology,22,65,82 two studies used electronic health record (EHR)-based tools,83,84 and two studies used mobile phones or tablets.39,85 Sixty-one percent of interventions that included a telephone component (31 of 51), compared with 51% of interventions that did not include a telephone component (37 of 73), demonstrated a majority of significant results.
Quality-of-life-relevant outcomes
Patient outcomes
Seventy-seven percent of studies (96 of 124) addressed patient quality-of-life-relevant domains, ranging from 11% (11 of 96) for existential or spiritual concerns to 42% (40 of 96) for other symptoms (all symptoms other than pain, dyspnea, depressive symptoms, and anxiety) (Table 3). Approximately 20%–30% of studies that addressed pain (9 of 37),28,29,42,51,60,61,75,83,86 dyspnea (3 of 14),24,53,87 functional status (12 of 37),21,42,57,67,69,74,88–93 and HRQOL (10 of 38)18,49,64,66,85,90–92,94,95 had a majority of significant results in each of those domains; these frequencies were ∼40%–50% for studies that addressed depressive symptoms (12 of 33),18,35,49,50,58,66,69,82,96–99 anxiety (9 of 22),35,37,53,55,58,69,78,94,100 other symptoms (15 of 40),21,35,37,49,57,60,77–79,88,91,94,101–103 existential or spiritual concerns (4 of 11),53,87,103,104 patient experience or satisfaction (8 of 20),20,23–25,43,44,105,106 and ∼70% for communication or care planning (12 of 18).31,44,49,53,88,104,106–111 Of studies that addressed patient quality-of-life-relevant outcomes, 45% (43 of 96) demonstrated a majority of significant results in the majority of quality-of-life-relevant domains.
Other symptoms include all symptoms other than pain, dyspnea, depressive symptoms, and anxiety (e.g., fatigue, anorexia, nausea, and diarrhea).
HRQOL, health-related quality of life; QOL, quality of life.
Caregiver outcomes
Forty-two percent of studies (52 of 124) addressed caregiver quality-of-life-relevant domains. The range of these studies that addressed individual domains was 6% (3 of 52) for existential or spiritual concerns to 40% (21 of 52) for depressive symptoms. No studies that addressed existential or spiritual concerns (0 of 3) had a majority of significant results in each of those domains; this frequency was ∼30% for studies that addressed anxiety (2 of 6),112,113 40% for studies that addressed HRQOL (3 of 7),31,36,66 60%–70% for studies that addressed depressive symptoms (12 of 21),62–64,66,70,71,80,112–116 other symptoms (all symptoms other than pain, dyspnea, depressive symptoms, and anxiety) (5 of 8),31,62,112,116,117 and caregiver experience or satisfaction (5 of 8),25,48,104,106,118 and 75% for communication or care planning (3 of 4).31,72,119 Of studies that addressed caregiver quality-of-life-relevant outcomes, 60% (31 of 52) demonstrated a majority of significant results in the majority of quality-of-life-relevant domains.
Relationships among key study characteristics and select quality-of-life-relevant outcomes
Sixty-one percent of interventions that addressed patient symptoms (59 of 96) were delivered only to cancer patients. Patient pain and depressive symptoms were a common focus in cancer studies but less commonly addressed in other conditions.20,24,52,53,66,82,87,100,102,120 Interventions that addressed pain and depressive symptoms in cancer patients were much more effective than those that addressed pain and depressive symptoms in other conditions: no interventions demonstrated significant results for pain, and only two for depressive symptoms,66,82 in CHF, COPD, or dementia.
Interventions with a significant effect on patient pain (nine studies)28,29,42,51,60,61,75,83,86 were usually delivered to cancer patients (78% [7 of 9] included only cancer patients)28,29,42,61,75,83,86 and specifically designed to address cancer pain, usually involved pain education and management, were short term (33% [3 of 9], were one-time interventions,60,61,86 and none exceeded six weeks). Nurse-only interventions were particularly effective at reducing pain: 44% of all interventions that reduced pain (4 of 9) used only nurses.28,29,42,83
In contrast to pain, interventions that had a significant effect on patient depressive symptoms (12 studies)18,35,49,50,58,66,69,82,96–99 were heterogeneous in terms of settings, use of multidisciplinary teams, clinical disciplines, duration, and focus; case management, palliative care teams, hospice, skills training, and other interventions were all effective. Interventions with significant effect on caregiver depressive symptoms (12 studies),62–64,66,70,71,80,112–116 by contrast, often involved a home component (83% [10 of 12]),62–64,66,70,71,113–116 did not use multidisciplinary teams, were long term (average duration 1.2 years), and often involved caregiver skills training63,64,71,113 or counseling and therapy.62,66,70,114–116 The use of mental health professionals also differed between effective interventions in patient versus caregiver depressive symptoms: 86% of interventions (6 of 7)64,70,80,114–116 that used mental health professionals and addressed caregiver depressive symptoms were effective, compared with 0% of interventions (0 of 7) that used mental health professionals and addressed patient depressive symptoms.
Interventions with significant effect on patient HRQOL (10 studies)18,49,64,66,85,90–92,94,95 were generally more comprehensive in focus. They ranged from case management18,90,91 to caregiver training, 64 occupational therapy, 66 quality-of-life questionnaire completion,85,95 and a hospital-to-home transitional care program. 90 Forty percent (4 of 10)49,91,92,94 involved a multidisciplinary team, and all were delivered in outpatient settings and/or at home.
Interventions with a significant effect on patient and/or caregiver communication or care planning outcomes (14 studies)31,53,72,88,104,106–111,119 often included decision support,88,106,108,109,119 advance directive completion,53,88,106 education and/or communication training,31,72,104,110 and case management components.53,88,106 Seventy-one percent of interventions that included a nurse (5 of 7)31,44,49,53,88 and addressed patient communication or care planning outcomes had a significant effect on these outcomes; 100% of interventions that included a social worker (4 of 4)44,53,88,104 and addressed patient communication or care planning outcomes had a significant effect on these outcomes. Only 7% of interventions (9 of 124) involved decision support, but 56% of these (5 of 9)88,106,108,109,119 had a significant effect on communication or care planning outcomes. This pattern was similar for advance directive completion: only 5% of interventions (6 of 124) involved advance directive completion, but 50% of these (3 of 6)53,88,106 had a significant effect on communication or care planning outcomes.
Interventions with a hospital component focused on patients with a greater burden of illness than those without a hospital component: many were in advanced stages of cancer, CHF, or COPD, and 44% of these interventions (8 of 18)43–45,48,54,58,62,112 were delivered to patients determined by clinicians to have a poor prognosis (in one case within days of death). 112 These interventions were generally less effective than those without a hospital component.
Longer interventions tended to be more effective for patient depressive symptoms and anxiety (56% of interventions [11 of 18]18,35,49,50,53,55,69,78,82,96,98 with significant effects on these outcomes lasted at least 12 weeks) and patient and caregiver quality of life (75% of interventions [9 of 12]18,31,49,64,85,90–92,95 with significant effects on these outcomes lasted at least 12 weeks).
Economic outcomes
Healthcare use
Forty-one percent of studies (51 of 124) addressed economic outcomes (Table 4). Healthcare use was the most frequently studied, followed by costs and drugs. Hospital use was the most well-studied utilization outcome: 65% of studies with a significant effect on healthcare use (11 of 17)23,24,43,44,57,74,89,91,102,104,118 had effects on CHF-related and all-cause hospital readmissions and length of stay. Emergency department (ED) use was also relatively well studied, but only 31% of interventions (4 of 13) had a significant effect on it.22,43,82,90 Fifty-three percent of interventions with a significant effect on healthcare use (9 of 17)22–24,53,57,74,89–91 included a case management component, and many included education57,74,104 and disease and symptom management40,82,102 components. Only four studies addressed hospice use.24,43,44,118
CPR, cardiopulmonary resuscitation; ICU, intensive care unit.
Healthcare costs
Of the studies that addressed healthcare costs, 74% (14 of 19)23–25,44,83,89,91–93,105,106,117,121,122 reported intervention costs; however, only 50% of these (7 of 14)25,89,92,93,117,121,122 incorporated intervention costs into statistical tests for intervention efficacy in lowering costs or in cost-effectiveness analyses. Thirty-two percent of studies that addressed healthcare costs (6 of 19)22,43,44,89,92,96 demonstrated significant effects on cost outcomes or cost-effectiveness. Interventions tended to be more successful in lowering specific costs (36% of interventions that addressed specific costs [4 of 11]22,44,89,96 significantly reduced these costs) than in lowering overall costs of care (20% of interventions that addressed overall costs [3 of 15]43,44,92 significantly reduced these costs). Specific costs reduced included hospital readmission,44,89 ED, 22 and pharmacologic89,96 costs.
Interventions that lowered costs included participants from a variety of clinical disciplines (83% [5 of 6])43,44,89,92,96 included at least three clinical disciplines). Nurses and social workers were well represented among these interventions: all of these interventions included a nurse, and 67% of them (4 of 6)43,44,92,96 included a social worker. Palliative care teams had little effect on costs: only 20% of interventions in which the intervention itself was the palliative care team (2 of 10)43,44 reduced healthcare costs.
Discussion
We identified many RCTs of palliative and end-of-life health service interventions with the strongest evidence for interventions in cancer, CHF, and COPD. We found the strongest evidence for the roles of nurses and social workers, strong evidence for home-based components, and moderate evidence for multidisciplinary approaches. In terms of quality-of-life-relevant outcomes for both patients and caregivers, we found the strongest evidence for palliative and end-of-life services in improving communication and care planning, moderate evidence for improving psychosocial health and the patient and caregiver experience, and weaker evidence for improving HRQOL, pain, dyspnea, functional status, and existential or spiritual concerns. In terms of economic outcomes, we found moderate evidence relevant to reducing hospital use, weaker evidence for palliative care in reducing other specific healthcare use, and moderate evidence for effectiveness in lowering healthcare costs. We found weak evidence for palliative care teams specifically in reducing healthcare costs.
The strategy of identifying patients for palliative care by eliciting clinician-reported risk was a common and generally effective approach. It is prudent, relatively simple to implement, and may foster buy-in. 123 However, there are also drawbacks to clinician-reported risk, including lack of familiarity with palliative health services and bias against referral to those services. The literature was silent on innovative approaches that contemporary entrepreneurs, payers, and providers are taking to identify high-risk patients who might be targeted for palliative care. These include data mining that combines health and consumer information and novel sensor technologies that characterize function and high-risk events (e.g., falls).
Palliative and end-of-life services were most frequently studied in cancer populations. In general, studies of cancer focused on very sick patients, identified by severity (e.g., metastatic cancer) or clinician-identified poor prognosis. We found evidence for the effectiveness of interventions in cancer, supporting a recent American Society of Clinical Oncology guideline's and other calls for integrating palliative care in advanced cancer. 124 While cancer was most frequently studied, we also found evidence supporting the application of palliative care to other advanced illnesses (CHF, COPD, and dementia) and to mixed populations.
The literature supports various models for palliative care delivery. Evidence supports the role of nurses and social workers in teams and working alone. Our findings underscore the value of home services, whether in-person or by telephone, and the role of nurses and social workers in home-based care. Integrated payment and delivery may improve support for nurses and social workers, 125 who play crucial roles in communication and coordination. For example, two-thirds of Physician Orders for Life Sustaining Treatment in Oregon are completed in nursing homes by social workers. 126
Our review generally supported the ability of palliative services to promote effective communication and deliver symptomatic support. The evidence is strongest for care planning and psychological outcomes, consistent with the results of clinical systematic reviews. 2 The recent IOM report on death and dying has a special emphasis on communication and advance care planning that is appropriate, given the evidence supporting this practice area. 1 We found that decision support and advance directive completion should be considered a facilitative component of this emphasis.
We found that the use of mental health professionals was effective for depressive symptoms in caregivers but not in patients. Our review excluded studies of psychological interventions unless they addressed an aspect of health service delivery (e.g., in person versus remote counseling). As such, our results are not a comment on the overall efficacy of mental health professionals in all palliative settings, in which psychotherapy, counseling, and medication are known to be effective for patient depression. This finding may be explained by the fact that interventions for caregiver depression on the whole lasted much longer than those for patient depression. Long-term interventions are known to be more effective for depression than short-term ones. 127
We found minimal healthcare use and cost reductions for palliative care in general (aside from hospital use) and palliative care teams specifically. Other reviews demonstrated an advantage for the latter but have included lower quality study designs, 128 and a recent high-quality RCT of a palliative care team that demonstrated clinical benefit and lower healthcare use failed to demonstrate a cost advantage. 129 That said, our economic results likely reflect a lack of evidence rather than a lack of effect, as the included studies had very significant shortcomings in characterizing economic outcomes. Their measurement of these outcomes was heterogeneous and they often failed to account for various dimensions of cost or use. Our results call for much higher quality economic research.
We faced several limitations. First, we focused on health service interventions only, so our review does not encompass the full range of effective interventions that palliative care teams and providers are capable of delivering. Second, our definition of what constitutes “palliative care” was not limited to a specialty service and could have increased the heterogeneity of included articles, both because of the subjectivity of the definition and inconsistent indexing in the literature. However, our approach improves the generalizability and applicability of our findings. Third, we limited our review to studies of adults aged 18 years and older due to concerns about feasibility, given that our literature searches in the adult population identified nearly 15,000 titles. Pediatric end-of-life populations are equally deserving of attention, and future systematic reviews of palliative health services should focus on this population. Fourth, we limited our included studies to RCTs, which excluded observational and qualitative study designs. These types of studies can offer valuable information, particularly in end-of-life populations, whose vulnerability poses challenges for conducting RCTs. However, our goal was not to incorporate all available evidence, but rather to synthesize the highest quality evidence. Future systematic reviews of palliative health services should focus on observational and qualitative study designs.
In summary, our review underscores the importance of the recent IOM report and its call to more broadly implement palliative and end-of-life care. It supports an emphasis on cancer, chronic cardiopulmonary conditions, and dementia; highlights the importance of nurses and social workers, multidisciplinary approaches, and interventions that encompass the home; and reinforces the focus on improving communication and psychosocial support. It also highlights the need for much more rigorous and comprehensive research to understand the impact of palliative care on healthcare costs.
Footnotes
Acknowledgments
The authors thank Paul Shekelle, MD, PhD, for consulting on methodological approaches to this topic, and Keegan Wood, BSN, for helping to prepare the evidence tables for publication. All authors had full access to all of the data and take responsibility for the integrity of the data and the accuracy of the data analysis.
Grant Support: This work was supported by grant R01 NR013372 from the National Institute of Nursing Research, a Cambia Health Foundation Sojourns Award, and the California HealthCare Foundation. Dr. Singer received support from grant T32 GM008042 as a member of the Medical Scientist Training Program at the University of California, Los Angeles. Dr. Walling received support from the NIH/National Center for Advancing Translational Science (NCATS) UCLA CTSI grant UL1 TR000124 and the NIH loan repayment program.
Disclaimer: The views expressed are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the US government.
Author Disclosure Statement
No competing financial interests exist.
Appendix: Additional Description of Studies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.