
Abstract
Abstract
Background:
Bereavement support is a core tenet of palliative care that may prove difficult for clinicians as it is time-consuming, emotionally charged, and not emphasized in pediatrics training. This project is intended to describe the opinions, knowledge, and practice of bereavement care among pediatric oncologists to identify gaps in clinical care.
Procedures:
An internet-based survey instrument was pilot tested, refined, and distributed to pediatric oncologists in the United States. Statistical analysis was performed using SAS 9.2.
Results:
Electronic surveys were distributed to 2,061 pediatric oncologists and 522 surveys (25%) were fully completed. Participants were asked how likely they are to engage in particular bereavement activities (phone calls, condolence cards, memorial services, family meetings, or referrals for counseling) following the death of a pediatric cancer patient. Eighty-two percent of participants, at least, sometimes engage in at least one of these activities. Being female, an attending physician, and increased time in clinical practice were predictive of active participation in bereavement care. Nearly all participants (96%) believe that bereavement care is part of good clinical care, while 8% indicate that bereavement support is not their responsibility. Lack of time and resources were the biggest barriers to providing bereavement support.
Conclusions:
The majority of pediatric oncologists engage in clinical practices to support bereaved families. Lack of time and physical resources pose significant barriers to clinician's efforts. Additional supports should be explored to increase pediatric oncology physician uptake of bereavement care practices.
Introduction
B
Among children and young adults ages 0–24 years, cancer accounts for about 5% of deaths in the United States. Pediatric oncologists are therefore in a unique position to care for families coping with a child's death. 18 There has been very little research examining how pediatric oncologists address the bereavement needs of patient's families, although new guidelines indicate that bereavement care should be standard for pediatric oncology patients. 19 Many medical institutions allocate resources to palliative care services, which may include bereavement support, but these programs have varying degrees of physician participation in bereavement. 20 Previous research has indicated that parents are grateful when physicians acknowledge their child's death by sending condolence cards, attending memorial services, or meeting with parents.21,22 It is unknown if these interventions improve health outcomes, but they do reflect the importance of compassion from a child's medical provider to a bereaved family. 14 When bereavement care is absent, surviving family members may express feelings of abandonment and decreased satisfaction with care. 23
The objective of this study is to define how pediatric oncologists in the United States engage in bereavement care following the loss of a child to cancer. To our knowledge, this is the first study conducted regarding bereavement care in this specific population. Physicians were queried about available institutional resources and barriers that prevent them from providing bereavement care. Physician-specific traits and attributes that may be associated with engagement in bereavement care were assessed.
Methods
Study population and participant recruitment
Eligible study participants were pediatric oncology physicians who are currently providing clinical care to children with cancer within the United States. Potential participants were identified by an internet-based search of medium to large medical centers with pediatric oncology programs. We defined “medium to large” programs as those that participate in the largest pediatric oncology clinical trial organization in United States (Children's Oncology Group). An internet search was conducted to obtain e-mail addresses of physicians at these academic sites. All physicians with available addresses were included. Initial basic questions assured that responding physicians fit the inclusion criteria as above
Survey instrument
The survey instrument was developed according to the Tailored Method of Survey design by Dillman et al.24,25 A subset of questions were based (with permission) on a survey tool utilized in a study of bereavement practices of oncology and radiation oncology physicians caring for adult patients by Chau et al. 16 Additional questions were developed specifically for pediatric physicians to assess beliefs and attitudes regarding their role in providing bereavement support. The survey was pilot tested with a group of pediatric oncologists to ensure clarity and refined based on feedback. Questions that addressed physician opinions, beliefs, attitudes, and frequency of participation in bereavement activities were formulated using a 5-point Likert scale.
The survey was electronically formatted and sent to participants using Research Electronic Data Capture (REDCap), a secure web-based data system developed for clinical research in academic institutions. An introductory e-mail was sent to potential participants followed by an Internet link to the survey. Two reminder e-mails were sent to nonresponders at approximately four-week intervals. This study was reviewed and approved by the University of Utah Institutional Review Board.
Data collection and statistical analysis
Data were captured in REDCap and analyzed using SAS 9.2 (SAS, Inc., N.C.). Descriptive statistics are reported as frequencies and counts for categorical variables. Means and standard deviations are reported for normally distributed numerical variables. Medians and interquartile ranges are reported for nonnormally distributed numerical variables. For bereavement care activities, Likert scale categories of “never,” “rarely,” and “sometimes” were collapsed into a category labeled “no participation” in bereavement activities, while “often” or “always” were collapsed and defined as “active participation.” For questions regarding physician emotions, beliefs, and knowledge surrounding bereavement care, “important” and “very important” were defined as “positive answers.” Univariate and multivariate analysis using logistic regression was performed to model active engagement in bereavement activities. Multivariate models included all variables with p-value <0.2 for association with bereavement care. Missing data were not imputed, rather, list-wise deletion was utilized.
Results
Participant characteristics
Electronic surveys were distributed to 2,061 eligible participants. A total of 522 surveys (25.3%) were fully completed, all of whom met inclusion criteria. Twenty-two participants (1.1%) declined to complete the survey because of minimal to no patient care responsibilities or because they practice hematology only. The median age of participants was 44.6 years (±10.4 years) and they worked a median of 60 hours per week. Just over half (51%) of the respondents are female and 87% are attending level providers. The median time of practicing medicine was 14 years (1–47 years). The majority of participants (92%) work at an academic hospital or medical center, most of which have palliative care services (89%). (Table 1).
Not all participants answered this question.
Participants could answer more than one category.
More than half of the respondents (58%) indicated that greater than 10% of their patients have advanced or life-limiting illness, while 21% reported this in greater than 25% of their patients. Respondents experienced 8.5 patient deaths per year on average. A small number of respondents (2.5%) reported completion of palliative care fellowship, 12.5% had experience as a hospice or palliative care physician, while a third (34.2%) of the physicians reported no formal palliative care training. Almost 1/3 of participants (29%) did not know if a bereavement program exists at their institution.
Bereavement practices
Participants were asked how likely they are to engage in specific bereavement activities (phone calls, condolence cards, memorial service attendance, family meetings, or referrals for bereavement services) following the death of a patient. More than a third (38%) “often” or “always” engaged in at least one bereavement activity, while 44% reported that they “sometimes” participate in bereavement care, and 18% “rarely” or “never” participate.
The most common bereavement activities were calling parents (30%), attending funerals/memorial services (41%), and sending condolence cards (42%). A quarter of participants rarely or never attended memorial services and nearly half (48%) rarely or never met with a family after the death (Table 2). When questioned about workplace practices, 41% indicated that they are aware of a departmental practice intended to support bereaved families and 30% of these stated that physicians are encouraged to participate. Examples of departmental practices included bereavement information (pamphlets), reminders of death anniversaries, condolence cards, hospital remembrance events, and mementos such as flowers, wind chimes, and hand molds.
The scale used included “never,” “rarely,” “sometimes,” “often,” “always,” and not applicable. Those who respond to questions with “often” or “always” were defined as “actively” participating in that bereavement care practice.
Total N = 522 as some categories had missing observations.
Predictors that were associated in univariate analysis with initiating communication with the family after a patient's death included female gender, being an attending physician, access to institutional palliative care services, older age/seniority in practice, and parenthood. Only years in practice (which overlapped with being an attending provider), gender, and presence of a palliative care program remained significant in multivariate analysis (Tables 3 and 4).
Number of observations used in the final model was n = 464.
Number of observations used in the final model was n = 470.
Physicians with access to a palliative care program were more likely in multivariate analysis to engage in all bereavement care activities, including calling families (adjusted OR: 1.90, 95% CI: 1.52–3.14; Table 3), writing condolence cards (adjusted OR = 1.83, 95% CI: 1.21–2.79; Table 4), attending memorial services (adjusted OR = 2.57, 95% CI: 1.13–5.85), and referring family members to bereavement counselors (adjusted OR = 1.90, 95% CI: 1.14–3.16).
Physician beliefs and attitudes
Nearly all participants (96%) believed that bereavement care is part of good clinical care and only 4% of respondents felt that their responsibility ends when a patient dies. Eight percent indicated that they believe that bereavement support is the responsibility of nonphysician providers. Most participants agreed (72%) that families may feel abandoned when physicians fail to express sympathy following their child's death. Only 60% recognized that bereaved parents have more mental, physical, and psychosocial problems compared to parents of healthy children and 90% believed that bereavement care can help families deal with grief (Table 5).
Original Likert scale included “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree.” In this sudy, the categories of “strongly agree” and “agree” were collapsed to form a positive answer to these questions (yes).
The majority of participants (88% and 80%, respectively) indicated that they agree or strongly agree with the statements “I tend to get attached to my patients” and “I often think about my patients when I am not at work.” One-fifth indicated that despite appropriate medical management, they feel a sense of failure when their patient dies and worry that parents will be angry or dissatisfied if contacted. One-fifth of participants also feel anxious speaking with family members and almost half (46%) reported feeling emotionally drained from working with dying patients and their families (Table 5). Finally, 60% of respondents recognized that performing bereavement care can help establish personal closure and decrease personal emotional stress.
Barriers and physician needs
Lack of time was identified by almost 2/3 of participants as the biggest barrier to providing bereavement support. Shockingly, one-third of providers indicated that they are unfamiliar with their own institutional and/or community bereavement resources. Most physicians (88%) felt that addressing this knowledge gap would help them support families. A majority of participants indicated that bereavement-specific communication training (74%) and support from other providers (80%) would be moderately or extremely helpful. Half of all respondents would like formal training in writing condolence letters (Fig. 1).
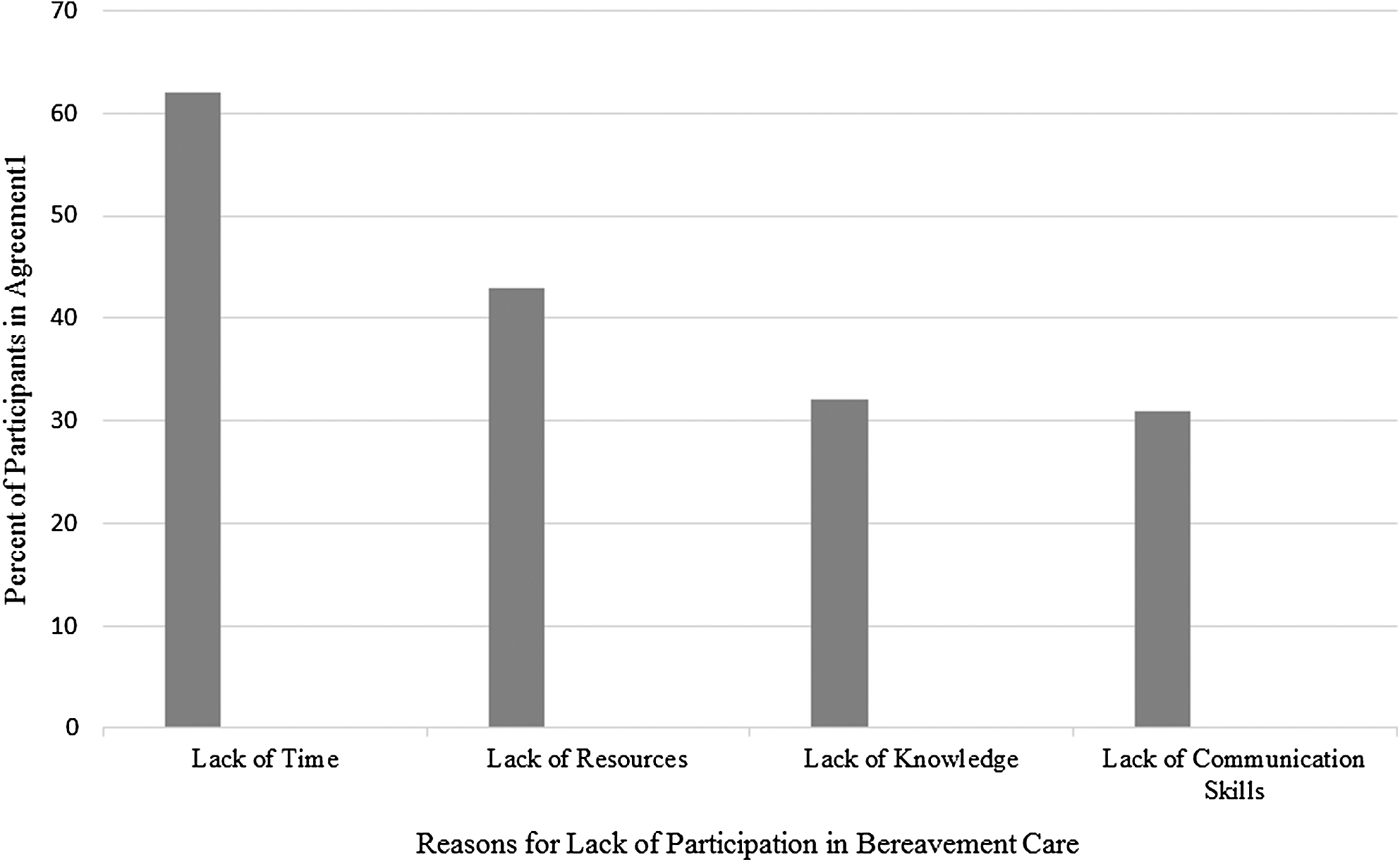
Barriers to physicians' performance of bereavement care. One percentage of physicians who answered “somewhat important,” “important,” and “very important.”
Discussion
Bereavement care is recognized as an important component of comprehensive care for families of patients with life-limiting illness.2,9,13 The American Academy of Pediatrics (AAP) advocates for integrated palliative care starting at diagnosis and continuing through bereavement support for children with life-limiting illness and their families. 26 While little data are available regarding what physician practices reduce the risk of adverse bereavement outcomes, the literature does provide convincing evidence that parents recognize and appreciate personalized physician efforts that acknowledge the life and death of their child.21,22 To our knowledge, this is one of the first studies looking at the bereavement care practices of pediatric oncologists specifically. Despite a recent position statement calling for bereavement care to be a standard practice in pediatric oncology, this is the first look at what cares are actually being provided. 19
Pediatric oncologists feel that bereavement care is important, yet are frequently unaware of institutional and community resources for bereaved families. In some settings, there are limited to no bereavement care services as these vary by location and have varied funding in many areas. This suggests that increased knowledge about existing resources in addition to more training in bereavement care provision at the local level may improve the quality of physician interventions with bereaved families.
Similar to a study conducted of physicians who care for adult cancer patients, our results indicate that the presence of a palliative care program is associated with increased physician-directed bereavement care practices.15,16 Most palliative care teams see bereavement care as part of their responsibility and continue to provide services for families after the loss of their child. Perhaps having palliative care clinicians present, who model the provision of bereavement care, allows other physicians the opportunity to see, understand, and subsequently perform similar activities for the bereaved. Palliative care teams may therefore serve as educators for clinicians about the importance of bereavement care and also offer support to clinicians by sharing their knowledge and skills.
This study indicates that pediatric oncologists are more likely than adult oncology providers to engage in active bereavement support15,16 In a similar study of medical oncologists, less than 10% of providers felt that a condolence card was their responsibility, suggesting that bereavement support may not be provided or may be delegated. 16 In contrast, almost all participating pediatric oncologists believed that physicians have a responsibility to provide bereavement support; many actually provide this and recognize that families may feel abandoned otherwise. In pediatrics, family-centered care is expected; the unique patient–family relationship inherent to pediatrics may underlie the pediatric oncologist's desire to deliver bereavement care for surviving family members. However, 40% of pediatric oncologists did not agree with the statements regarding the adverse health outcomes seen in bereaved parents, despite a great deal of literature support. Further education for physicians in training regarding the comorbidities seen in bereaved parents may motivate them to enhance bereavement care provision to decrease these risks.
Being an attending physician was associated with increased bereavement engagement, yet the majority of our sample was attending physicians (13% were fellows). However, longer practice duration among attending physicians correlated with increased engagement with specific bereavement care practices in multivariate analysis as well. This suggests that the physician experience is an important influence on bereavement practice. Physicians, despite not having formal bereavement training, may learn these skills as they experience pediatric oncology as a career.
Bereavement engagement was higher in female physicians than their male counterparts. Interestingly, concern for physician burnout is more common in female physicians, both pediatricians and oncologists, as well.27,28 As above, bereavement care is difficult for some due to the emotional toll it may take to interact with bereaved parents. In our study at least, despite the potential for increased emotional exhaustion (one element of burnout), female physicians were more likely to provide bereavement care. This gender difference is interesting, unexplained, and requires further research. We hypothesized that physicians with children of their own may better relate to and therefore provide support for parents who have lost children. Parenthood significantly influenced bereavement care provision in univariate, but not multivariate analysis.
Despite a growing recognition that bereavement care is inherent to good clinical care, physicians often receive little training on how to compassionately and professionally communicate with families after a loss.14,15,18,21,29,30 Many physicians learn about bereavement care from mentors or through a “trial and error” approach rather than through dedicated training. 18 Most pediatric oncology fellows do not receive specific education in provision of bereavement care as this is not part of the required curriculum. Pediatric trainees report being uncomfortable attending to patients and families at or around the time of death, further highlighting the need for education and modeling from more experienced practitioners. 14 Structured, educational experiences may not only improve a trainee's skill in bereavement support but also prepare young physicians to cope with the emotional demands of caring for seriously ill children. By formally integrating bereavement care training into medical education, physicians may improve the utilization of institutional and community resources and be better prepared to support families at the end of their child's life.
Not unexpectedly, the pediatric oncologists indicated that they form strong professional and emotional attachments to their patients, however, a significant portion indicate that they experience anxiety or feel emotionally drained as a result of providing end-of-life care. Interestingly, these specific emotional barriers did not predict which physicians provide bereavement care. This suggests that some providers may benefit from continuing relationships with bereaved families, while this may cause stress for others. The intensity of patient relationships and physician's personal styles may influence how they handle relationships with bereaved parents.
The most common barrier to provision of bereavement care cited by pediatric oncologists was lack of time (Fig. 1).1,15,16 Reimbursement for time spent in bereavement support is scarce, which may deter clinicians.12,18,31 Aside from the busyness of a clinician's schedule, our data suggest that a combination of emotional factors and lack of training in how to address bereaved families may prohibit physicians from bereavement care.
How do we encourage more pediatric oncologists to systemically participate in bereavement care for their patients? Physicians may benefit from a greater emphasis on self-care, including skills to identify and process their grief responses.11,17,18 In fact, writing a condolence letter or attending a funeral may be deeply appreciated by a bereaved parent and may also contribute to physician self-care. If physicians are well, they may be more able to address the difficult task of reaching out to bereaved families. The AAP recently addressed the need for organized efforts surrounding physician health and wellness as these areas are consistently overlooked due to pressing patient care and research issues. 32 Improved communication education for trainees may also help alleviate stress when caring for bereaved families by providing clear, appropriate language to use with the bereaved. Both self-care and communication interventions may also help minimize burnout, which is known to diminish compassionate care and is unfortunately common in both pediatric and oncology physicians.28–33
This study offers insight into the bereavement practices of pediatric oncologists, a subspecialty with clinically relevant perspectives regarding the care of children with life-limiting conditions. There are relevant limitations recognized by the authors. The study population of interest was difficult to define in its entirety and reach by e-mail. We targeted programs that participate in a large national organization, but smaller programs may have been overlooked.. The majority of respondents work in an academic medical center with access to a palliative care team. As pediatric oncology practices are limited, most are located in universities and larger cities, yet this may influence our results. Nonresponse bias is a limitation15,34 as only 25% of eligible participants completed the survey. The investigators acknowledge that the practices of nonresponders may vary considerably. 34 Data were self-reported, not based on observation of practice behaviors, and physicians could overestimate their participation. Furthermore, this study did not attempt to link physician practices with parental bereavement outcomes or satisfaction with care, which are both important directions for future research.
Conclusions
This study demonstrates that the majority of pediatric oncologists engage in clinical practices to support bereaved families. Most acknowledge that parents may feel abandoned after the loss of a child, yet many do not know about the adverse health risks for bereaved parents. Pediatric oncologists report that lack of time and resources are barriers to participation in bereavement care. In addition, many physicians are unfamiliar with the resources available even within their institutions and communities. Educational programs focusing on the provision of bereavement care, physician self-care, and communication skills should be explored to improve pediatric oncologists' bereavement care practices.
Footnotes
Acknowledgments
This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding, in part, from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant 8UL1TR000105 (formerly UL1RR025764).
Study data were collected and managed using REDCap electronic data capture tools hosted at The University of Utah. REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data download to common statistical packages; and (4) procedures for importing data from external sources. The authors would also like to acknowledge support from Dr. Krzyzanowska who kindly shared her survey instrument used to assess bereavement care in the adult oncology physician population.
Author Disclosure Statement
No competing financial interests exist.