
Abstract
Dear Editor:
The goal of advance care planning (ACP) is for patients to communicate their end-of-life (EoL) treatment preferences to a selected proxy. However, it is not clear what information must be shared to adequately inform a proxy. Given the practical challenges of measuring ACP conversations, previous studies have focused on measuring ACP surrogates such as code status documentation or completion of advance directives (ADs) and/or physician orders for life-sustaining treatment (POLSTs).1,2 However, it has been demonstrated that AD completion alone does not necessarily promote high-quality EoL communication or understanding between patients and proxies. 3
The aim of this pilot study was to determine the feasibility of completing a focused ACP conversation identifying an informed proxy in a single clinic visit. This study was completed in adult cancer patients with a prognosis of less than one year. A clinical social worker led the ACP intervention between study patients and proxies focusing on three EoL preferences: (1) the patient's personal definition of quality of life, (2) his or her specific plan if he or she cannot achieve this quality of life, and (3) desired location of death. The proxy was deemed “informed” if he or she understood these three EoL preferences. Patients were encouraged but not required to complete an AD/POLST and followed until death.
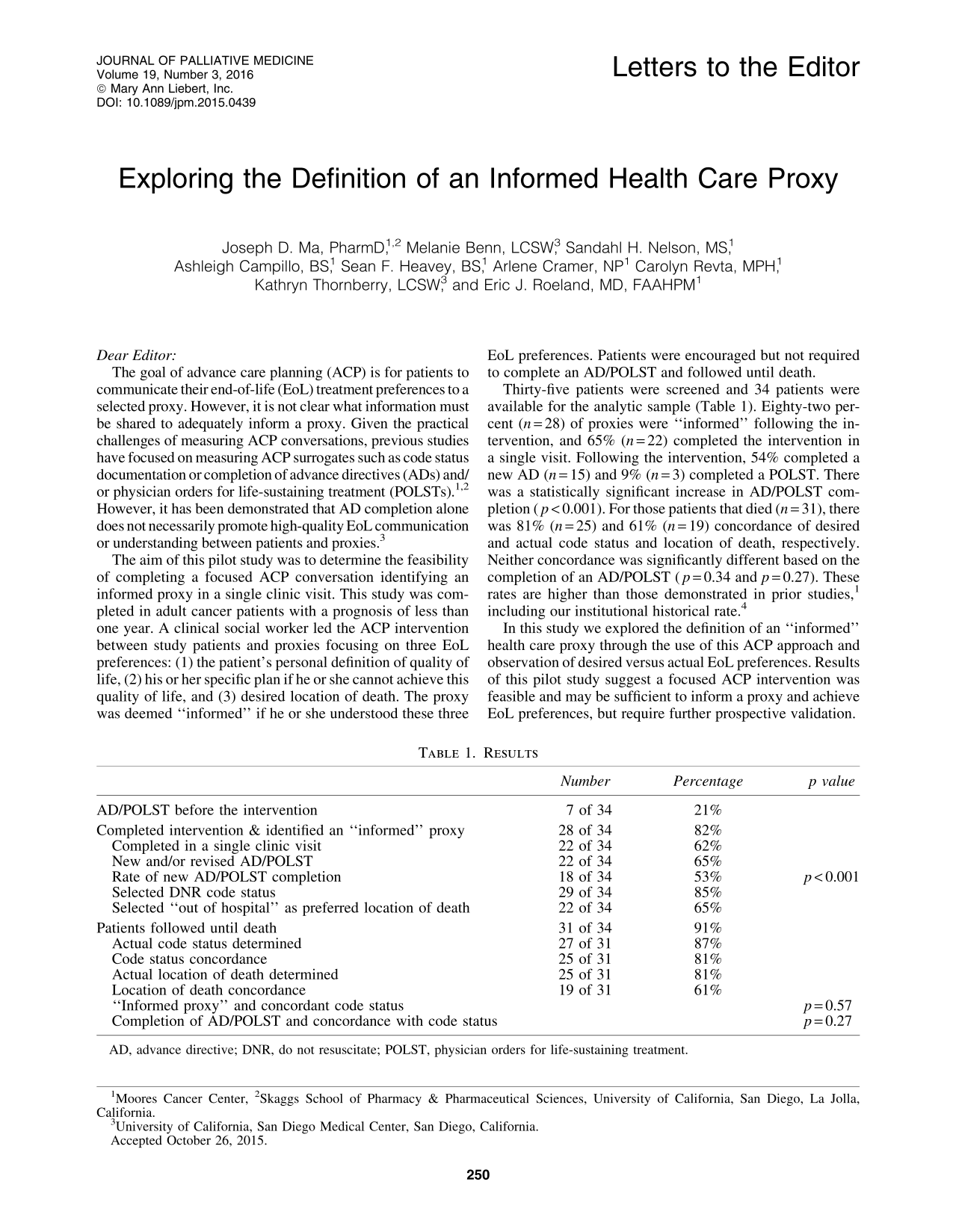
Thirty-five patients were screened and 34 patients were available for the analytic sample (Table 1). Eighty-two percent (n = 28) of proxies were “informed” following the intervention, and 65% (n = 22) completed the intervention in a single visit. Following the intervention, 54% completed a new AD (n = 15) and 9% (n = 3) completed a POLST. There was a statistically significant increase in AD/POLST completion (p < 0.001). For those patients that died (n = 31), there was 81% (n = 25) and 61% (n = 19) concordance of desired and actual code status and location of death, respectively. Neither concordance was significantly different based on the completion of an AD/POLST (p = 0.34 and p = 0.27). These rates are higher than those demonstrated in prior studies, 1 including our institutional historical rate. 4
AD, advance directive; DNR, do not resuscitate; POLST, physician orders for life-sustaining treatment.
In this study we explored the definition of an “informed” health care proxy through the use of this ACP approach and observation of desired versus actual EoL preferences. Results of this pilot study suggest a focused ACP intervention was feasible and may be sufficient to inform a proxy and achieve EoL preferences, but require further prospective validation.
Footnotes
Acknowledgments
This study was supported in part by the American Cancer Society Institutional Research Grant 70-002 provided through the University of California San Diego Moores Cancer Center.