
Abstract

Introduction
C
Although more than 90% of cancer-induced hypercalcemias respond to initial treatment with rehydration and use of bisphosphonates, the condition often recurs after one to four weeks after the initial treatment and becomes difficult to control.7,8
Although hypercalcemia treatment does not always alleviate distress in terminally ill cancer patients and could in fact make them more distressed, there is no consensus on whether or when treatment should be withdrawn or withheld. 9
As previously shown in the issues of end-of-life discussion, hydration, and sedation in terminally ill patients, physicians' attitudes vary considerably between specialties.10–13 Our previous study reported that physicians' specialties, beliefs on treatment efficacy, and perceived importance for a good death affected their attitude on whether hypercalcemia should be treated until patients' death. 14
It is important that medically appropriate treatment could be offered consistently by all physicians beyond the difference in specialty-specific attitudes among the physicians. The primary aim of this study was to clarify interspecialty differences in physicians' treatment attitudes, beliefs on the efficacy of hypercalcemia treatment, and reasons for withdrawing or withholding hypercalcemia treatment in terminally ill cancer patients.
Methods
This study was designed as a nationwide cross-sectional survey, in which a self-reported questionnaire was mailed to eligible physicians in 2004. Potential participants were recruited from the member list of the Japanese Society for Palliative Medicine (JSPM). JSPM is a multidisciplinary association consisting of palliative medicine specialists, oncologists, internists, and surgeons with interest in palliative care. A total of 757 physicians, whose specialty involved treating hypercalcemia in daily practice (i.e., internal medicine, surgery, oncology, and palliative medicine), were requested to complete and return the questionnaire. Physicians whose specialties rarely involved treating hypercalcemia (such as emergency medicine, psychiatry, pathology, and public health) were excluded. Scientific and ethical validity were approved by the Institutional Review Board of Tohoku University.
Questionnaire
Due to lack of validated instruments, we developed the questionnaire through discussions with reference to our previous studies.11–12 Face validity was confirmed in a pilot test.
Physicians' attitudes, beliefs, and reasons for withdrawing or withholding hypercalcemia treatment in terminally ill cancer patients were assessed by asking them to rate their degree of agreement with 2 statements on attitude (e.g., How much do you think that hypercalcemia treatment should be provided for a terminally ill cancer patient with cancer-induced hypercalcemia in general/until the patient's death?), 12 statements on belief (e.g., “hypercalcemia treatment improves nausea” and “effect of treatment reduces gradually”), and 17 reasons for withdrawing or withholding treatment (e.g., “intractable pain” and “family member's preference”) on a six-point Likert-type scale (1: strongly disagree to 6: strongly agree). Physicians who (dis)agreed with each statement were defined as those who chose “slightly (dis)agree,” “(dis)agree,” or “strongly (dis)agree.” Physician characteristics such as sex, years of clinical practice, experience of anticancer treatment, specialty, and practice settings were also obtained.
Statistical analyses
The characteristics of the respondents are expressed as mean standard deviation (SD) or % (n), where applicable. The percentage of physicians who agreed with hypercalcemia treatment in terminally ill cancer patients, in general, or until a patient's death was plotted using a bar plot according to the physicians' specialties and compared by using chi-square test.
To explore interspecialty differences in physicians' beliefs and reasons for withdrawing or withholding hypercalcemia treatment, we summarized the mean values with SD on the six-point belief scales. Interspecialty difference was tested using an analysis of variance with post hoc tests. Thresholds for statistical significance were restricted to p < 0.004 (i.e., 0.05/12) for the beliefs and p < 0.003 (i.e., 0.05/17) for the reasons with Bonferroni correction. Post hoc analysis was conducted using Scheffe's test.
For analyses, the specialties were grouped into four categories: palliative medicine (palliative care, home hospice practice, or pain medicine), surgery (general surgery, thoracic surgery, urology, gynecology, orthopedics or otorhinolaryngology), internal medicine (general internal medicine, gastroenterology, respiratory medicine, dermatology, or neurology), and oncology (medical oncology, radiation oncology, hematology, and breast medicine).
All analyses were performed using the Statistical Package for the Social Sciences version 18.
Results
Analyzable responses were returned from 380 physicians (response rate: 50.2%). The characteristics of the respondents are summarized in Table 1.
Values are mean (SD), or % (n).
The percentage does not add up to 100% due to missing data.
Attitudes toward treatment for hypercalcemia in terminally ill cancer patients
As shown in Figure 1, more than 80% of physicians agreed to treat hypercalcemia in general. The difference between specialties was not significant. In contrast, the percentage of respondents who agreed to treat hypercalcemia until a patient's death was the lowest in palliative medicine (30%), followed by internal medicine (43%), surgery (53%), and oncology (54%; p = 0.001).
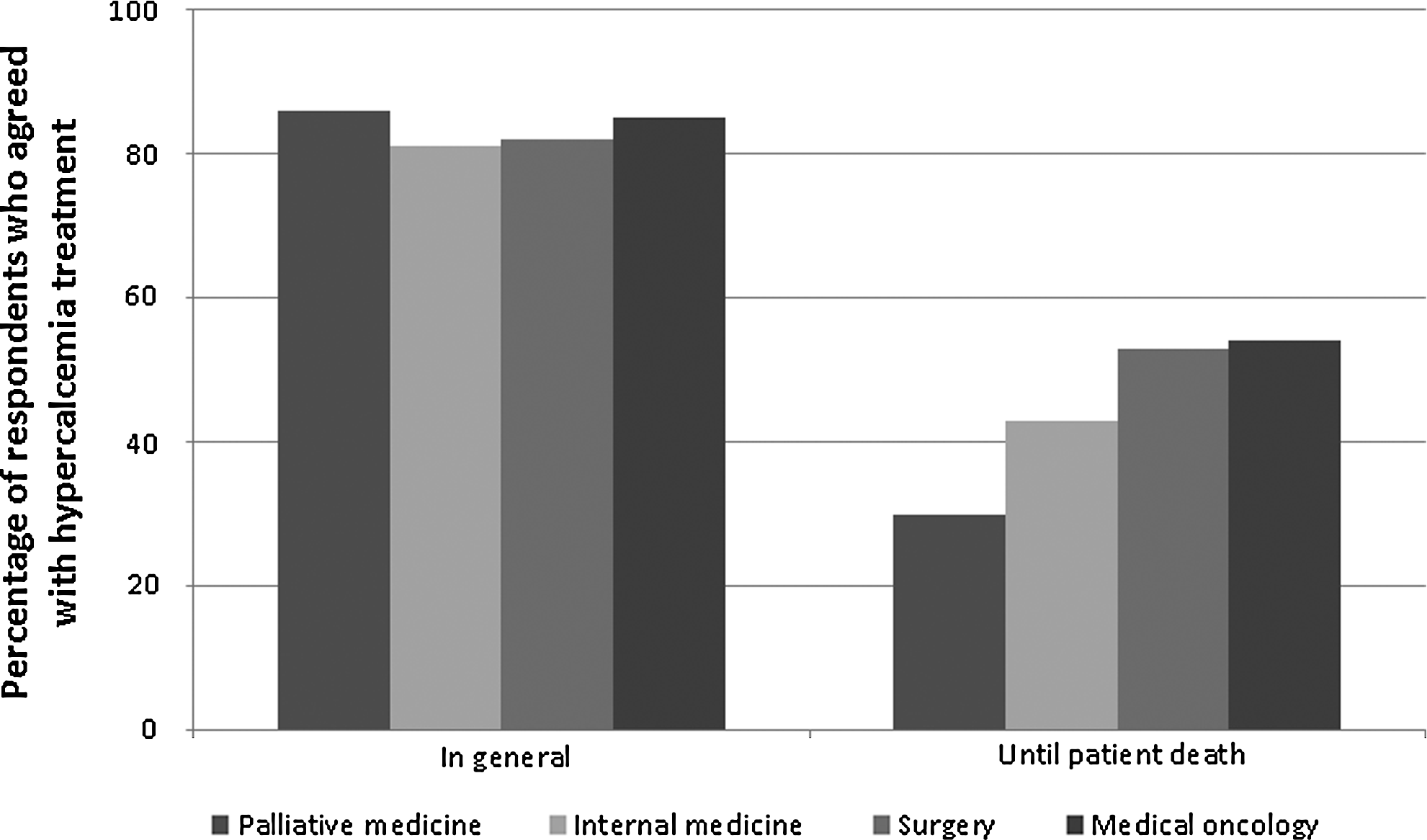
Percentage of physicians who agreed with hypercalcemia treatment in terminally ill cancer patients in general (left) or until patient death (right). Physicians were asked “How much do you think that hypercalcemia treatment should be provided for a terminally ill cancer patient with cancer-induced hypercalcemia in general/until the patient's death?” and classified as “agree” if they answered “4: slightly agree,” “5: agree,” or “6: absolutely agree.” Interspecialty difference in physicians' attitude toward hypercalcemia treatment in general was not significant (p = 0.77), but was significant for “until the patient's death” (p = 0.001).
Physicians' specialty and belief on hypercalcemia treatment
As shown in Table 2, more than 80% of the physicians believed that hypercalcemia treatment improves nausea, consciousness disturbance, delirium, bone pain, and quality of life; that the effect of the treatment is unpredictable; and that bisphosphonate is expensive. Only one-third of the physicians believed that hypercalcemia treatment prolongs patient survival. The proportion of physicians who believe that death in hypercalcemia is less distressing was 51%. Palliative medicine specialists had a significantly stronger belief that hypercalcemia treatment improves consciousness disturbance (vs. surgeon, p = 0.002), effect of hypercalcemia treatment reduces gradually (vs. oncologists, p = 0.005), death in hypercalcemia is less distressing (vs. surgeon, p = 0.028; and vs. oncologists, p = 0.001), and bisphosphonate is expensive (vs. oncologists, p < 0.001).
On a 6-point Likert-type scale from 1: strongly disagree to 6: strongly agree.
classified if the physician answered “4: slightly agree”, “5: agree”, or “6: strongly agree”.
p-values for ANOVA. Threshold of statistical significance was restricted to p < 0.004 (i.e., 0.05/12) with Bonferroni correction.
significantly different when compared with palliative care.
Physicians' specialty and reasons for withdrawing or withholding hypercalcemia treatment
As shown in Table 3, a prognosis of less than one week, worsened patient distress after previous hypercalcemia treatment, and patient's preference were the reasons for withdrawing or withholding treatment in most physicians. A prognosis of a few months or longer, patient being of older age, intractable bone pain, and price of bisphosphonate were rarely reasons for withdrawing or withholding hypercalcemia treatment. Internists more strongly agreed to withdraw or withhold hypercalcemia treatment if the patients had intractable bone pain compared with other specialties (vs. palliative medicine specialists, p = 0.002; vs. surgeons, p = 0.036; medical oncologists, p = 0.026). Palliative medicine specialists more strongly thought treatment should be withdrawn if the patient's distress worsened after the previous treatment compared with surgeons (p < 0.001) and medical oncologists (p < 0.001), medical oncologists were less likely to consider withdrawing or withholding treatment if family members do not wish for further treatments (vs. palliative medicine specialists, p = 0.004; vs. internal medicine physicians, p = 0.001).
On a 6-point Likert-type scale from 1: strongly disagree to 6: strongly agree.
classified if the physician answered “4: slightly agree,” “5: agree,” or “6: strongly agree.”
p-values for ANOVA. Threshold of statistical significance was restricted to p < 0.003 (i.e., 0.05/17) with Bonferroni correction.
significantly different when compared with palliative care. ¶: significantly different when compared with internal medicine.
Discussions
We demonstrated interspecialty differences in physicians' attitudes, beliefs, and reasons for withdrawing or withholding hypercalcemia treatment in terminally ill cancer patients. We found that palliative care physicians (1) were more likely to withdraw or withhold hypercalcemia treatment before patient death; (2) believed more strongly that treatment efficacy decreased gradually, and death in hypercalcemia was less distressing; and (3) thought that worsened patient distress after previous treatment and family member's preference was important when determining treatment policy.
Recurrent hypercalcemia is a refractory symptom and its treatment does not necessarily reduce patient's distress, that is, coma caused by hypercalcemia may contribute to alleviation for patient's discomfort. 9 Because efficacy of hypercalcemia treatment decreases gradually,15–17 practical and ethical dilemmas arise on whether and when hypercalcemia treatment will be terminated. As shown in our previous report, 57% of physicians engaging oncology and palliative care practice disagreed on treating hypercalcemia until a patient's death. 14 In this study, findings illustrated that palliative care physicians make treatment decisions with significant consideration of patients' comfort, families' preference, and the course of the previous treatment. Their attitude may be influenced by their clinical experience and the central aim of palliative care, which is alleviating distress in dying patients and their families.
Several limitations of the study should be noted. First, this survey was conducted in 2004. The results may not be the same if a follow-up survey is conducted recently because some clinical guidelines and a new class of drug (denosumab) are now available. Second, the generalizability of the results might be restricted because this survey was conducted on JSPM member physicians predominantly consisted of Japanese male physicians with a relatively low response rate. We believe, however, that interspecialty differences were larger if the survey included non-JSPM member physicians because oncologists would more aggressively treat hypercalcemia in terminally ill patients. Other limitations were use of a nonvalidated questionnaire with vague definitions of disease stage “in general” and “until death.”
In conclusion, we found interspecialty differences in physicians' attitude, beliefs, and reasons for withdrawing or withholding hypercalcemia treatment for terminally ill cancer patients.
These differences may partly be attributed to the differences of patients' disease stage and physicians' usual practice. More patient outcome data are needed to identify terminally ill patients with cancer-induced hypercalcemia who are benefited from hypercalcemia treatment to provide them with standardized care beyond the difference in physician' attitude by specialty.
Footnotes
Acknowledgments
We thank Michiya Ito, Toshimichi Nakaho, Kumiko Suzuki, and Akiko Sukeno for their useful comments regarding this study.
Author Disclosure Statement
No competing financial interests exist.