
Abstract
Abstract
Background:
Compared with private, not-for-profit hospitals, significantly fewer public hospitals report that they provide palliative care services for their patients. Because uninsured and underinsured patients largely depend on public hospitals for acute medical care, they therefore experience disparities in access to inpatient palliative care services. To address this disparity, the statewide Spreading Palliative Care in Public Hospitals Initiative (SPCPHI) was established to help implement or expand inpatient palliative care services in all 17 of California's public acute care hospitals.
Aim:
The aim of this article is to use the experiences from the SPCPHI to describe the unique challenges to providing palliative care in public hospitals; the major barriers to initiating, growing, and sustaining palliative care programs in public hospitals; and the common solutions to overcoming those barriers.
Conclusions:
Palliative care programs in public hospitals must develop the necessary skills and staffing to meet the complex needs of vulnerable patients and their families. These programs face a variety of unique organizational and operational challenges such as limited and uncertain funding, limited access to hospital data and analytic support, and complex regulatory structures, which may hinder growth of palliative care in these systems. Experiences from the SPCPHI suggest that networking, technical assistance, and startup funding are helpful to overcome these barriers and to develop high-quality, sustainable palliative care programs in public hospitals.
Introduction
D
Hospitals that care for patients regardless of their ability to pay are variably referred to as “public hospitals,” “safety net hospitals,” or “essential hospitals.” These institutions typically care for a significant proportion of patients insured by Medicaid, those who have limited health insurance, or those who are uninsured. Of the ∼250 “essential” hospitals in the United States, many also serve as academic training sites and provide critical emergency services such as Level I Trauma services, pediatric or neonatal intensive care, and specialized burn care. 5 Public hospitals are typically owned and operated by state or local government, whereas other “safety net” or “essential” hospitals may have more typical nonprofit organization and ownership.
To date, there have been no published studies addressing the disparity in palliative care program development between public and private not-for-profit hospitals. The purpose of this article is to share lessons learned from developing palliative care programs in public hospitals, through a statewide initiative in California, the Spreading Palliative Care in Public Hospitals Initiative (SPCPHI), which has been previously described. 6 For the purposes of this article, we refer to public, safety net, and essential hospitals as “public hospitals,” though it should be noted that some of the hospitals included in this initiative are neither owned nor operated by the government. This 5-year initiative funded by the California HealthCare Foundation (CHCF) sought to develop or expand palliative care programs in all 17 of California's acute care public hospitals. The experiences of these 17 hospitals provide insight about how to care for the specific populations of patients cared for in public hospitals, the challenges to developing palliative care programs in public hospitals, and the strategies to overcome these challenges. Because many hospitals work with underserved and marginalized populations and face challenges similar to public hospitals, though often to a lesser degree, many of these lessons are also relevant to other hospitals and palliative care programs serving marginalized populations.
Description of the SPCPHI
The SPCPHI was a collaboration between the CHCF; the California Association of Public Hospitals and Health System–Safety Net Institute; the University of California, San Francisco Palliative Care Leadership Center (PCLC); and Learning Partners. It provided funding, technical assistance, and direct advocacy to palliative care champions at each of California's acute care public hospitals. Figure 1 shows the distribution of grantee hospitals across California, and Table 1 describes the characteristics of the 17 sites. Twelve sites received implementation or expansion grants in 2009, and 5 additional sites received funding in 2011.
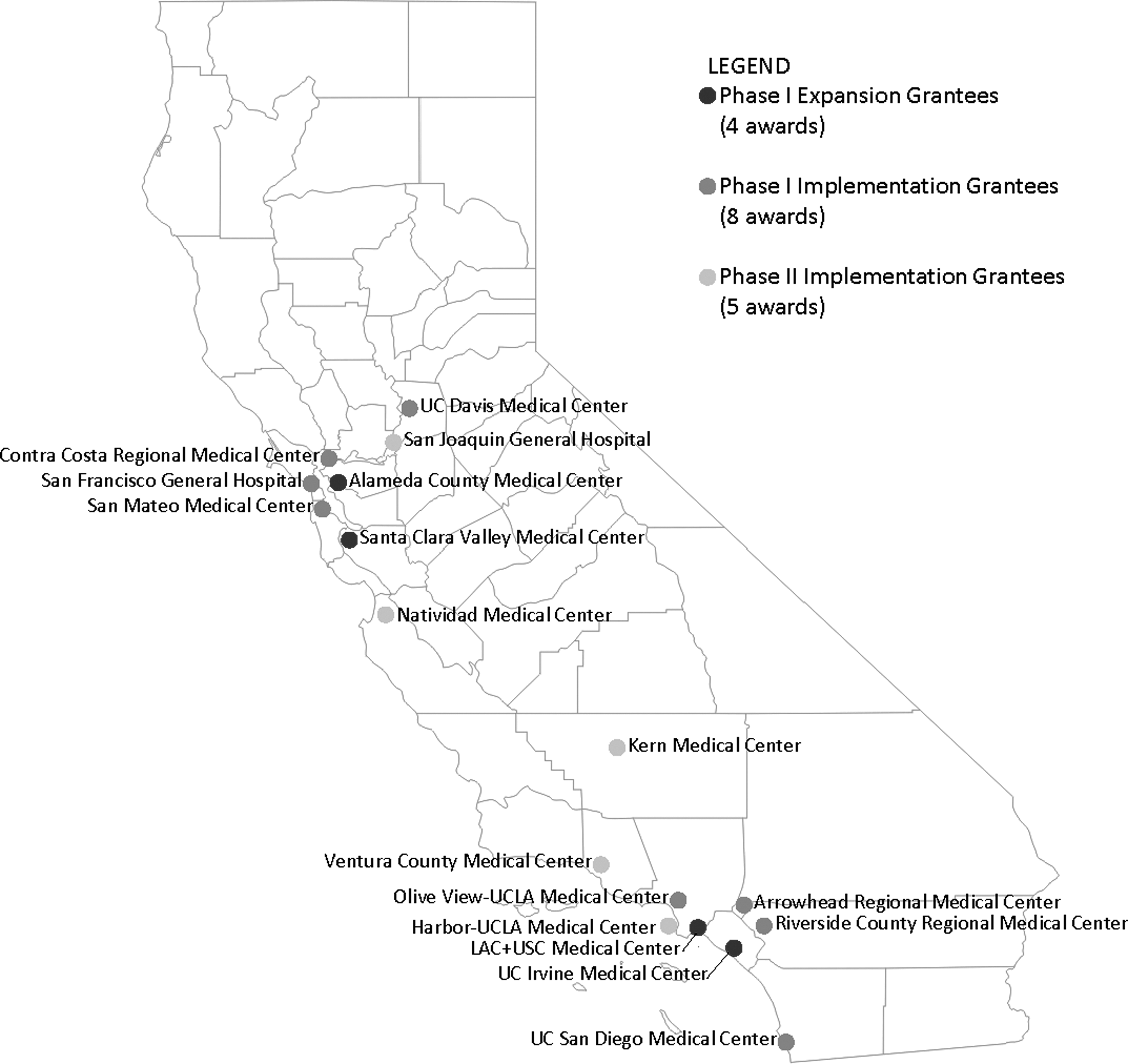
Map of Spreading Palliative Care in Public Hospitals Initiative (SPCPHI) grantee sites.
Data for overall bed size, academic affiliation, and trauma status obtained from the Office of Statewide Health Planning and Development. Available online at gis.oshpd.ca.gov/atlas/places/list-of-hospitals
Number of consults during the reporting period for each site. SPCPHI sites reported data for variable lengths of time, as noted in footnotes c–f.
12 implementation and expansion sites reported data from January 2010 to June 2013.
Harbor–UCLA Medical Center and Kern Medical Center reported data from July 2012 to June 2013.
Natividad Medical Center reported data from January 2012 to June 2013.
San Joaquin Medical Center and Ventura County Medical Center reported data from July 2011 to June 2013.
Grantee sites were required to provide semi-annual reports, including operational program data and narrative progress reports. Operational data included aggregated consultation metrics (patient demographics, consultation volume, and outcomes), program staffing, and educational activities provided for hospital staff and trainees. Narrative progress reports included descriptions of project accomplishments, impact, challenges, and sustainability plans. In 2014, 16 months after completion of the Initiative, follow-up phone interviews were conducted with the palliative care leaders of all 17 programs to ascertain changes in consult volume and staffing, and to elicit factors contributing to or threatening program sustainability.
We used operational data to describe the characteristics of patients served and staffing of palliative care teams in the SPCPHI. Narrative data obtained before 2011 reflect the experiences of the original 12 grantee sites, whereas operational data after 2011 and follow-up phone interviews reflect the experiences of all 17 sites. Two authors (ALK and HAH) independently reviewed the final project narratives and 16-month follow-up phone interview transcripts, cataloguing themes. These themes were then reviewed by two additional authors (PC and RTB) in comparison with the narratives, and an overall consensus was reached among all authors regarding prominent and consistent themes. The themes are listed as major subject headings throughout the remainder of this article.
Differences in Providing Palliative Care in Public Hospitals
Patients served
As of the final reporting period in 2013, the 17 palliative care programs had provided care to 15,499 unique patients through 17,337 consults. Patients seen by SPCPHI teams were relatively young, with a mean age of 59 years and a median age of 58 years across all sites in 2010. Given that 26% of the patients seen by all of the programs died during hospitalization, and an additional 27% were discharged with hospice care, this statistic stands in stark contrast to the average life expectancy in California (80.4 years) and to the average age of 71.6 years for patients seen by member sites of the Palliative Care Quality Network (PCQN), a nationwide quality improvement collaborative.7,8
Racial demographics of patients seen at 12 of the SPCPHI sites in 2010 are shown in Figure 2. Beyond their racial diversity, patients seen by the SPCPHI consult services also included a large population of immigrants, many of whom had limited English proficiency. In the final 12 months of data collection (July 2012–June 2013), SPCPHI sites reported that 36% of patients used a primary language other than English, with at least 17% requiring professional interpreters for substantive conversations. By contrast, data from the U.S. Census's 2013 American Community Survey suggest that only 19% of Californians and 8.5% of all Americans report limited English proficiency. 9
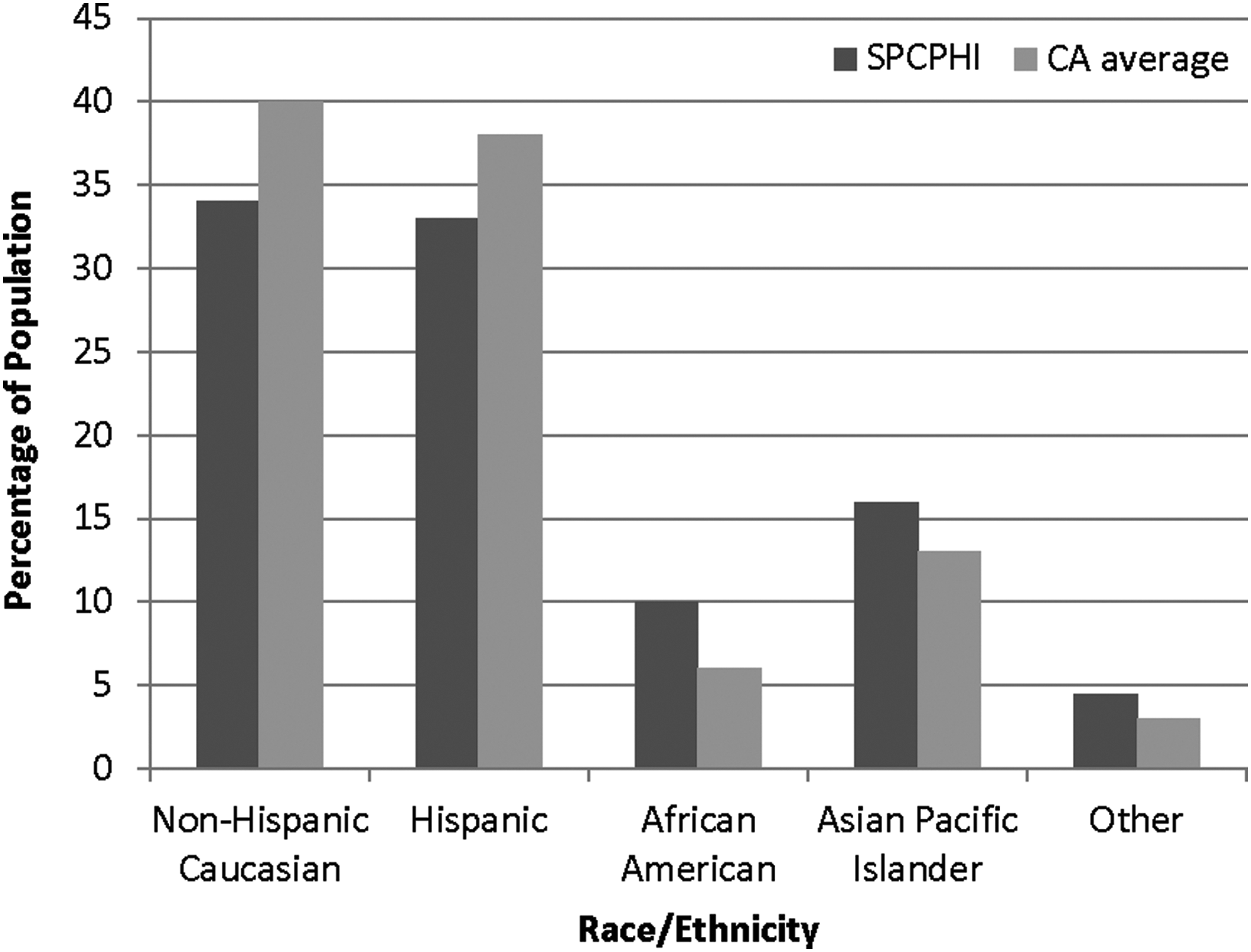
Cumulative racial demographics of patients seen by SPCPHI sites in 2010, compared with 2010 California racial demographics (http://www.dof.ca.gov/research/demographic/reports/projections/p-1/). SPCPHI, Spreading Palliative Care in Public Hospitals Initiative.
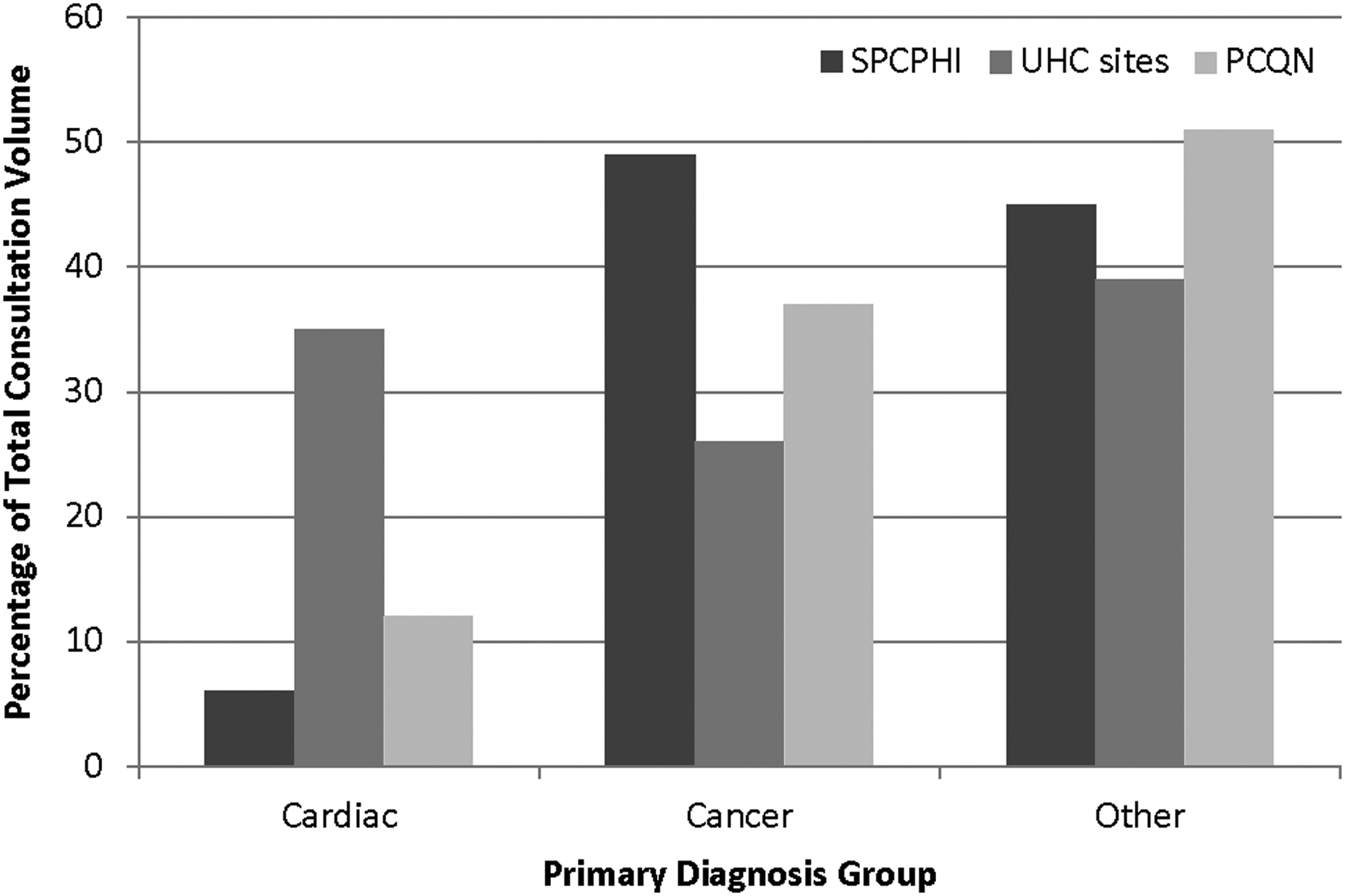
SPCPHI sites cared for a larger proportion of cancer patients than other palliative care programs have reported elsewhere (Fig. 3). Nearly half of all patients seen by SPCPHI in FY13 had a principal diagnosis of cancer, only 6% had a principle cardiac diagnosis, and 13% had a principal neurologic diagnosis; a large minority (32%) had “other” principal diagnoses. By contrast, a 2007 analysis of inpatient palliative care programs at 35 University Health Consortium sites showed that 35% of patients had a principal diagnosis of heart failure, 26% had a principal diagnosis of cancer, and the remaining 39% had a principal diagnoses of HIV or respiratory illnesses. 10 Similarly, data from the PCQN show that among nearly 20,000 patients cared for by 28 palliative care teams, 37% have cancer as the principal diagnosis, 12% have cardiovascular disease, and 10% have neurological disease. 8
In addition to demographic data collected by the 17 SPCPHI sites, narrative reports from the sites describe a variety of psychosocial challenges faced by their patients. Several sites described challenges associated with caring for patients with limited financial resources, particularly when making arrangements for necessary healthcare and support services in the community. Three sites described targeted outreach to partner hospice agencies to arrange for charity care for their patients, and two sites described additional challenges in arranging for follow-up medical care after discharge. A significant proportion of patients seen at the SPCPHI sites also have difficulty in identifying friends or family who can assist with caregiving and/or surrogate decision making. In 2010, 58% of SPCPHI sites reported that more than 10% of their patients did not have a family member, close friend, or other surrogate who could assist with decision making. Some sites also reported caring for a significant proportion of incarcerated patients, whereas others described caring for patients with significant mental health comorbidities.
Palliative care team composition
SPCPHI sites reported significant racial and linguistic diversity among palliative care team members. In 2010 site surveys, 73% of palliative care teams included at least one member who identified as Hispanic, and 73% had at least one team member who identified as East Asian. By contrast, in 2004, the Sullivan Commission on Diversity in the Healthcare Workforce reported that only 9% of nurses and 6% of physicians identify as African American, Hispanic American, or American Indian. 11 In addition to racial diversity, 83% of sites reported having at least one fluent Spanish speaker on their team, and 42% reported having at least one fluent Mandarin speaker.
The professional composition of palliative care teams varied significantly across the 17 SPCPHI sites (Fig. 4). At the end of the initiative, nearly all sites (88%) reported including a dedicated physician, most included a social worker (76%), and many sites (64%) also included an advanced practice nurse and other nursing staff. A majority (58%) also included dedicated chaplain staff, whereas only 29% reported any dedicated clerical staff. In many instances, staff allocation to the palliative care team was part-time, representing less than 50% of the staff member's effort. The average total full-time equivalent (FTE) staff dedicated to the SPCPHI palliative care teams was 2.94, with an average 0.95 physician FTE, 0.5 Advance Practice Nurse FTE, 0.46 other Nurse FTE, 0.46 social work FTE, and 0.22 chaplain FTE. Although some public hospitals have encountered difficulty in obtaining funding from their local government to hire chaplains, 12 SPCPHI sites reported having chaplains assigned to their palliative care teams with the same frequency as other hospitals in California. 13
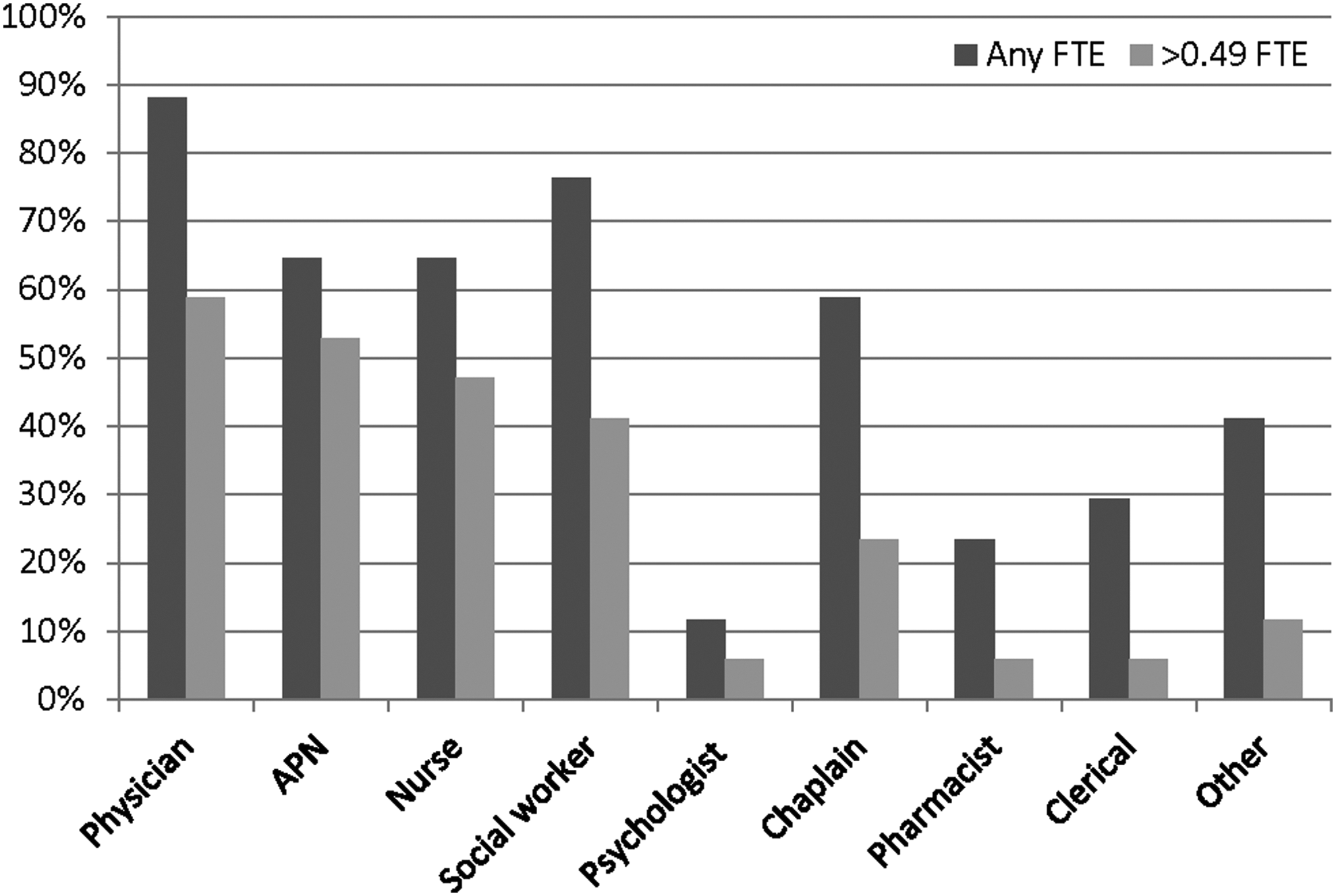
Proportion of SPCPHI sites reporting dedicated staff from various health professions, June 2013. APN, advance practice nurse; FTE, full-time equivalent, as a proportion of staff effort dedicated to work with the palliative care team.
Barriers to Development, Growth, and Sustainability for Palliative Care Programs in Public Hospitals
Experience from the SPCHPHI suggests that public hospitals often face similar challenges to those experienced by similarly sized not-for-profit hospitals, such as funding and workload. In addition, the organization, governance, and financing of public hospitals may create unique barriers to palliative care program development in these settings.
High demand for service
Nationwide, many palliative care programs report difficulty both in meeting the demand for services and in obtaining the necessary staff to meet that demand. 14 These sentiments were echoed in the SPCPHI. Interviews and narratives from the early phases of program implementation found that 83% of surveyed sites identified either “inadequate budget to pay for additional staff” or “too much demand, not enough staff on the palliative care team” as their most significant challenges toward accomplishing their program's goals. By contrast, the majority of the original 12 grantee sites reported no difficulty in recruiting staff to the palliative care team (n = 8, 67%) or in receiving referrals (n = 9, 75%). Three sites also described challenges related to working with clinicians and administrators who have a poor understanding of what palliative care is, or how it benefits patients, staff, or the hospital.
Public hospital governance and regulation
Beyond these more common challenges, palliative care programs in public hospitals must navigate a number of unique challenges related to the structure and financing of public hospitals. The majority of public hospitals in the United States are owned by the local or state government. 15 As a result, hospital governance often includes additional oversight by local and/or state government authorities. Public hospital organization and governance structures vary significantly, 16 so palliative care program leaders must learn how to navigate the unique processes of program approval and funding at their institutions. The majority of SPCPHI sites (n = 10, 83%) reported that “lack of support from hospital administration” was either “not a challenge” or a “mild challenge.” However, because program funding decisions are often made above the level of hospital administration, even the most successful public hospital palliative care programs still need approval and support at the level of city or county administration, which may be unfamiliar with the benefits of their systems' palliative care programs. One program summed up this organizational challenge, “Hospital admin [is] very supportive but ultimately they don't make the funding decisions, unfortunately.”
Beyond the difficulties of understanding and successfully navigating the complex governance structures of public hospitals, additional regulatory constraints may also present barriers to palliative care program development. For example, one site was unable to fully implement their expansion project as originally intended due to strict limitations regarding a case manager's scope of practice. Another site described difficulty in obtaining permission for social workers and chaplains to attend continuing education conferences, due to inflexible restrictions on professional development time.
Public hospital funding
Public hospital palliative care programs may face additional barriers to obtaining the necessary funding for program development and sustainability. Public hospitals care for a disproportionate percentage of Medicaid and uninsured patients, leaving significant gaps in reimbursement for services provided. During times of economic stress, as the number of uninsured Americans increases, public hospitals often experience a greater demand for services from uninsured or underinsured patients. 11 Although the Affordable Care Act has increased the number of Americans with health insurance, there are still a large number of people without any insurance, and a large proportion of Medicaid-insured patients who continue to receive care at public hospitals. As a result, public hospitals report significantly lower operating margins, compared with the national average (−0.4% vs. 6.5%). 17 In times of additional budget stress, public hospitals typically attempt to increase efficiency rather than limiting services; 13 however, new initiatives may not receive funding, and other essential components of program development (e.g., staff education, administrative support) may be cut back or eliminated.
To alleviate service stress due to slow budget approval processes or limited funds for dedicated staffing, many SPCPHI sites relied on additional mechanisms for program funding. Internally, the majority of original 12 grantee sites (75%) reported relying on “in-kind” hospital support, that is, temporary, not contracted, reallocation of existing staff resources. Although these arrangements help to meet rapidly increasing clinical demands, they are even more vulnerable in times of financial or regulatory stress. As an indication of this vulnerability, nearly all sites that participated in the entire 4-year grant period (92%, n = 11) reported at least a temporary loss of program staffing during the Initiative, which was coincident with a period of significant economic recession in the United States. Data from the SPCPHI suggest that some staff positions may be more vulnerable than others. One site commented, “All non-MD, non-RN positions in the division are in-kind supported which makes them unstable.” Three SPCPHI sites echoed difficulty in obtaining dedicated funding for social worker positions, despite the significant psychosocial challenges faced by many patients in public hospitals.
Program administration and data management
Although most sites reported dedicated physician or nursing staff for their programs, few of the original grantee sites (17%, n = 2) reported any dedicated clerical or administrative support for routine program operations in the first year of the SPCPHI. Staff who act as clinical leads often also take on primary responsibility for data collection, uploading or extraction from medical records, and/or analysis. Some sites reported partial support from quality management or hospital administration for routine data analysis; others had limited or no support for data collection and analysis. In surveys at the beginning of the Initiative, the majority of sites (75%, n = 9) reported moderate or significant difficulty in collecting and analyzing data. By the end of year 1, fewer sites (50%, n = 6) reported moderate to significant difficulty in collecting data, suggesting that sites were either able to develop their own internal processes for data analysis and collection or able to obtain support for these tasks.
Analyzing the financial impact of the palliative care programs represented its own particular challenge for the SPCPHI sites. Given that a large proportion of patients in public hospitals are uninsured or Medicaid insured, public hospitals must adapt traditional analyses to demonstrate the financial impact of their palliative care services. However, with limited analytic support and limited staffing of hospital financial departments, the necessary data can be difficult to obtain. Unfortunately, most of the original grantee sites (75%, n = 9) reported that their hospital administration had communicated goals or expectations for the palliative care program regarding financial outcomes; however, the mismatch between analytic support and expectations may make it harder to meet administrators' expectations.
Staff turnover
Turnover of key staff or influential champions is challenging for any new initiative. In follow-up postinitiative phone calls, most (58%, n = 10) SPCPHI sites noted setbacks and challenges that came with staff leaving the palliative care team or turnover in hospital administration. In particular, the loss of a physician champion or social worker seemed to impede palliative care program growth. Two sites speculated that the significant psychosocial issues impacting many of the patients served within public hospitals may have the potential to exacerbate staff burnout. At the beginning of the initiative, it was also postulated that the salaries provided to healthcare providers within public health systems, which often are less than what counterparts receive in other systems, might hamper their ability to recruit or replace team members. However, the results of the follow-up surveys suggest that the sites did not face difficulties in recruiting staff members.
Although staff recruitment was not difficult, six sites reported that the complex hiring processes in public hospitals contributed to significant delays in filling vacant positions. Narrative reports described human resource policies that require positions to be vacated and routinely reassessed for necessity before rehiring. These complex hiring processes led to added vulnerability for team positions, gaps of several months in which positions were unfilled, and an inability to formally train new hires with outgoing team members.
Strategies for Overcoming Barriers
Although SPCPHI sites identified many barriers to program growth and sustainability, they also developed many strategies to maintain and grow their palliative care programs.
Involve specific stakeholders
Many SPCPHI sites recognized the importance of commitment from the organization and the palliative care team, to establish their programs. Nearly all of the original 12 sites (92%, n = 11) identified support from hospital administration and the “quality and commitment of the palliative care team staff” as the most important factors in achieving their program's goals. Sites were encouraged to bring hospital administrators to initial PCLC trainings, which helped solidify relationships between palliative care teams and their hospital leaders.
Within the teams themselves, most of the original 12 sites (92%, n = 11) felt it was important to have a physician champion to lead program development and implementation, with interdisciplinary support from social workers, nurses, and chaplains to address the complex psychosocial issues that many vulnerable patients face. Given the cultural and ethnic diversity of their patients, many of the programs found it beneficial to hire team members with additional language skills and those who reflect the demographics of patients served. Regardless of team composition, many of the programs recognized the need to establish a close relationship with hospital interpreter services departments to facilitate excellent communication with patients and families with limited English proficiency.
Dedicate time for planning
The SPCPHI provided a structure for program development and growth at all 17 sites, and as a condition of participation in the initiative, it required that sites dedicate time to attend grantee conferences and engage in strategic planning. Two sites specifically highlighted the importance of dedicating time for strategic planning, for both program initiation and growth. Key tasks that these sites identified for planning included identifying appropriate staff to provide clinical care and administrative support; providing marketing and education to hospital staff about the program; planning for, collecting, and analyzing program data; developing appropriate templates and policies; and assessing when demand for services and financial impact warrant program growth.
Obtain supplemental funding
One of the most critical components of the SPCPHI was the startup funding provided by the CHCF. This support included funding for palliative care team members' salaries and subsidies to enable their participation in training activities. This financial support was critical both to launch programs in traditionally resource-poor environments and to underscore the legitimacy of and need for subspecialty palliative care. As a condition of participation in the Initiative, hospitals were required to provide matching funds for program development and to track the financial impact of the palliative care programs. Because of these requirements, most of the original grantee sites (75%, n = 8) were able both to weather the systemic budget cuts resulting from the concurrent American recession and to obtain further investment in the palliative care program once the grant period ended.
Despite the importance of hospital support and startup funding, many of the sites were compelled to find additional funding from other sources. At the end of the Initiative, 67% of sites received support from the hospital; 75% continued to receive “in-kind donation” support from the hospital; 8% received grant funding from their hospital foundations; and 25% turned to external grants to support ongoing services. For example, one site was able to leverage support from the local Catholic Archdiocese to provide routine chaplaincy support.
Obtain technical support
Participating sites stated that technical support provided by the faculty and staff involved in the Initiative was critical to the successful establishment of public hospital palliative care programs. All sites were offered initial PCLC training, which equipped program leaders with key skills and knowledge to establish, grow, and sustain palliative care programs. Sites were provided with a core set of data elements that they were required to collect and routinely report on, reflecting program operation and outcomes. These practices in routine data collection and reporting provided a basis for ongoing reporting to hospital administration and participation in quality improvement initiatives. Although many sites had difficulty in accessing hospital financial data, the sites that were able to complete financial impact analyses underscored the value of the technical assistance they received to develop site-specific business cases.
Leverage national data and existing evidence base
Given that many sites reported difficulty in obtaining financial or utilization data from their administration, some sites were able to leverage existing evidence of the positive impact of palliative care services, to initiate or grow their palliative care programs. Literature regarding the impact of palliative care consultation on Medicaid patients, 18 or case examples of palliative care programs in safety net hospitals19,20 were used in combination with tools to predict consultation volume, before initiating or expanding services. Once services were initiated, if financial data were not obtainable, some sites reported using cost data from similar institutions with palliative care programs, whereas others used surrogate measures such as avoided hospital admissions.
Network with other public hospital palliative care programs
Finally, many sites emphasized the value of the learning community created through the SPCPHI. Methods implemented to foster this community included monthly learning community calls, annual grantee meetings, and web-based message boards. These routine opportunities for connection created a forum in which participants could share best practices, collaboratively troubleshoot common issues, network, and provide mutual support. Grantee meetings emphasized the value of contributions of and inter-site collaboration among interdisciplinary team members, which may help sustain team members in the challenging work of providing palliative care to underserved populations.
Indicators of Program Growth and Sustainability
At the conclusion of the extended grant period, all 17 SPCPHI sites reported that they were continuing to provide palliative care services. Although all sites reported challenges to initiation, growth, and sustainability, they also showed evidence of impact beyond direct patient care, including providing education for hospital staff, engaging in quality improvement initiatives, and expanding access to palliative care services for ambulatory patients.
Increasing consultation volume and staffing
During follow-up interviews with all 17 sites, 16 months after the conclusion of the Initiative, the majority of programs reported increases in both consultation volume and staffing, with only one site reporting decreases in both consultation volume and staffing. Despite the challenges in obtaining dedicated funding from city/county administration, seven sites reported successfully obtaining resources from their hospitals to appropriately expand their program staffing to meet increasing service demands.
Participating in education activities
In addition to direct patient care, all 17 sites also dedicated significant effort to providing palliative care training for hospital staff and health professions trainees. Given the well-described workforce shortages in palliative care, 21 the SPCPHI sites heavily invested in promoting primary palliative care. Over the 3-year initiative, the 17 sites reported facilitating more than 1,230 educational sessions, reaching at least 12,165 staff and 6,665 trainees. In addition, three sites also reported more significant investment in training specialists in palliative care, through the development of, or association with, palliative care fellowship programs.
Engaging in quality improvement initiatives
Beyond simple metrics demonstrating increasing consult volume, several SPCPHI sites also were committed to enhancing the quality of services provided, through a variety of mechanisms. Two sites reported efforts to improve the communication of patients' wishes, through increasing completion of Physician Order for Life-Sustaining Treatment (POLST) forms, when clinically appropriate. In follow-up calls 16 months after the end of the Initiative, six sites had become members of the PCQN, 22 a national collaborative focused on defining and promoting high-quality palliative care. At the same time, two sites reported active efforts to pursue The Joint Commission Advanced Certification in Palliative Care.
Expanding access to palliative care services
In addition to the increase in consultation requests, several sites reported efforts to expand palliative care access both in the hospital and in the community. Four sites reported implementing “triggers” for palliative care consults in the hospital, in specific hospital units (e.g., intensive care unit), with specific patient populations (e.g., heart failure patients), and/or among all admitted patients. In addition to proactive outreach in the hospital, several sites reported planning or initiating community-based palliative care programs, through clinic-based services. In follow-up calls 16 months after the initiative ended, 6 sites had already initiated community-based palliative care services, and the remaining 11 sites were actively planning to implement these services.
Conclusions
The SPCPHI was a unique, statewide initiative that helped markedly increase access to palliative care for medically underserved Californians by launching or expanding services in 17 acute care public hospitals. The public hospital palliative care teams faced unique challenges in providing palliative care in the healthcare “safety net.” Data from the Initiative suggest that the patients cared for by palliative care programs in California's public hospitals are younger, more ethnically diverse, and more likely to have a primary diagnosis of cancer than those seen in other not-for-profit hospitals. Patients served by the SPCPHI programs experience significant barriers to accessing care, frequently including language barriers, social barriers (including social isolation and incarceration), and financial barriers (including limited insurance coverage). Palliative care teams at SPCPHI sites reflect the diversity of their patients, with more providers from underrepresented minority groups and many who reported fluency in multiple languages. Teams are the most likely to include physicians, social workers, and advance practice nurses; however, many of the team members work only part-time with the palliative care team, and few teams have clerical support.
Similar to many palliative care teams nationwide, SPCPHI sites reported feeling understaffed to meet the demand for services. They also reported additional challenges related to the governance and regulatory structures common in public hospitals; limited and uncertain funding from their city/county government; limited access to hospital financial data and analytic support; and administrative and palliative care staff turnover. Although these challenges to program sustainability and growth were significant, SPCPHI sites found ways to overcome them, including obtaining supplemental funding to catalyze program initiation/expansion and to support strategic planning and staff development; learning from palliative care peers in other public hospitals; obtaining technical support for data collection and analysis; and leveraging national data when local data were unavailable.
Postinitiative follow-up suggests that the SPCPHI was highly successful, with a greater than 400% increase in the prevalence of inpatient palliative care services in California's public hospitals from 2009 to 2013. This growth translated into a substantial increase in access to services for vulnerable Californians, with the 17 programs providing care to more than 15,000 Californians in 30 months. All 17 SPCPHI sites were continuing to provide consultation services several months after the end of the Initiative, with most sites reporting increased consultation volume and actively planning for program expansion. In addition, many programs reported contributing to quality improvement and education initiatives at their sites, and most became members of the PCQN, a national palliative care quality improvement collaborative. These findings suggests that the SPCPHI succeeded in catalyzing and expanding access to palliative care for the millions of Californians who depend on these 17 hospitals for acute care services.
The primary limitation of this article is that it focuses on a single initiative in a single state. Palliative care programs in other states are likely to encounter unique challenges based on the availability of resources for vulnerable populations, Medicaid regulations and reimbursement, and demographics. Additionally, California is a very large state with 17 public hospitals, which allowed for peer support and shared learning. Initiatives in states with fewer public hospitals might consider partnering with each other, with California public hospitals, or with the Safety Net Hospital Special Interest Group of the American Academy of Hospice and Palliative Medicine, to create the support community that was so important to the success of the SPCPHI. Furthermore, since the SPCPHI was a philanthropically funded initiative, we cannot comment on the likelihood of palliative care program development in the absence of this external funding, beyond the low prevalence of palliative care services before the Initiative. However, it may be possible to find philanthropic support for similar initiatives in other states and regions. In addition, it is important to note that the CHCF provided startup funds, whereas all palliative care programs were subsequently supported by institutional funds, suggesting that although foundation support is helpful in catalyzing program development, it may not be mandatory.
Despite many challenges faced by palliative care programs in public hospitals, the SPCPHI provides strong evidence that such program development, growth, and sustainability is possible, and it provides guidance for how to accomplish it. The hard work is well worth the effort, as it provides access to palliative care for vulnerable patients and addresses disparities in access to quality care.
Footnotes
Acknowledgments
The authors would like to thank Melissa Ramos, of Learning Partnerships, for her assistance with project management and with follow-up phone calls to SPCPHI sites; and the CHCF, for sharing project data reports and narrative reports. They also thank all the SPCPHI sites that shared their insights and ideas with them. The SPCPHI would not have been possible without the leadership and advocacy of the CHCF, and the support of the California Association of Public Hospitals-Safety Net Institute, the UCSF PCLC, and Learning Partnerships.
Author Disclosure Statement
No competing financial interests exist.