
Abstract
M
As teams struggle to meet new demands, they inevitably ask for additional staff, often met with administrative indifference, in part due to the teams' inability to adequately make the case for more resources in a manner that aligns with health system priorities, leading to staff frustration and further deterioration in team function. In prior editorials I have written about the dangers of being a team martyr and how teams can embrace the new reality of increasing clinical demand by starting to shift some of their work to support increased generalist-level palliative care training and system-change efforts.1,2 Although I find some teams working to embrace these ideas, far too many are trapped in an unproductive cycle of feeling overwhelmed and underappreciated. In this editorial I outline some concrete steps teams can take to move forward.
1. Self Care/Team Care
A principle of palliative care is that before you can help a patient establish goals, physical symptoms need to be well managed. Similarly, before teams can move forward they need to openly address issues of team health and correct dysfunctional team behaviors, including martyrdom. Since palliative care specialist clinicians are a scare resource, all teams need a proactive strategy for both prophylactic and interventional team health. At a minimum, teams should complete a self-assessment of team function and develop a plan for consistent activities to both assess and promote improvements in team health. 3
2. Workload Assessment
Teams are buffeted by increasing demands for clinical services and by new administrative imperatives to expand services to new patient populations and new care venues. Most teams approach these requests as if they have no voice in decision making, not wanting to offend administrators or colleagues who request their services. Thus, a key step is for teams to step back, take a deep breath, and gain some control over their own destiny. A few key questions can begin the process:
• Are there opportunities to change daily work processes to increase efficiency without abandoning core palliative care principles? • Are there patients that no longer need team follow-up in which the team can “sign off”? • Are there frequent consultations that are outside staff knowledge/skills? • Are there frequent consultations that are outside the program scope of practice? • What percentage of consultations represent generalist-level palliative care, as compared to true specialist-level consultations? • Can some of the generalist-level requests be managed by curbside advice, rather than a full consultation?
Once these questions are discussed and teams recognize the gap between current and desired practice, they need to give themselves permission to set boundaries around their services and set program goals that realistically match their resources. Some will argue that setting limits around consultation practice has the potential to anger referring clinicians, leading to a drop in consultation volume. In the past, when we often struggled to prove our value, this was a reasonable concern. But such is not the case anymore for programs that are growing beyond their resources. Setting limits is a natural evolutionary step in program development that reinforces the notion that we are a true specialty, rather than a “feel-good” service for any and all needs of sick patients.
3. Scope of Services
Most teams, at the time of program inception, develop a marketing message including indications for referral. But seldom do I see teams make changes in how they market themselves as their program grows. The most common issues I see teams struggle with as they get busier are how to handle requests for chronic nonmalignant pain management, substance abuse assessment, hospice informational visits, and requests to manage time-intensive procedures such as a planned ventilator withdrawal. Each team needs to decide the relative value of their time and expertise in handling these and similar requests, in comparison to the more traditional palliative care specialty consultations for symptom management, conflict resolution, goal setting, and discharge planning. 4 To help teams realign their resources with current clinical demands, I encourage all teams to develop a Scope of Services document, reassessed annually, that outlines four domains: indications for referral, diagnoses suitable for referral, consultation management options, and team availability (see Fig. 1).
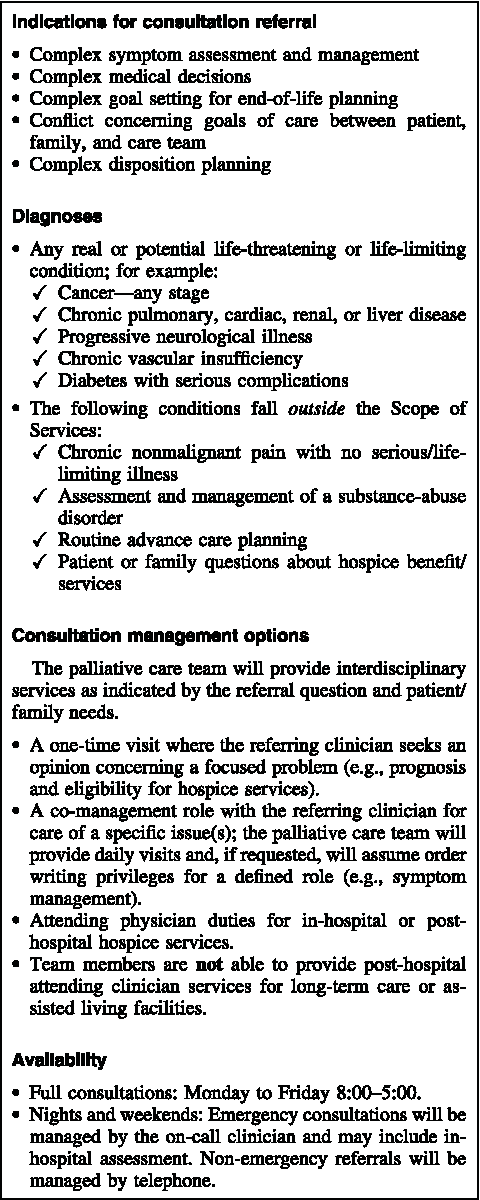
Palliative Care Consultation Service: Scope of Services (SAMPLE).
4. Service Standards
Service standards define how a team operationalizes their day-to-day work. This is vital information both for the team itself, especially when new staff are added, and for referring clinicians. Establishing a list of service standards is an excellent team building exercise that, like the Scope of Services, should be reviewed annually. Key domains of service standards include daily work process, interactions with referring clinicians, and other components specifying the who-does-what-when of the interdisciplinary team (see Fig. 2).

Palliative Care Consultation Service: Service Standards (SAMPLE).
5. Strategic Planning
Strategic planning is a process to define a program's goals and make decisions on how to achieve those goals based on available resources, or in the words of Yoggi Berra, “If you don't know where you are going, you might not get there.” 5 Strategic planning for palliative care teams involves an analysis of current work, assessment of opportunities for new services, appraisal of staffing resources necessary to expand into new programmatic areas, and making a plan to operationalize the steps necessary to achieve the desired goals (see Fig. 3). Strategic planning involves the palliative care team and key stakeholders, including health system administrators, key clinicians, and others necessary to get the big picture of how palliative care services can best impact the health care enterprise. Program leaders who are unsure of how to go about a strategic planning process can usually find someone from hospital administration to help guide the process.

Strategic Planning Process Steps.
Summary
The five elements outlined here should not be thought of as linear steps to be completed in the order of presentation, but rather a cycle of work processes. A natural starting point is to first work on team health and complete a strategic planning process and workload assessment, with subsequent changes made to the Scope of Practice and Service Standards. As teams work through the five elements they should also ponder their potential to impact the local health care culture beyond specialist consultations. I find that many teams are fixated on increasing their consultation volume as the key measure of value and impact. Indeed volume is one measure of how well the palliative care team is viewed by referring clinicians. But focusing on consultation volume alone limits the vision of what palliative care, as a force for culture and practice change, can achieve.
Forward-thinking hospitals and health systems are starting to recognize that palliative care services represent more than an end-of-life service line; palliative care concepts that are widely integrated can have positive impacts that ripple through all aspects of the institution and improve outcome metrics that administrators care about. If I were a hospital administrator, I would want the specialty team to spend no more than 50% of their time seeing consultations, and the other 50% working on elements of systems/culture change with a goal of improving the care of all patients with unmet palliative care needs, not just those fortunate enough to be referred for consultation. 6 Furthermore, I would change how palliative care clinicians are evaluated for productivity, from a system based on clinical patient volume and billing to one focused on culture change that brings about a true system of patient-centered care.
Systems change work includes educating our colleagues in generalist-level palliative care, developing screening pathways to identify patients with unmet needs, patient/family and community education, quality improvement processes, and establishment of standards, tools, and metrics to improve and measure patient-centered care.2,6 Granted, most palliative care clinicians today view themselves as clinicians first, rather than as agents for system change or education. And yet, when I meet with teams, it is the lack of culture change (e.g., “Why did the emergency physician admit this dying patient to the intensive care unit” or “Why did this patient suffer for three days with severe pain before they called us?”) that is an ever-present source of team distress.
In the early days of our specialty, the vision of palliative care was that it could positively impact the cure at all costs culture of health care and help shift care from clinician-centered to patient-centered. Starting a specialty consultation service was viewed as one of many important building blocks in realizing this goal. To fully realize that early vision, specialist teams can continue their good clinical work, but also seek out opportunities to change the larger culture of care through systems change and education. As a first step, teams need to remind themselves that they have control over how they meet the increasing demands for their time and services through self and team care, defining the boundaries of their services, and strategic planning.