
Abstract
Abstract
Background:
Objective Prognostic Score (OPS) was developed as an easy and simple prognosticating tool in South Korea. It has been validated retrospectively in a single center in South Korea.
Objective:
We aimed to validate the OPS prospectively for advanced cancer inpatients in South Korea using a multicenter study.
Design:
This was a prospective cohort study.
Setting/Subjects:
We enrolled 243 advanced cancer patients admitted in five palliative care units in South Korea from May 2013 till March 2015. Seven members of the Korean Palliative Medicine Research Network who are experts of palliative care led the study.
Measurements:
Clinical variables (dyspnea/anorexia/performance status) and laboratory variables (total leukocyte counts/serum total bilirubin/serum creatinine/lactate dehydrogenase) were collected at the enrollment. Survival time was calculated as days from enrollment to death during admission.
Results:
A total of 217 patients were included in the final analysis (feasibility: 89.3%). Survival time of the higher OPS group (OPS ≥3) and the lower OPS group (OPS <3) was 10.0 (95% confidence interval (CI) 7.72–12.28) days and 32.0 (95% CI 25.44–38.56) days, respectively. There were significant differences between the 2 groups (p < 0.001). Overall accuracy of OPS ≥3 for predicting survival less than three weeks was 71.0%.
Conclusions:
OPS was successfully validated using a prospective multicenter study in South Korea. It is a useful method to predict three-week survival of Korean inpatients with advanced cancer.
Introduction
P
Prognostic scores encompassing various variables are developed to assist physicians' prognostication in palliative care. Generally, variables include performance status, signs, and symptoms such as laboratory data and clinical prediction of survival (CPS).1,4 Palliative Prognostic Score (PaP) and Palliative Prognostic Index (PPI) are the most widely used and validated prognostic scores worldwide.5–9 However, PaP is not user friendly for the less experienced physicians. 10 PPI poses a challenge for physicians when diagnosing delirium.
Objective Prognostic Score (OPS) was developed through a multicenter prospective study in Korea in 2010. 11 Its aim is to function as an easy and quick scoring system. The validation of prognostic scores is crucial. 12 Second-step validation of OPS, as well as comparing to other prognostic scores, was performed using retrospective data in a single center.13,14 Therefore, we aimed to validate OPS prospectively for advanced cancer inpatients in South Korea through a multicenter study.
Materials and Methods
Subjects
Subjects of this study were inpatients admitted to five palliative care units (PCUs) of South Korea from May 2013 to March 2015. Seven palliative care experts of the Korean Palliative Medicine Research Network led the study. Inclusion criteria were as follows: (1) patients with advanced cancer undergoing palliative care; (2) older than 18 years; (3) voluntary participation; and (4) CPS <3 months. Exclusion criteria were as follows: (1) patients who did not agree to participate; (2) currently receiving chemotherapy and radiotherapy for cancer cure; (3) hematological malignancies; and (4) chronic renal failure. All patients were transitioned from active anticancer therapy to a focus on supportive care. Palliative chemotherapy or palliative radiotherapy was allowed with purpose of symptom control. Informed consent was provided to patients and their families. The protocol of this study was approved by the institutional review boards of each institution.
Data collection
This study was a prospective observational study. Clinical data were recorded by trained professionals under the supervision of each investigator. Total leukocyte counts, serum total bilirubin, serum creatinine, and lactate dehydrogenase (LDH) were recorded using routine laboratory data of the enrollment day or nearest date (within seven days) to the enrollment. Performance status of patients was assessed using Eastern Cooperative Oncology Group (ECOG, range: 0–4) performance score. 15
Resting dyspnea and anorexia were assessed according to the judgment of each investigator physician based on conversation with patients and their families or direct patient observation. Anorexia was defined as <5 spoons per meal, which was a third of a typical Korean meal. Survival time was calculated as days from enrollment to death during admission.
Objective prognostic score
OPS was developed for its easy applicability, minimizing subjective variation (i.e., CPS), and an integrated model. OPS consists of two symptoms (anorexia and resting dyspnea), one performance score (ECOG), and four laboratory data (total leukocyte counts, serum total bilirubin, serum creatinine, and LDH). OPS ranged from 0.0 to 8.0 points. The overall accuracy for three-week survival was 75.5% with a cutoff score of 3.0. 11
Statistical analysis
Survival curves were constructed by the Kaplan–Meier method. Comparison of survival time was performed using log-rank test. Cases transferred to other hospitals, discharged from hospitals, and survived at end of study were considered censored data. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of OPS ≥3 for less than a three-week survival were calculated. All statistical analyses were performed using the SPSS statistical package for Windows version 22 (IBM, Armonk, NY). The significance level was set at p < 0.05.
Results
A total of 243 subjects were enrolled. Among all subjects, 26 were excluded due to lack of laboratory data for calculating OPS (feasibility: 89.3%). One hundred ninety subjects were confirmed in-hospital mortality cases.
General characteristics of all subjects are described in Table 1. Mean age was 65.1 years. Lung cancer was the most prevalent primary cancer (24.5%). About half of subjects were in bed-ridden state (ECOG 4: 45.2%). Median value of survival time was 14 days (95% confidence interval [CI]: 11.6–16.5).
CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; SD, standard deviation.
Among 217 subjects whose OPS was calculated, 129 (59.4%) subjects showed OPS ≥3 and 88 (40.6%) subjects had OPS <3. Table 2 shows each distribution of OPS items.
Objective Prognostic Score ranges from 0.0 to 8.0 points.
Five or less spoons per meal (1/3 amount of routine meal in Korea).
LDH, lactate dehydrogenase.
Median of survival time of the higher OPS group (OPS ≥3) was 10.0 days (95% CI 7.72–12.28) and that of the lower OPS group (OPS <3) was 32.0 days (95% CI 25.44–38.56). There was a statistically significant difference between the two groups (p < 0.001, obtained by log-rank test, Fig. 1).

Survival curves according to OPS group (n = 217). Survival time (10.0 [95% CI 7.72–12.28] vs. 32.0 [95% CI 25.44–38.56] days) was significantly shorter in the higher OPS group (OPS ≥3, n = 129) than the lower OPS group (OPS <3, n = 88; p < 0.001). p-Value was obtained by log-rank test. Data were expressed as median value. CI, confidence interval; OPS, Objective Prognostic Score.
Area under ROC curve (AUROC) of predictability of OPS for three-week survival was 0.743 (95% CI 0.675–0.810, Fig. 2).
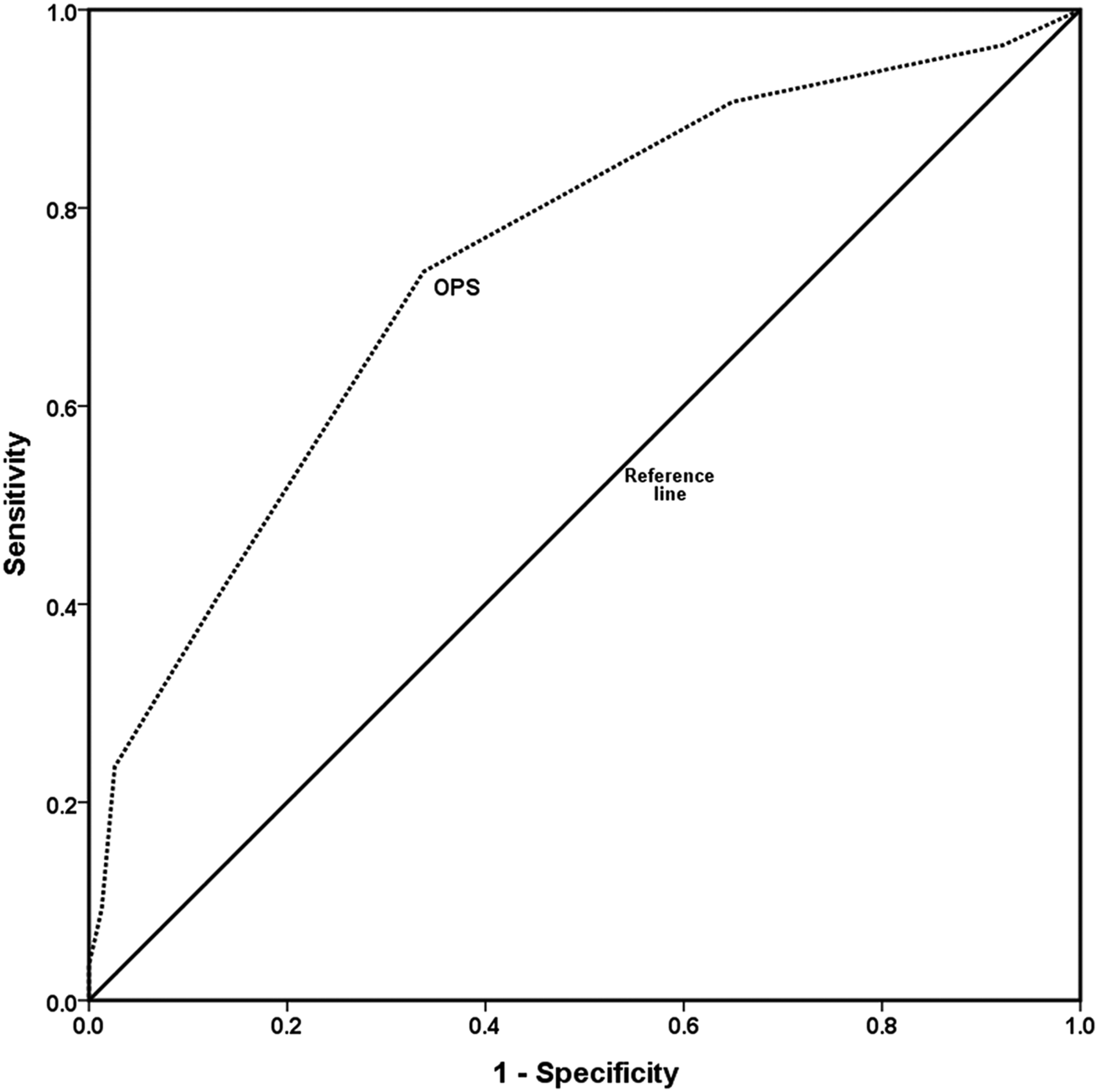
Receiver operating characteristic curve for three-week survival (n = 217). Area under receiver operating characteristic curve was 0.743 (95% CI 0.675–0.810) for OPS.
Sensitivity, specificity, PPV, NPV, and overall accuracy of OPS ≥3 for less than three-week survival were 73.6%, 66.2%, 79.8%, 58.0%, and 71.0%, respectively.
Discussion
We successfully validated the accuracy of OPS for predicting three-week survival in Korean inpatients with advanced cancer using a prospective multicenter study.
Survival estimation is the most vital parameter when making decisions on active treatments in palliative care. Approximately one month's survival is useful in decision making of more intensive care such as palliative surgery or procedures. Therefore, predicting three-week survival using OPS would be helpful in making a decision. Survival estimation is a guideline to prepare patients themselves and their families. Palliative patients often decease without any prearrangements of business and family matters. At times, families of dying patients miss the opportunity to say good bye to their loved ones because they do not have proper information about patients' survival. OPS could be utilized to avoid such overly optimistic expectations in such cases.
Our results showed that survival time of the higher OPS group (≥3) was significantly shorter than that of the lower OPS group (<3), which was consistent with previous studies.11,13,14 In this study, PPV, overall accuracy, and AUROC of OPS ≥3 for three-week survival were 79.8%, 71.0%, and 0.743, respectively, which was consistent with previous findings. Therefore, OPS using cutoff 3 can be regarded as an accurate estimate for three-week survival.
In our results, specificity and NPV of OPS ≥3 for three-week survival were 66.2% and 58.0%, respectively. It was lower than those of previous original OPS study (specificity 77%, NPV 79%). 11 These values were lower in succeeding studies than in original OPS study. Low NPV indicates that there were some patients who lived less than three weeks despite having OPS <3. It is possible that unexpected events such as embolism and hemorrhage caused sudden deaths. Carefully designed studies to detect such events are required in future. In practice, prognostication of shorter survival than longer survival is more important for patients and their families. Therefore, we believe high PPV and NPV are important indicators as a good prognostic score in estimating life expectancy of terminally ill patients.
In this study, median survival of all subjects was 14 days. Interestingly, all patients of studies subsequent to the original OPS study showed poorer general condition (ECOG 4; 45.2% of subjects in this study vs. 37.8% of original OPS study) and shorter actual survival than those of the original study. Application of OPS to patients with longer survival merits further research.
One of the biggest advantages of the OPS is the ease of use for anyone, including inexperienced medical professionals in palliative care. PaP is generally regarded as the most accurate prognostic score in practice and research. However, inexperienced palliative care physicians may encounter difficulties in selecting six categories (1–2, 3–4, 5–6, 7–8, 9–10, 11–12, >12 weeks) of CPS in PaP. OPS does not include CPS, thus it is easier than PaP. PPI is a useful prognostic score when laboratory data are unavailable. However, inexperienced medical professionals may have difficulties in dividing Palliative Performance Scale categories (especially 20 or 30, 50 or 60) in PPI. Moreover, PPI requires diagnosis of delirium based on the Diagnostic and Statistical Manual of Mental Disorders IV, which mandates the physicians' experience. Recently, simplified PPI was developed to solve this issue. 16 Comparing OPS to PaP and PPI can solve if the subjectivity of PaP or PPI makes it harder to use or less accurate. In a retrospective study, OPS was compared to PaP and PPI and showed no significant differences. 14 However, in this study, there was no prospective comparison of OPS to PaP and PPI. Therefore, any conclusions regarding its accuracy cannot be drawn.
We recognize the limitations of this study. First, this study was performed in PCUs in Korea. Thus, our results may not be generalized to patients under palliative care worldwide. Second, 10.7% of our study subjects lacked some laboratory data for OPS. However, feasibility of 89.3% was in the acceptable range. Third, all subjects were inpatients admitted to PCUs. Thus, further studies are required to extend the current findings to patients in diverse palliative care settings. It is also important to note that actual survival of our patients was relatively short. Thus, additional research may be necessary to extend our findings to patients with longer life expectancies. As well, laboratory data of the enrollment day or nearest date (within seven days) to the enrollment were used for calculating OPS. In considering survival time with such variation between enrollment and collecting laboratory data could have some impact on results. Finally, the invasiveness of blood tests is sometimes questioned. However, laboratory monitoring is routinely performed as a part of inpatient care. Investigators may use laboratory data to detect earlier phases of disease trajectory in future studies in early palliative care.
This is the first prospective study as a second-step validation of OPS for Korean advanced cancer patients using a multicenter design. OPS has strengths where medical professionals can easily use it without skillful clinical judgment. Future studies on OPS should include patients of diverse ethnicities in various palliative care settings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.