
Abstract
Abstract
Background:
Palliative cancer patients suffer from high levels of distress. There are physiological changes in relation to the level of perceived distress.
Objective:
To study the efficacy of 5 minutes of mindful breathing (MB) for rapid reduction of distress in a palliative setting. Its effect to the physiological changes of the palliative cancer patients was also examined.
Methods:
This is a randomized controlled trial. Sixty palliative cancer patients were recruited. They were randomly assigned to either 5 minutes of MB or normal listening arms. The changes of perceived distress, blood pressure, pulse rate, breathing rate, galvanic skin response, and skin surface temperature of the patients were measured at baseline, after intervention, and 10 minutes post-intervention.
Results:
There was significant reduction of perceived distress, blood pressure, pulse rate, breathing rate, and galvanic skin response; also, significant increment of skin surface temperature in the 5-minute MB group. The changes in the 5-minute breathing group were significantly higher than the normal listening group.
Conclusion:
Five-minute MB is a quick, easy to administer, and effective therapy for rapid reduction of distress in palliative setting. There is a need for future study to establish the long-term efficacy of the therapy.
Background
P
As a result, various psychosocial methods were introduced for reduction of distress in palliative cancer patients. Of all the psychosocial interventions, mindfulness-based intervention has shown some efficacy in promoting relaxation and reducing psychological stress.5–9 Although mindfulness-based interventions are useful in reducing various forms of psychological stress, its application in the palliative care settings is not without its challenges. Patients may have fluctuating levels of consciousness, psychological distress, or physical disabilities. Palliative care cancer patients are physically weak and lethargic to go through a series of lengthy psychotherapy sessions. To address these challenges, a 5-minute mindful breathing (MB) technique was proposed. 10
The 5-minute MB is based on a series of mindful practices. From a range of mindfulness practices, MB was selected for the study because humans breathe every second of every day. Breathing is both an involuntary and voluntary physiological process; it is controlled voluntarily by the motor cortex but also controlled automatically by the brainstem. Practicing MB allows the patients to practice it anytime and anywhere they want. MB represents a main practice that serves as an anchor for the other mindful practices, such as mindfulness walking and mindfulness meditation. 11
Current literature suggests that psychological distress in palliative patients tends to be underdiagnosed and undertreated. 12 This is because palliative patients often experience distress that is not well characterized within the context of Diagnostic and Statistical Manual of Mental Disorders phenomenology. 13 Therefore, it is important to screen for psychological distress among palliative cancer patients by using a measurement that is suitable for them. Common tools used in measuring psychological distress are self-rating questionnaires such as the Hospital Anxiety and Depression Scale 14 and Beck Depression Inventory. 15 The patients answer the self-rated questionnaires subjectively, based on their feelings. However, their answers may be susceptible to response biases. 16 For example, patients may respond based on social desirability. In the palliative care setting, patients are often too fatigued and weak to go through the self-rating questionnaires and interview questions. Individuals are assumed to answer the question with response biases when they are more fatigued, more burdened, and less motivated. Therefore, a nonburdensome and nonsubjective method should be considered in measuring the psychological distress among palliative cancer patients. The present study suggests that physiological responses could be one of the indicators in measuring psychological distress.
When humans are stressed, the sympathetic nervous system is activated and it stimulates the adrenal glands to release catecholamines (e.g., epinephrine, norepinephrine). Epinephrine elevates the cardiac output, which increases blood flow to the heart, brain, and airways to increase available oxygen to the bloodstream and muscles. Norepinephrine constricts blood vessels of the viscera and skin and shunts blood to the vessels dilated by epinephrine. In response to these hormones, the human body experiences physiological changes and enters the “fight or flight” mode.17–20 Measurable indicators of increased catecholamine levels include blood pressure, heart rate, respiratory rate, and galvanic skin response. 21 However, the physiological responses only are indirect indicators and are not conclusively diagnostic because they can be influenced by side effects of certain pharmaceuticals, pain, or medical conditions. Although physiological responses are indirect indicators and cannot predict stress levels per se, it is suggested that there will be a relationship between physiological changes and stress levels.17–21
To date, there is no study on the effect of MB on the perceived level of distress together with the changes in the physiological responses among palliative cancer patients. Therefore, the present study aims to study the efficacy of 5 minutes of MB on the reduction of perceived level of distress among palliative cancer patients. At the same time, this study aims to study the changes of the physiological responses in palliative care cancer patients with 5 minutes of MB therapy.
Methods
This randomized controlled study was conducted in the palliative care unit, University Malaya Medical Centre. The inclusion criteria are (1) 18 years and older, (2) with the diagnosis of cancer of any type, (3) under palliative care, (4) the score of distress is more than 4 based on the measurement on the distress thermometer, (5) able to understand and follow simple instructions, and (6) consented. The exclusion criteria are (1) those who are delirious or confused, (2) those with breathing difficulties/respiratory distress, and (3) unable to maintain concentration for at least 20 minutes (based on the subjective assessment of the researcher during the process of interview and explanation of the study). Patients from the palliative care unit were approached and screened for eligibility. Those who fulfilled the criteria were recruited into the study, and explanation about this study was offered to their family members and caretakers. Their sociodemographic background information was collected. The relevant clinical data (type of cancer, other comorbid medical conditions, and medications) were obtained from the medical records.
Based on the previous literature, we measured the physiological parameters that were correlated with psychological distress.17–21
The following measurements were taken:
(1) Perceived level of distress using distress thermometer (2) Skin surface temperature (3) Galvanic skin response (4) Blood pressure (5) Pulse rate (6) Breathing rate
Distress thermometer
The distress thermometer is a validated rapid screening tool for psychological distress and has been endorsed by the NCCN Distress Management Guidelines panel. It serves as an initial single-item question screen, which identifies distress from any source. The word “distress” was chosen because it sounds “normal” and is less embarrassing to patients. It assesses how much distress patients went through in the past week. The subjects were instructed to circle from a scale of 0 to 10 to indicate their distress level, where “0” means no distress and “10” means extreme distress. 22 In the previous literature review, most studies showed that the score of 4 has the maximum sensitivity and specificity relative to established criterion. 23
Skin surface temperature measurement
Dr. Lowenstein's Stress Thermometer SC911 was used to measure the skin surface temperature. The stress thermometer (ST) SC911 is widely used in clinical research to identify stress levels and relaxation, as well as to see how cognition and emotion impact the human body.24–28 A decrease in skin surface temperature indicates tension, during which individuals experience nervousness, worry, or stress, while an increase in skin surface temperature indicates relaxation, during which individuals are in a peaceful emotional state. The ST displays the hand skin surface temperature ranging from −58°F to 158°F. When individuals are extremely stressed, their skin temperature will drop to less than 79°F, while when individuals are very relaxed, their skin temperature will increase to more than 95°F.
Galvanic skin response measurement
Skin response, also known as galvanic skin response, skin conductance, or electrodermal response, is a measurement method based on bioelectrical properties of the skin. 29 The galvanic skin response was recorded by using the Mindfield eSense Skin Response Biofeedback System. It has been used in previous clinical research.30,31 The Mindfield eSense Skin Response Biofeedback System applies a very safe and small electrical voltage and sets up an electrical current in the skin. Activity of the sweat glands in the skin is measured by changes of the electrical current. When individuals are stressed, the activity of the perspiratory glands will increase and this is indicated by an increase in the skin conductance response. When individuals are calm, the skin conductance response will decrease, indicating low activity of perspiratory glands. The skin conductance was measured in microsiemens (μS).
Blood pressure and heartbeat measurement
An Omron blood pressure monitor was used to measure the blood pressure and heart rate. The monitor measures blood pressures between 0 and 299 mmHg, and a pulse rate between 40 and 180 beats/min. When individuals are stressed, the blood pressure and heart rate will increase in response to the activation of the sympathetic nervous system.
Procedure
The perceived level of distress and physiological responses were measured at the beginning of the sessions (T1). The subjects were then randomly assigned to the intervention arm (5 minutes of MB) or the control arm (normal listening) for 5 minutes. The perceived level of distress and physiological responses were reassessed after the completion of the first session (T2). After a short break (5 to 10 min), the measurements were taken again (T3).
Normal listening
In the normal listening group, the subjects were interviewed using the following list of standard semistructured questions for 5 minutes:
(1) Could you tell me about your illness? (2) Could you tell me about yourself? (3) What about your life? (4) What about your family and friends? (5) What are the things that are important to you? (6) Is there anything else that you would like to share with me?
Five minutes of MB
In mindfulness-based therapy, the subjects are taught to increase their awareness through paying attention in a particular way, on purpose, in the present moment, and nonjudgmentally, following the steps below:
(1) Step 1—Adopt a physical posture A good physical posture helps to maintain a healthy mental posture. For example: Sitting upright on a chair. (2) Step 2—Establish a mindfulness anchor. Tie the mind to the present moment. For example: Pay awareness to the breathing. (3) Step 3—Maintenance of mindfulness Maintain the focus to the present moment and regulate ruminations. For example: Count the breathing. Do not force breathe.
The participants are instructed to relax their body, close their eyes, and focus their attention on their breathing. If they notice any distractions, such as sounds, body sensations, thoughts, or feelings, they are told to gently redirect their attention back to their breathing. They are told to focus their attention on their breathing for 5 minutes, and the palliative care physician will sit and practice the mindfulness breathing together with the participants during the sessions.
Statistical analysis
The within-subjects changes in the level of distress and physiological responses (systolic blood pressure, diastolic blood pressure, pulse rate, breathing rate, skin surface temperature, and galvanic skin response) pre- and postsession were analyzed using the Wilcoxon signed-rank test. The between-groups (MBT versus normal listening) differences in the changes of level of distress (T2 versus T1 and T3 versus T1) were compared using the Mann–Whitney test. All the tests were two tailed with a significant level of 0.05. All the analyses were performed using SPSS version 12.
Results
Participants
Sixty patients were recruited for the study. All patients completed their participation in this study. Figure 1 provides an overview of the numbers of subjects screened, excluded, randomized, and completed the study.
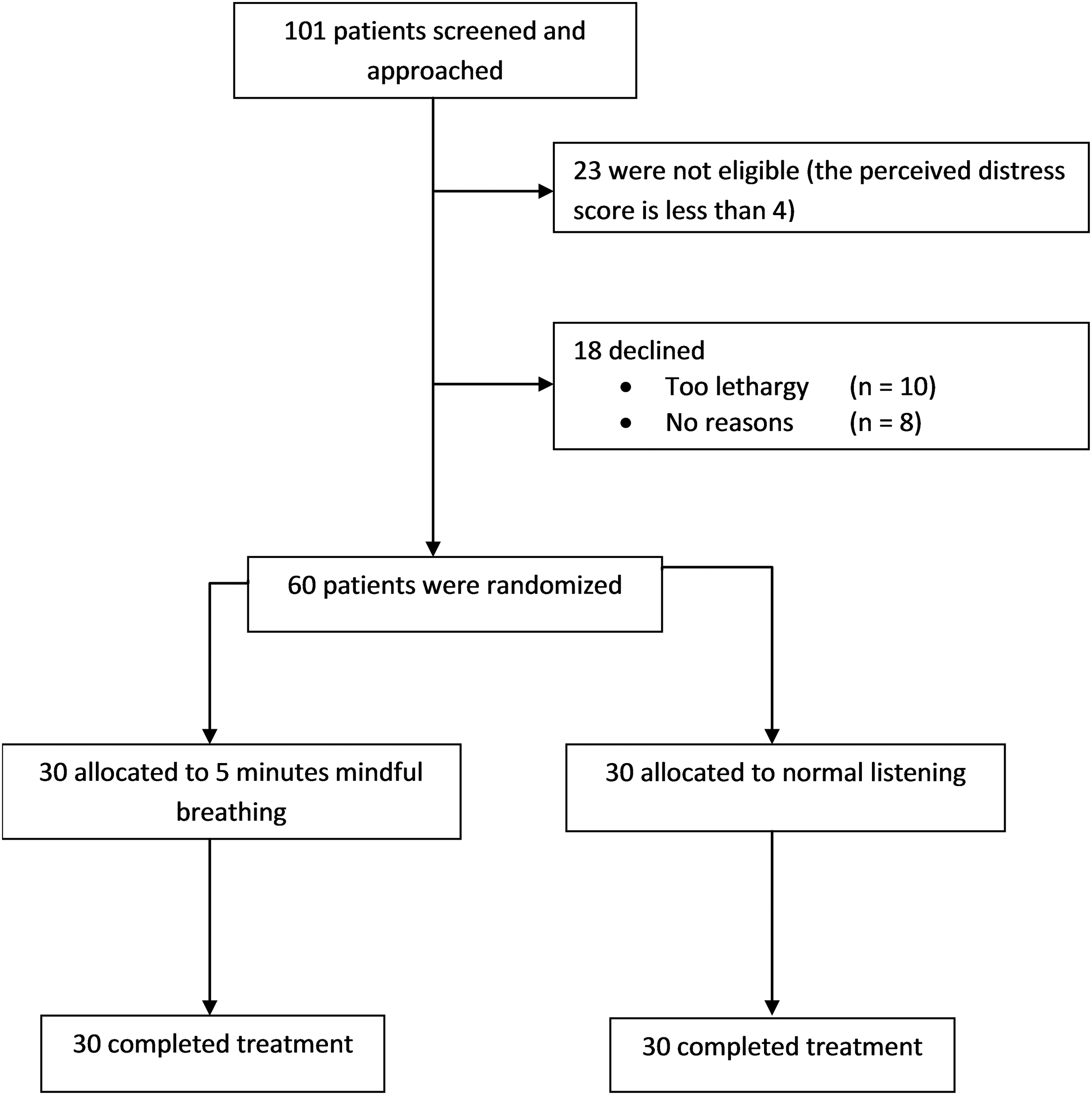
Disposition of patients in the randomized controlled trial between 5 minutes of mindful breathing and normal listening for cancer patients under palliative care.
Sociodemographic characteristics and cancer types
The average age of the patients is 47 years old. The majority of them were Chinese (60%) followed by Malay (23%) and Indian (15%). The commonest religion was Buddhism (40%) followed by Islam (23%) and Christianity (20%). There were slightly more female (51%) than male participants. Most of the patients were married (68%). The two commonest types of cancer were bone (18%) and breast (16%). The others cancer types included lung, nasopharyngeal, liver, pancreatic, prostate, testicular, esophageal, and cervical cancer (Table 1).
Efficacy
Perceived level of distress
There was significant reduction of perceived levels of distress post-intervention at T2 and T3 for patients in the intervention group (p < 0.01). There were no changes in the levels of perceived distress before and after intervention for patients in the control group. As such, the reduction of perceived distress in the intervention group was significantly more than the control group (p < 0.01) (Table 2).
Distress = psychological distress based on distress thermometer, breathing rate = breathing per minute, systolic and diastolic blood pressure in mmHg, pulse rate = pulse per minute, skin surface temperature in °F measured using Dr. Lowenstein's stress thermometer SC911, galvanic skin response in microsiemens measured using Mindfield eSense Skin Response Biofeedback System, the within-group changes (T1 vs. T2 and T1 vs. T3) were analyzed with Wilcoxon signed-rank test, the between-group (5 minutes of mindful breathing vs. normal listening) differences in changes were analyzed using Mann–Whitney test. T1 = Time point before intervention, T2 = time point immediately after intervention, T3 = 10 minutes after intervention.
Breathing rate
The mean breathing rate of patients in the intervention group reduced from 20 breaths per minute at the baseline to 19 breaths per minute at T2 and T3. These changes were statistically significant (p < 0.01). For the patients in the control group, there were no changes in the breathing rate. There was a significant difference in the comparison of the reduction of breathing rate between the two groups at T2 and T3 (p < 0.01) (Table 2).
Systolic blood pressure
The mean systolic blood pressure of patients in the control group reduced from 127 mmHg at baseline to 120 mmHg at T2 and 124 mmHg at T3. The reduction of systolic blood pressure was statistically significant within the interventional group (p < 0.01). There were no significant changes in the control group. The reduction in the mean systolic blood pressure in the MB group was significantly higher than the control group (p < 0.01) (Table 2).
Diastolic blood pressure
Similar to data from patients' mean systolic blood pressure, there was a reduction of mean diastolic blood pressure of patients from the intervention group from 78 mmHg at baseline to about 75 mmHg at T2 and T3, which is statistically significant (p = 0.02). There was no change in the control group. Overall, there was a significant difference between the intervention and control groups in the reduction of mean diastolic blood pressure (p < 0.05) (Table 2).
Pulse rate
There was also significant reduction of pulse rate from an average of 91 beats per minute to 87 beats per minute at T2 (p < 0.01) and 88 beats per minute at T3 (p = 0.06) in the intervention group. The average pulse rates were about 88 beats per minute to 89 beats per minute in the control group. In the comparison between the two groups, the intervention group showed significant reduction of pulse rate (p < 0.01) (Table 2).
Skin surface temperature
The skin temperature in the intervention group increased significantly from 87°F to 89°F at T2 and T3 (p < 0.01). Although there was also significant increment in the skin temperature in the control group from T1 to T2 (p = 0.02), the changes diminished at T3 (p = 0.05). The changes in the intervention group were significantly higher than the normal listening group at T2 (p = 0.05) and T3 (p = 0.03) (Table 2).
Galvanic skin response
The galvanic skin response in the intervention group reduced from the average of 0.9 to 0.75 μS at T2 and 0.73 μS at T3. The changes were statistically significant (p < 0.01). The galvanic skin response was measured using the Mindfield eSense Skin Response Biofeedback System. There was no reduction in the galvanic skin response in the control group. The reduction of galvanic skin response in the treatment group was significantly different from the control group at T3 (p < 0.01) (Table 2).
Discussion
This is the first study to examine the efficacy of 5 minutes of MB on the rapid reduction of perceived distress among palliative cancer patients. The effect of 5 minutes of MB on physiological responses was also studied. Five minutes of MB showed favorable results where there was a significant reduction of distress among the study subjects. For the physiological parameters, there was a reduction in the mean breathing rate, blood pressure, pulse rate, and galvanic skin response in the patients who were randomized to the intervention arm with increases in the skin surface temperature.
The effectiveness of 5 minutes of MB in the reduction of perceived distress among palliative cancer patients is consistent with our previous pilot study. In our pilot study, 20 subjects who were either patients or caregivers demonstrated a significant rapid reduction in distress levels with 5 minutes of MB therapy. 10 There are a number of meta-analyses on the efficacy of mindfulness-based therapy or mindfulness-based stress reduction (MBSR) therapy in cancer patients. The meta-analysis by Ledesma and Kumano, which included 10 randomized controlled trials and observational studies, showed that MBSR was helpful for the mental health of the cancer patients with a Cohen's effect size of 0.48. 8 This finding was confirmed in another meta-analysis by Cramer et al. 9 A more recent meta-analysis by Zainal et al. suggests that the efficacy of MBSR in cancer patients lasts for a year. 32 MBSR is a structured 8-week group program, with each session lasting about 2.5 hours. 33 MBSR is different and much more intensive than 5 minutes of MB. The application of MBSR in the palliative setting is challenging. As mentioned in our previous pilot study, its application is limited by the intention and determination of terminally ill patients to break the long-standing habitual reactions to distressing experiences. Second, palliative cancer patients have a limited attention span. Finally, palliative patients are often too lethargic to participate in regular stress reduction sessions. 7
As a result, this 5-minute MB therapy was introduced to address the aforementioned challenges. This 5-minute MB therapy is an easy to administer therapeutic practice with rapid efficacy for terminally ill patients. From a variety of mini-mindfulness practices, MB was chosen for the study because it represents a core practice that serves to anchor the other mindful practices. 11 The efficacy in rapid reduction of distress using 5 minutes of MB in our previous pilot study 7 is replicated in this larger scale controlled trial. The rapid onset of effects of 5 minutes of MB could be explained by the fact that focused attention on breathing reduced the attention given to distressing experiences or thoughts. 7 In the current study, the results show that the reduction of distress lasted for 10 minutes after the therapy. In our pilot study, we have demonstrated that a subject's attention may return to focus on distress after the therapy has stopped. Therefore, after the initial guided practices, the patients are encouraged to have multiple self-practiced sessions of 5-minute MB to produce a more sustained effect. The effects of this 5-minute mindful therapy were measured using both a subjective self-rated assessment scale and physiological parameters.
From a physiological aspect, the sympathetic nervous system is activated when a human is under stress. Levels of circulating catecholamines (e.g., epinephrine, norepinephrine) are then increased. Blood flow to the heart, brain, and muscles is elevated, but blood vessels in the viscera and skin are constricted. The physiological parameters as indicators of increased catecholamine levels include blood pressure, heart rate, respiratory rate, and galvanic skin response. 21 Our current results demonstrated that blood pressure, breathing rate, pulse rate, and galvanic skin response reduced after 5 minutes of MB. It is consistent with studies that indicate a reduction of psychological distress leads to physiological changes, which include decreased cardiac output, blood pressure, and pulse rate. In addition to these common physiological parameters, we also measured the skin surface temperature and skin response in this study. Changes in hand or foot temperature are a reflection of peripheral blood flow—a measure of the stress response. A decrease in skin surface temperature indicates tension, in which individuals are experiencing nervousness, worry, or stress. Conversely, an increase in skin surface temperature indicates relaxation, in which individuals are in a peaceful emotional state. When individuals are stressed, their skin temperature will drop below 79°F, while when individuals are relaxed, their skin temperature will increase to more than 95°F. Dr. Lowenstein's ST SC911 was used to measure skin surface temperatures in this study. The ST SC911 is widely used in clinical research25–28 to identify stress levels and relaxation, as well as to see how cognition and emotion impact the human body. Skin response, also known as the galvanic skin response, is a measurement method based on bioelectrical properties of the skin. The present study used Mindfield eSense Skin Response Biofeedback System to record the galvanic skin response based on the activity of the perspiratory glands on the skin. 29 When individuals are stressed, the activity of the perspiratory glands will increase and vice versa.
Physiological measurements are indirect and nonsubjective indicators of psychological distress but can be influenced by many external factors such as the room temperature, effects of drugs, and medical conditions of the patients. In this study, the skin temperature increased after 5 minutes of MB, which was reflecting the constricting blood supply to the skin with lower perceived distress. However, skin temperature is the most sensitive physiological indicator toward the external factors. It is easily influenced by the environment and is easily changed according to the surrounding temperature. Overall, the current study demonstrated that there was rapid reduction of perceived distress after the 5-minute MB exercise in the palliative setting. The efficacy is indicated by the self-rating responses of the study subjects. The clinical efficacy is also demonstrated by the concurrent physiological changes.
There are several limitations in this study. The sample size of the current study was calculated based on the effect size of the reduction of distress in the previous pilot study. In a future study, a larger sample size is needed to illustrate the significant effect of 5 minutes of MB to the changes of physiological responses among the palliative cancer patients. Second, the current study aimed to examine the rapid and immediate effect of 5-minute MB. The sustainability of the effect was not examined. It requires a longer study period in the future. Furthermore, the presence of a staff member during the interventional sessions in the current study may have introduced attention as an intervening variable, which by itself has been shown to have significant effects on the psychological distress of the patients. This is especially dependent on the personality attributes of the staff member. In future studies, the instruction of 5 minutes of MB could be delivered in a practice session, before the actual testing sessions, so that the effects would be more purely a measure of the technique itself rather than the staff's impact. With limited funds, the current study was not able to afford to use the expensive instruments for the measurement of the physiological parameters. Future research could consider a better instrument to measure the galvanic skin responses such as Biopac MP36R with AcqKnowledge software. This instrument is specially designed for the use of psychological experiments and research. It has been used in previous clinical research.30,31 Finally, it is a single-centered study conducted in a university hospital setting. The application of the 5-minute MB in palliative care should be studied in other settings in the future.
Conclusion
At the end-stage of life, palliative care cancer patients experience a high level of distress. There is a need for a nonpharmacological or alternative therapy with rapid efficacy for the reduction of distress in this group of patients. Five-minute MB therapy is a simple, quick, and easy to practice therapeutic option. It produces a rapid reduction of perceived distress in terminally ill cancer patients. It also reduces the stress-related physiological responses in the patients. In view of the risk of recurrence of distress, it is advisable to have regular practice of 5-minute MB to achieve a sustainable reduction of perceived distress among the palliative cancer patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.