
Abstract
Abstract
Introduction:
Prior research has shown that advanced stage nonsmall cell lung cancer (NSCLC) patients enrolled in hospice care receive less aggressive treatment at the end of life (EOL) without compromising survival. Our purpose was to profile the continuum of care of these patients, exploring the connection between hospice enrollment and quality indicators for excellence in EOL cancer care.
Methods:
One hundred ninety-seven deceased stage IV NSCLC patients diagnosed between 2008 and 2010 at two separate tertiary care centers within the same county were identified. A retrospective review was conducted, collecting data from electronic medical records regarding antitumor treatment, postdiagnosis hospital visits and admissions, hospice referrals and enrollments, and circumstances surrounding the patient's death. Patients were grouped by their status of hospice enrollment, and the remainder of the measures compared accordingly.
Results:
There was no significant difference found in total number of postdiagnosis hospital admissions between the patients who were enrolled in hospice and those who were not. However, the group who received hospice services had a significantly lower number of hospitalizations (p < 0.001), emergency department visits (p < 0.01), and intensive care unit admissions in the last 30 days of life (p < 0.001). The number of lines of chemotherapy received did not differ significantly between the groups. Median survival, measured by the length of time between diagnosis and death, was significantly longer for hospice patients (p = 0.02).
Conclusions:
This study demonstrates that, among patients with metastatic NSCLC, hospice enrollment was associated with optimized EOL oncological care and a significantly longer median survival.
Introduction
L
Although palliative care and hospice services are often seen as “last resort” options that hasten death, recent studies have begun to offer alternative views. 4 It was first suggested in the landmark study by Temel et al. that the incorporation of early palliative care (defined as outpatient referral within eight weeks of diagnosis) in metastatic NSCLC patients not only improved quality of life but may have also extended survival. 5 Similarly, in the retrospective analysis performed by Connor et al., hospice enrollment for terminally ill patients with various cancers and congestive heart failure did not shorten survival. In fact, the subset of lung cancer patients referred to hospice survived an additional 39 days compared to their nonhospice counterparts (p < 0.0001). 6 Saito et al. also examined advanced stage NSCLC patients, concluding that hospice enrollment did not compromise their survival and that they received less aggressive end-of-life (EOL) care compared to nonhospice patients. 7
The ultimate goal of extending life in cancer care is expanding to include the comfort of the patient in the dying process. 8 New metrics have been designed to address this added aim in the field of oncology. As defined by the American Society of Clinical Oncology Quality Oncology Practice Initiative, high-quality treatment near death includes the following: no chemotherapy given within the last two weeks of life, a referral to hospice, and the enrollment in hospice care for more than one week before death. 9 Other studies have looked at additional markers, such as the number of postdiagnosis admissions to the emergency room, general ward, and intensive care unit (ICU), associating rising numbers with more aggressive and undesirable EOL care. There has been consistent evidence that EOL care is superior with the incorporation of hospice in terms of efficacy of pain management, preservation of patient dignity, and family satisfaction. 10 Our goal was to examine whether the emerging EOL measures are also superior with hospice care.
Methods
Study patients
Deceased patients with stage IV NSCLC diagnosed between January 2008 and January 2010 were identified at two tertiary medical centers within the same county. Patients were eligible for this study if they had pathologically confirmed stage IV NSCLC, were residents of the county in which the study took place, received care at either or both of the two study sites, and were deceased at the time of data collection. Exclusion criteria included pursuing treatment at an outside medical center, having a comorbid second malignant diagnosis for which the patient was receiving concurrent treatment, and those who were lost to follow-up (location of death unknown). Data collection was performed in two separate parts. The data for one tertiary medical center were gathered during the summer of 2012. The opportunity arose to repeat data collection at a second medical center, which was started in the fall of 2013 and completed by March 2014.
Study design and data collection
The electronic medical records of patients meeting inclusion criteria were retrospectively reviewed for basic demographic data in addition to data concerning hospital admissions (including emergency department [ED] visits, general hospitalizations, and ICU admissions), treatment regimens (including timing and lines of chemotherapy, radiation, and surgeries), palliative care consultations, hospice referrals, and location of death. We additionally reviewed the electronic medical records from the area hospice facility to obtain data concerning dates of hospice enrollment, any chemotherapy or radiation received while enrolled in hospice services, and location of death.
Patients were then divided into two primary study groups: those enrolled in hospice services and those who were never enrolled in hospice services. We compared these groups with regard to the following primary outcome measures: number of hospitalizations, ED visits, and ICU admissions in the last 30 days of life; new chemotherapy received in the last 30 days of life; any chemotherapy received in the last 14 days of life; and death in an acute care setting (including general hospital floor, ED, ICU, or acute palliative care unit within a hospital). These outcome measures were developed based on similar previous studies9,11–13 and the Quality Oncology Practice Initiative measures. 14 Secondary outcome measures included median survival, total lines of chemotherapy received, and the total number of hospital admissions following diagnosis.
Statistical analyses
Descriptive statistics were assessed for demographic variables using means and standard deviations for continuous measures and counts and percents for categorical measures. Comparisons between groups (nonhospice vs. hospice) were made using two-sample t tests for continuous measures and Fisher's exact tests for categorical variables. Median survival was compared between groups using a two-sample median test (using the SAS npar1way procedure with the MEDIAN option). Survival times were also compared using the Wilcoxon test and Kaplan–Meier estimator. For all analyses, SAS (version 9.3) was used.
Results
Patient characteristics
Demographic factors of age, sex, and race did not differ significantly between those patients who were enrolled in hospice and those who were not (Table 1). The majority of patients were white males, mean age 67–69 years old. For those patients enrolled in hospice, the mean length of enrollment was 48.9 days, with a range of enrollment durations from 1 to 396 days. Among patients in hospice, 84.2% of patients were in hospice for more than seven days.
EOL measures: Hospitalizations
Patients enrolled in hospice, on average, visited various departments of the hospital fewer times in the last 30 days of life than nonhospice enrolled patients (Table 2, Fig. 1). In the last 30 days of life, hospice patients had a lower mean number of hospitalizations (0.44 hospice vs. 0.84 nonhospice; p = 0.0003), fewer ED visits (0.36 hospice vs. 0.67 nonhospice; p = 0.0062), and fewer ICU admissions (0.0086 hospice vs. 0.16 nonhospice; p = 0.0004). However, the two groups were similar in the total number of hospital admissions following the cancer diagnoses (1.48 hospice vs. 1.78 nonhospice; p = 0.24).
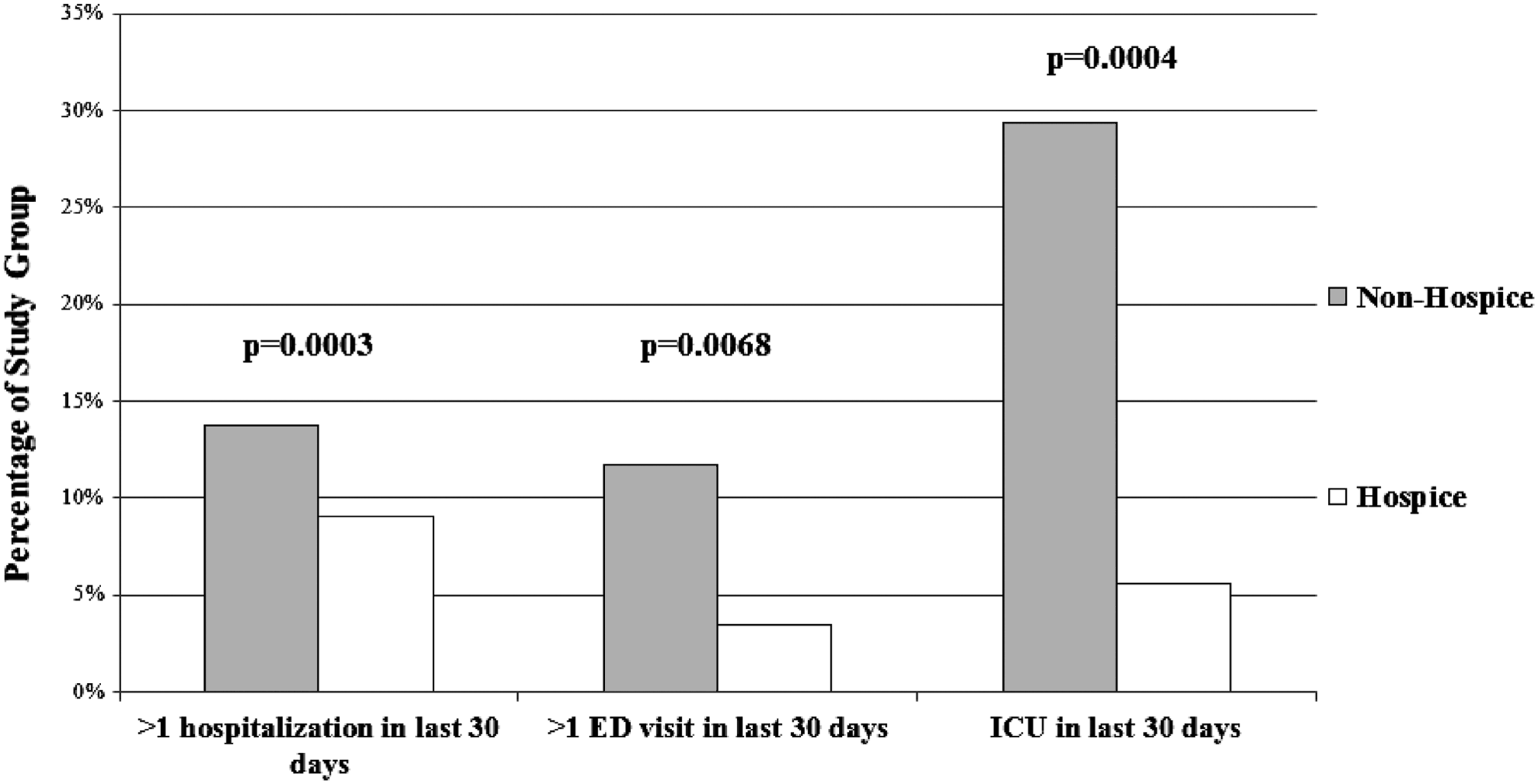
Comparison of the percentages from each study group (nonhospice and hospice) that had greater than one hospitalization, greater than one ED visit, and any ICU admissions in the last 30 days of life. p-Values denoted. ED, emergency department; ICU, intensive care unit.
Denotes significant p-value.
ED, emergency department; ICU, intensive care unit.
Timing of chemotherapy administration
Fewer patients enrolled in hospice were administered a new chemotherapeutic agent in the last 30 days of life (3.47% hospice v 11.76% nonhospice; p = 0.038). In addition, a lower percentage of patients enrolled in hospice received any chemotherapy in the last 14 days of life (1.39% hospice vs. 13.73% nonhospice; p = 0.0014, Fig. 2). However, the groups were similar in the average number of overall lines of chemotherapy they received from the time of diagnosis (0.92 lines for hospice patients, 0.93 lines for nonhospice patients; p = 0.96). In the entire studied population, patients received a range of zero to five lines of chemotherapy from the time of diagnosis until death.
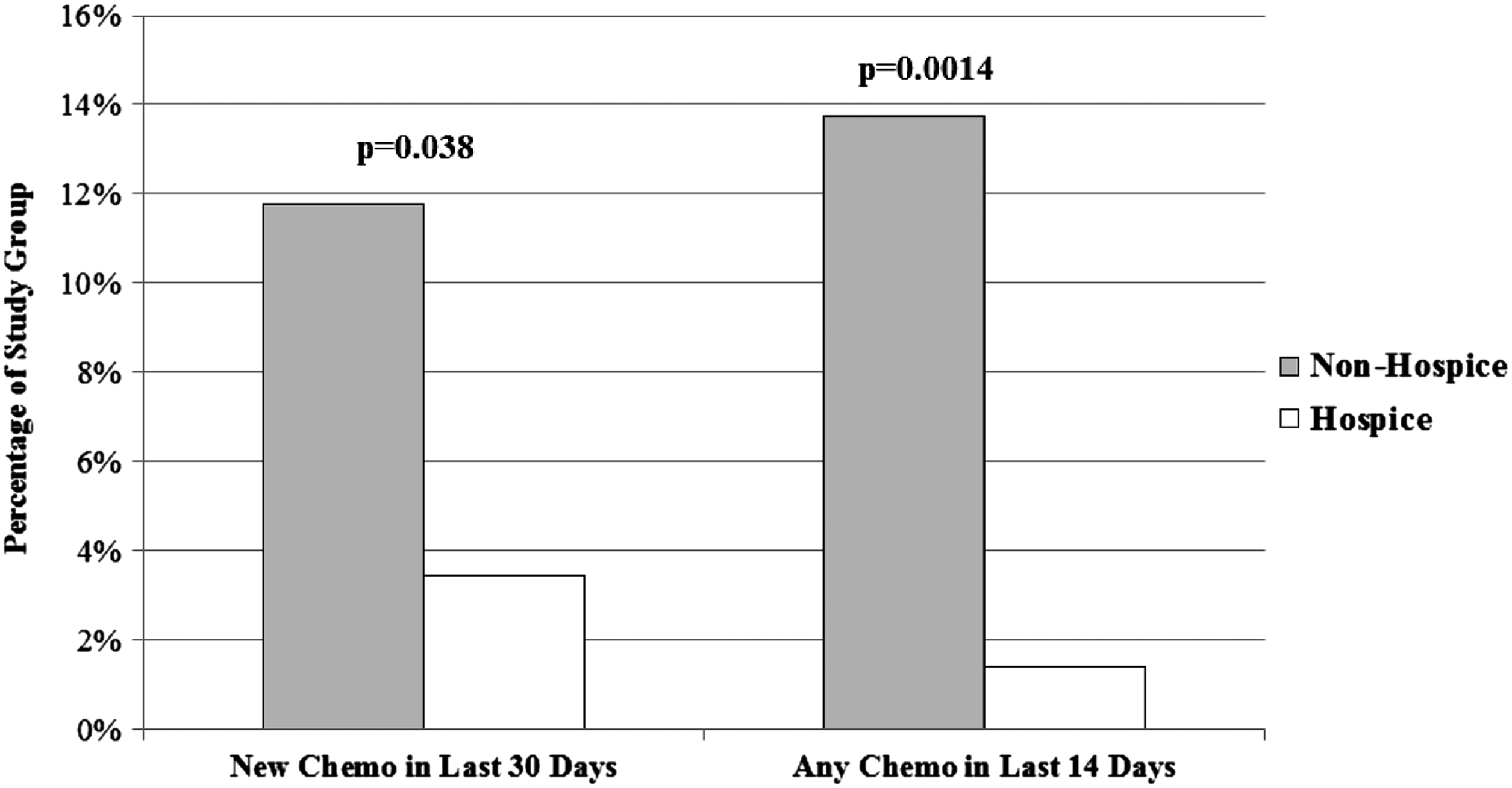
Comparison of the percentages of patients from each study group (nonhospice and hospice) who received a new chemotherapeutic agent in the last 30 days of life or any chemotherapy in the last 14 days of life. p-Values denoted.
Location of death
We defined death in an acute care setting as death occurring in a general hospital floor, ED, ICU, or acute palliative care unit housed within a hospital. Patients who were not enrolled in hospice services died in an acute care setting significantly more often than hospice enrolled patients (p < 0.0001). Patients enrolled in hospice were more likely to die at home, in an inpatient hospice facility, or in a nursing home (Fig. 3).

Location of death for nonhospice and hospice patients. Nonhospice patients were significantly more likely to die in an acute care setting (general hospital floor, ED, ICU, or palliative care unit; p = 7.6 × 10−23).
Palliative care consultation
Twenty-eight percent of the study population received a palliative care consultation. There was no significant difference in the rate of consultation between the hospice and nonhospice groups. Early palliative care was rarely evidenced, as the vast majority of the consults occurred in the inpatient setting within three weeks of the patient's death.
Survival
Median survival was found to be significantly higher in the group of hospice patients. Median survival was 87 days in the nonhospice group and 145.5 days for the hospice group (p = 0.02) (Fig. 4). When a Kaplan–Meier estimate is used, a higher survival probability is clearly demonstrated in the hospice group up to one year after diagnosis (Fig. 5). Mean survival did not differ between the two groups and was 179.8 days for the nonhospice group and 225.4 days for the hospice group (p = 0.22).

Median survival for nonhospice and hospice patients. Hospice patients had a longer median survival than nonhospice patients (p = 0.0166).

Product limit survival estimates. The survival plot demonstrates a clear separation of the curves, with the hospice patients having a higher survival probability than nonhospice patients up to one year after diagnosis.
Discussion
Nearly three quarters of the patients in our study enrolled in hospice services, which demonstrates a shift in the utilization of hospice care among this population, as previous studies show enrollment rates of at best 50% of their patients.15,16 Moreover, the majority (84.2%) of the hospice patients had a length of stay greater than one week. We are encouraged by this transition in care as the patients who received hospice services were found to have less intense EOL care in contrast to their nonhospice enrolled counterparts, according to the measures articulated by the Quality Oncology Practice Initiative and other studies. Although the total number of hospital admissions after diagnosis was similar between both groups, hospice patients had significantly fewer hospitalizations, ED visits, and ICU admissions in the last month of life, demonstrating a more optimal EOL time course.
In a similar trend, the two study groups did not differ in the number of lines of chemotherapy received from the time of diagnosis. Significantly fewer hospice-enrolled patients received a new chemotherapeutic agent in the last month of life as well as any chemotherapy in the final two weeks of life. This is not unexpected, as most insurance companies, including Medicare and Medicaid, do not cover the expense of chemotherapy for hospice-enrolled patients. Note, however, that chemotherapy is almost never used for curative intent in this population, given the nature of the disease. In this study, there were several instances of palliative radiation given during hospice, in contrast to no occurrences of palliative chemotherapy within hospice.
The location of death was examined and found to differ significantly between the two groups. Patients not enrolled in hospice were significantly more likely to die in an acute care facility (general hospital, ED, ICU, or acute palliative care unit housed within a general hospital). Patients who die in these acute care settings often experience greater distress and poorer quality of life than those who pass away in their homes. 17 A benefit of hospice services includes access to another inpatient alternative, which is able to provide a high level of supervision and skilled nursing care often required at the EOL, but in a less severe and intimidating environment for the patient, their family, and caregivers. Death of a loved one in the hospital has also been found to place caregivers at greater risk for the development of psychiatric illness. 18
Despite increased utilization of hospice services in our population compared to prior studies, it is interesting to note this in relation to the low rate of palliative care consultation (28%) and the absence of early palliative care. This contrast is thought provoking, but certainly does not argue against the utility of early palliative care referral. There are likely multiple factors contributing to these findings and may include the lack of organized infrastructure within these two study sites for palliative care, reflective of clinical practice before the Temel study in 2010. 5 In addition, increased use of advanced directives and Physician Orders for Life Sustaining Treatment-type forms may put clinicians more at ease about recommending hospice services themselves, given the patient's original wishes. One must also consider the subjective experience of the transition to hospice care, which was not captured in our study. In discussing and establishing goals of care soon after diagnosis, early palliative care plays a much-needed role in the mental, emotional, and spiritual aspects of the eventual transition to hospice.
Hospice services are commonly perceived to hasten death. Our study supports the findings of those previous, which showed that stage IV NSCLC patients enrolled in hospice services had a significantly longer median survival than their nonhospice counterparts. Moreover, they also received optimized EOL oncological care, as demonstrated by less aggressive chemotherapeutic approaches at the EOL and fewer visits and admissions to the hospital within the last month of life, which is theorized to be one of the potential mechanisms of their longer survival. 19 It is also proposed that hospice services provide better monitoring, palliative treatment, and increased social support, factors which have individually been associated with improved survival. 19
There are some significant limitations to the method and analysis of this study. As seen with many retrospective studies, we were limited by the amount and type of information available through the various electronic health records. Uniformly documented baseline characteristics were limited to age, race, and gender. Characteristics such as socioeconomic status, insurance status, and religion were only sparsely recorded. Performance status indicators, such as the Karnofsky or Eastern Cooperative Oncology Group scores, were not consistently recorded throughout the patient population and therefore were not utilized as a baseline demographic. We recognize the importance of these factors, as they may be major contributors to the approach to chemotherapeutic treatment as well as the patient's decision to enroll in hospice care. Our inability to control for these confounders significantly limits the degree to which we can attribute our findings to the hospice intervention alone. We also acknowledge the innate selection bias that exists in the population choosing hospice versus declining hospice. The correlation seen in our study between hospice and less aggressive EOL care could be largely due to the views, personalities, and priorities of the patients choosing it, rather than the role of hospice itself.
Finally, further work is needed to explore the optimal length of stay in hospice and the role that earlier palliative care referral plays in that transition of care. As previously referenced, between the years of 2008 and 2010, from which the data of this study are gathered, there were no formally structured palliative care programs available for newly diagnosed metastatic NSCLC patients. Since that time, palliative care has and continues to evolve at the study institutions and data are already being gathered in the wake of this development. We aim to continue studying the relationship and impact between the evolving role of early outpatient palliative care in the oncological setting and the subsequent transition to hospice services. The results of this study add to the growing body of evidence supporting the utility and benefits of hospice services in the care of stage IV NSCLC patients, without incurring a lower survival rate.
Footnotes
Funding Information
This work received NCI funding support (NCI P30 CA012197 Boris Pasche PI).
Author Disclosure Statement
No competing financial interests exist.