
Abstract
Abstract
Background:
Alternative locations for children near end of life (EOL) are lacking in the United States with deaths largely occurring within intensive care units (ICUs). The reflection room (RR) was implemented as a relevant space for providing this care in our hospital.
Objective:
We hypothesized staff would report a positive experience in providing EOL and/or postmortem (PM) care here and would recommend this to peers.
Design:
This explorative study summarized room use data and evaluated staff experiences using a voluntary qualitative and quantitative survey.
Subjects:
The survey was administered to the inpatient interdisciplinary team.
Results:
From 2011 to 2014, 116 children used the RR, 64% for PM care, and 34% for EOL care. A total of 201 staff responded to the survey. Of them, 90% described the space as a valuable resource to families, 90% reported a preference for using this location versus a hospital unit, and 93% stated they would encourage their peers to do the same. Advantages listed were increased privacy, allowance for more visitors, and a quieter, calmer environment. Challenges included distance from the unit of transfer, managing assignments in two hospital locations, and medication transportation. Overall, there was a measureable decrease in the number of deaths pronounced in the ICU as the number pronounced in the RR increased, illustrating a significant change in practice.
Conclusion:
This study demonstrated an overwhelmingly positive experience in providing EOL and/or PM care to children in the RR and staff would recommend this to peers. This model of care should be a serious consideration for hospitals in the United States.
Introduction
I
Families and professional caregivers are, therefore, faced with the ongoing reality of children continuing to die in the hospital. To address this, our hospital, UCSF Benioff Children's Hospital Oakland, implemented a palliative care consult program in 2011 that embedded an alternative homelike location, called the reflection room (RR), for EOL care, with donor funding. Our hospital serves more than 73,000 children per year, is Northern California's only Level 1 pediatric trauma center, and experiences on average 66 deaths per year. A series of small offices adjacent to the primary palliative care offices were converted to a family suite with a designated bedroom, living room, kitchenette, and children's play area (Fig. 1).

Reflection room bedroom/living room.
The goal of the RR was to provide an alternative location for EOL care for the last 8–12 hours of life and for up to 24 hours of postmortem (PM) care. Families are given the choice by the medical team whether they would like to use the RR, but can choose to stay in their assigned hospital room with their child if preferred. The time frame of 8–12 hours for EOL care was chosen so as not burden the medical team, who transfers to the RR with the child, away from the original unit/ward of care. This use of the RR heralded a significant change in practice for providers at our hospital.
The RR aimed to bring a homelike environment to the hospital with minimal medical technology, allowing more space for families to feel comfortable to participate in and maintain cultural and religious traditions while keeping the child's inpatient status. For example, cultural traditions for premortem and PM bathing and dressing require the presence of several family members in attendance. This is aided by the child not having multiple monitoring devices and catheters in place. The palliative care team is available for additional support and anticipatory guidance for providers, the child, and their family. After hours, support is garnered from the nursing supervisor and social worker on call. Patient care staffing remains the same, incurring no additional costs.
Objectives
The purpose of this explorative study was two pronged: (a) to analyze the data collected about the patients who used the RR and (b) to obtain feedback from providers who gave care to patients in the RR because of a change in practice. This was the initial part of a more comprehensive review of the impact of the RR on family experiences whose child used the room. The overall goal was to demonstrate whether this new model of care can be a serious consideration for other hospitals that care for children at EOL. For this initial portion of study, we hypothesized the following:
(1) Providers would report an overall positive experience in providing imminent EOL or PM care to children and their families in the RR. (2) Providers would recommend use of the RR to peers instead of EOL or PM care occurring on the primary unit.
Materials and Methods
Approval was obtained from the IRB at UCSF Benioff Children's Hospital Oakland. Demographics for use of the RR were extracted from the existing palliative care database and compiled into a summary comparative database (EXCEL) by our research assistant (Y.W.). Palliative care patient characteristics were categorized into four broad groups, as defined by ACT and RCPCH (Association for Children's Palliative Care and Royal College of Paediatrics and Child Health). 5 Group 1 encompasses life-threatening conditions in which curative treatment is possible but may fail, for example, cancer and cardiac disorders; Group 2 encompasses conditions in which life can be prolonged with periods of intensive treatment but early death is likely, for example, cystic fibrosis and muscular dystrophy; Group 3 includes progressive conditions in which there is no curative treatment and care is primarily palliative, for example, trisomies 13 and 18 and mucopolysaccharidosis; Group 4 encompasses conditions with extensive neurological disability and associated sequelae, whereby patients may decline unpredictably, for example, complicated cerebral palsy and brain injuries.
A quantitative and qualitative survey was developed based on the four components of the model of reflection for children's palliative care: the preliminary, deductive, inductive, and postreflection phases.5,7 This model specifically deals with debriefing opportunities for healthcare providers working with EOL circumstances and is integral to evaluating provider experiences with the RR. Our survey assessed the impact of a change in location of care of patients at EOL or PM from the usual location within the hospital (e.g., pediatric ICU (PICU), neonatal ICU (NICU), emergency department (ED), and acute care wards) to that of the RR on a different hospital floor.
The preliminary phase of the survey (questions 1–6) aimed to gather demographics of inpatient providers such as professional capacity, length, and clinical area of experience. The format of multiple choice and directed answers was used, the latter applying a 5-point Likert scale (with responses ranging from strongly agree to strongly disagree). The deductive phase (Part 1, questions 7–11) assessed provider knowledge of the RR, regardless of use. Part 2 (questions 12–16) was specifically for providers who had used the RR and evaluated the logistical effectiveness of the practical components involved in transferring a patient and family to the RR. The inductive phase (questions 17–21) used open-ended questions to give providers a chance to describe advantages and barriers to using the RR as well as suggestions for increased use of the room. The postreflection phase (questions 22–23) aimed to assess whether providers who had used the RR would continue to do so in the future and encourage their peers to consider the same practice. Participants were given the opportunity at the end to share additional comments.
The survey was piloted with selected providers with extensive experience in providing EOL care to children at the hospital. After feedback was incorporated, the survey (utilizing Survey Monkey www.surveymonkey.com) was sent to all providers (n = 912) working with children and families in the inpatient setting, including physician assistants, nurse practitioners, clinical nurse specialists, respiratory therapists, social workers, registered nurses, and physicians including fellows and residents. Participation was voluntary and the survey was emailed twice, four weeks apart. The results were summarized descriptively. Spearman correlations were applied to ordinal variables to test whether provider experience at the hospital (length of employment) and prior use of the RR were associated with likelihood of recommending the RR (either as a valuable resource and/or for future use).
Results
RR demographics
Since its inception in June 2011 through 2014, a total of 116 patients and their families have used the RR, 62% (n = 72) for PM care and 33% (n = 38) for EOL care. Figure 2 describes the locations that EOL care occurred (PICU/NICU, non-ICU, RR). Since inception, up to 23% of all EOL care occurred in the RR with a progressive decrease in EOL occurring in the ICUs. Other unique uses of the RR (n = 6, 5%) have included religious ceremonies or other celebrations of life such as birthday parties. The average length of time that families chose to stay in the room was 9 hours (64%), although 19% chose to stay for more than 19 hours. Patients (82%) were largely transferred from the ICUs (Fig. 3), reflecting literature citing these as the predominant location of death for children in the United States.1–4 The largest age group of patients to use the room was infants (<1 year) at 64%. Specifically, 34% of the total cohort were neonates (newborn–1 month), consistent with national death statistics (Fig. 4).4,8
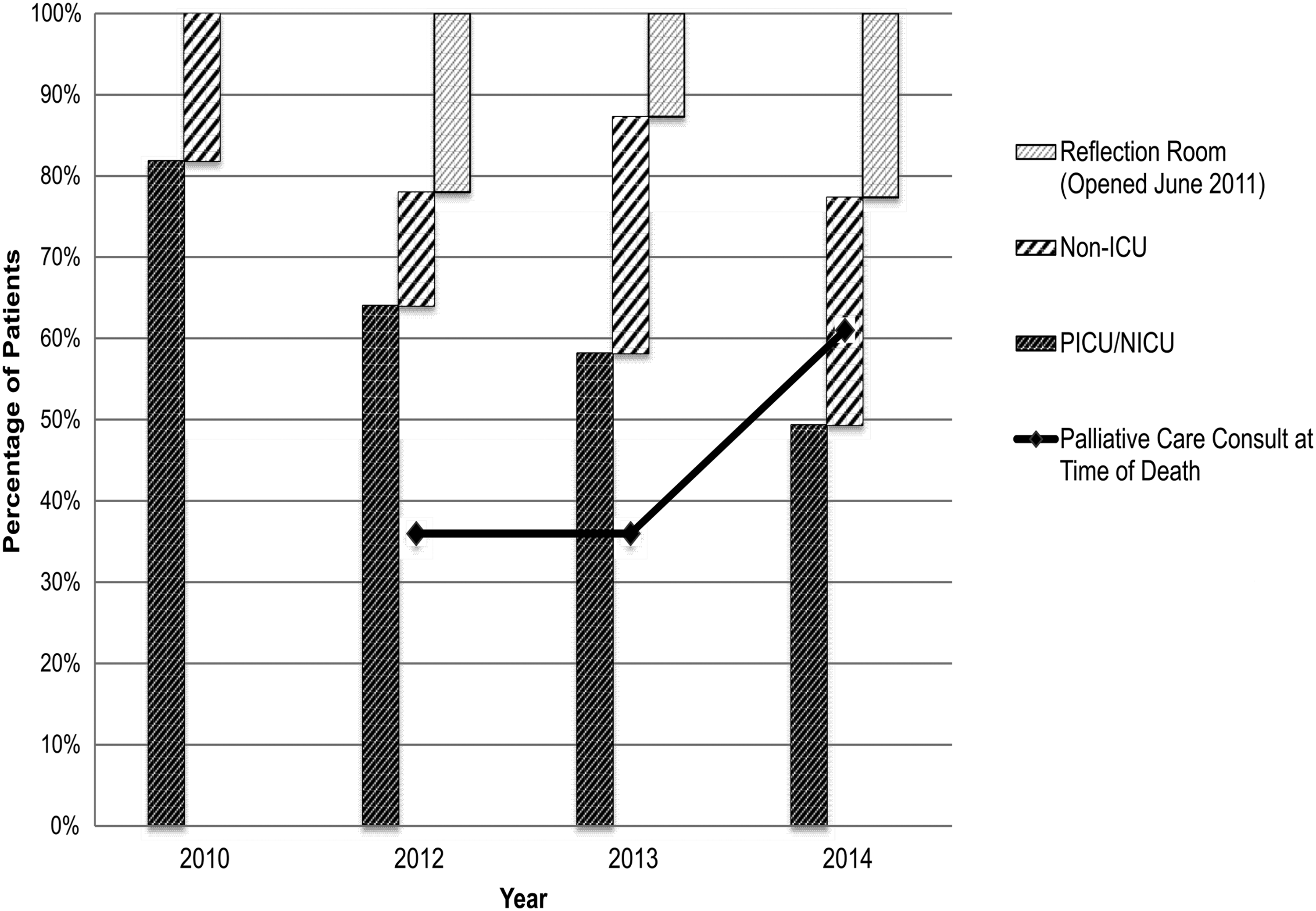
Location of end-of-life care at UCSF Benioff Children's Hospital Oakland per hospital area: 2010, 2012–2014.

Cumulative number of patients transferred from hospital unit to reflection room, 2011–2014.
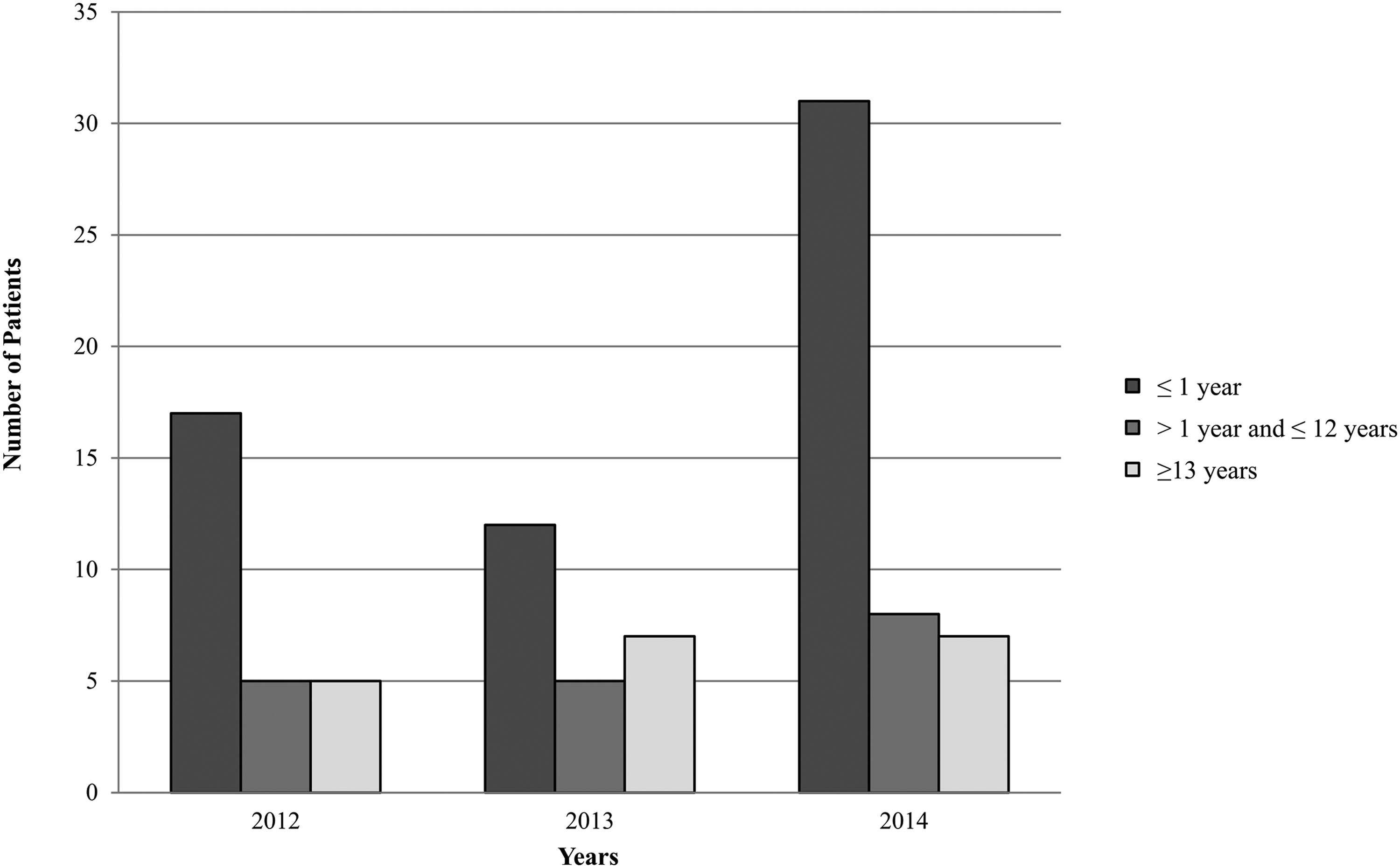
Number of patients utilizing reflection room per age group by year.
Table 1 describes the diagnostic categories of patients using the RR. The largest ACT/RCPH category (63%) included those with life-threatening illnesses. The remainder of patients fell evenly into categories 2, 3, and 4, reflecting life-limiting, incurable illnesses.
ACT and RCPCH, Association for Children's Palliative Care and Royal College of Paediatrics and Child Health.
Survey results
A total of 201 (22%) hospital providers responded. Results are reported in the context of the model of reflection for children's palliative care.5,6
Preliminary phase
Respondents represented a broad selection of healthcare providers (Fig. 5) with the overwhelming majority having more than five years experience (14% 5–10 years, 12% 10–15 years, 47%> 15 years). Interestingly, most respondents worked primarily in the ICUs (27% PICU and 37% NICU) with the remainder across oncology (11%), acute care (13%), subspecialty teams (9%), and the ED (3%). In addition, the majority of respondents had cared for a child at EOL multiple times (56%> 10 times, 20% 5–10 times, and 9% 3–5 times). Although most respondents (65%) agreed that the optimal location for EOL and/or PM care for children should be their own home (with 26% choosing a community inpatient palliative care center), the vast majority (90%) supported a preference for use of the RR rather than the hospital unit (71% strongly agree and 19% agree).
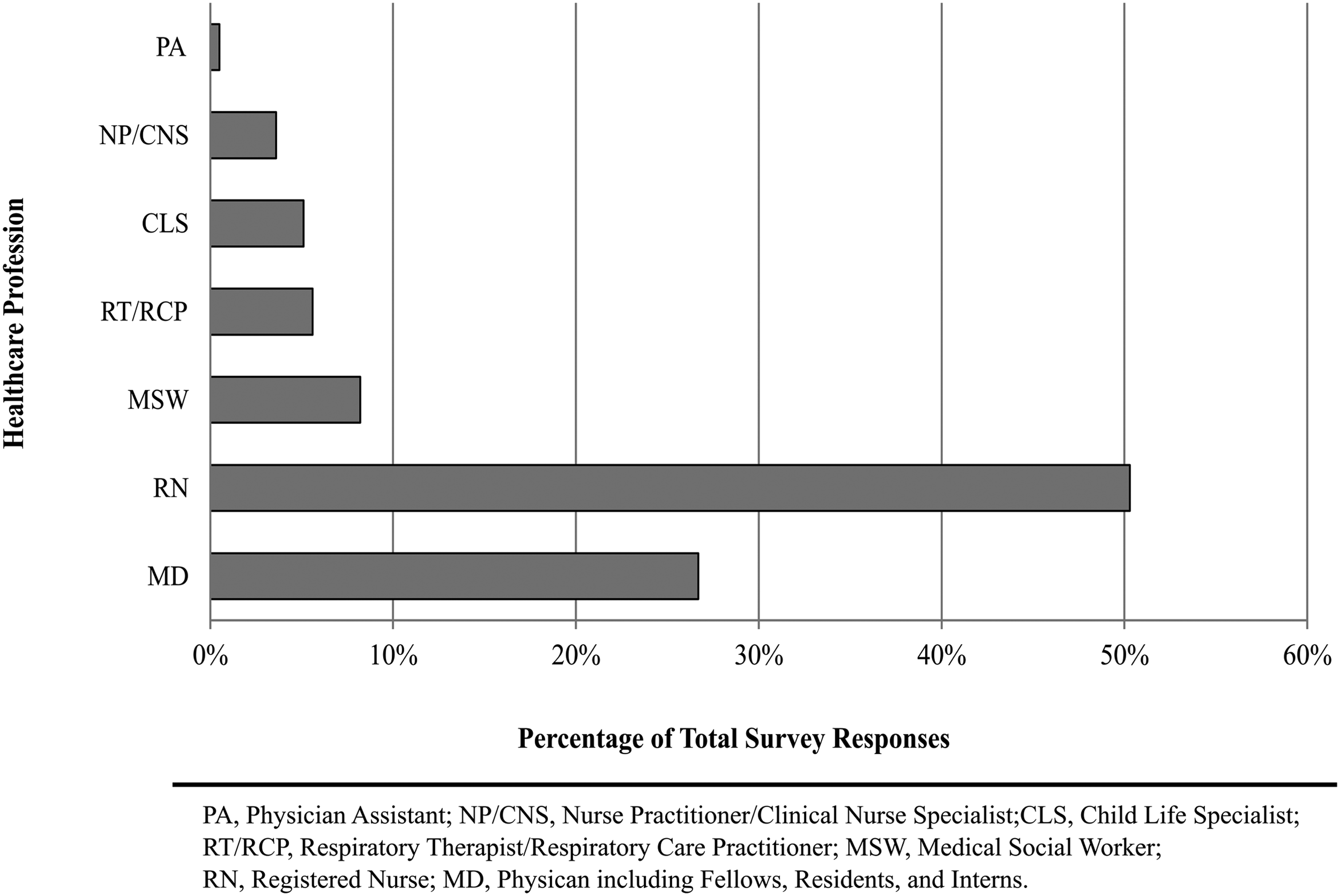
Percentage of total survey responses by healthcare profession.
Most respondents (86%) agreed that the main purpose of the RR was for imminent EOL and PM care. Despite most respondents knowing about the existence of the RR with hospital-wide announcements and open houses, ∼35% felt that they had an inadequate introduction to the use of the room, and 23% never had the opportunity to use it first hand in an EOL experience.
Deductive phase: All respondents
Most respondents (90%), regardless of personal use of the RR with a patient, reported that the RR was a valuable resource to families (76% strongly agree; 14% agree) and 92% reported that families appreciated the RR because it enhanced family-centered care at EOL (75% strongly agree; 17% agree). Fewer respondents (48% strongly agree; 17% agree) stated that they had suggested use of the RR to families.
Deductive phase: Respondents reporting previous use of RR
Providers who had used the RR described the logistical effectiveness of the clinical management of their patient. Most reported that the transfer of their patient was manageable as was providing overall support to, and meeting the needs of, the child and family (Table 2). However, some respondents (44% neutral to strongly disagree) indicate challenges with providing adequate pain and symptom management and in managing a two-patient assignment in different locations (62% neutral to strongly disagree).
Inductive phase
Respondents reported that their perception of RR use had improved after using it first hand (22% positive; 33% more positive). No respondents declared a negative perception. The most frequently reported advantages to RR use were improved family privacy (71%), increased visitors allowed (38%), and creation of a quiet and calm environment (31%). Others included increased physical space compared with the ICU, a more comfortable, homelike, nonmedical setting, and increased time for the family to be with their child after death. Comments included the following:
The family is allowed to orchestrate the final moments and I felt more able to step away and give them privacy. The comfort of the family is more possible.
The top three barriers listed were distance from the unit of transfer (28%), staffing ratio concerns, that is, management of a two-patient assignment in different locations (27%), and difficulty with the transport of medications (10%). The RR was created from renovated office space, therefore, lacking amenities helpful for patient care such as no bathroom, narrower doorways, and suboptimal staff access because of the allowable number of visitors. Hence, respondents also requested increasing the room size to allow better patient access (22%), having a sink and running water (15%), and a bigger bed for communal sleeping (6%). Family comfort was key in following suggestions:
Anything that allows family members to be in the room with the patient. Maybe a sliding door that can allow a bigger area if family wants everyone in the patient's room.
Respondents proposed other ways to increase room use, for example, offering use more frequently and earlier (18%), use as a waiting room for families whose child is at EOL in the hospital (8%), and to increase education about the room (8%):
…the more that staff nurses and inpatient doctors know about the benefits of allowing families to make beautiful memories at the time of their child's death and the benefits of that shared experience for their family members, the more people will support and facilitate its use.
Postreflection phase
Of the respondents who had directly cared for a child and family in the RR, 90% stated that they would prefer to use the RR for EOL and PM care rather than the hospital unit (71% strongly agree; 19% agree). In addition, 93% overwhelmingly supported that they would encourage their peers to do the same (74% strongly agree; 19% agree).
Correlations and other findings
As expected, we found a positive correlation between length of employment at our hospital and consideration of the RR as a valuable resource (ρ = 0.162, p = 0.028), as important to families (ρ = 0.128, p = 0.083) and likelihood of suggesting use to peers (ρ = 0.136, p = 0.066). The correlations were even more robust, and statistically significant, for those who had used the RR and experienced EOL processes there first hand and likelihood of suggesting use (ρ = 0.443), as important to families (ρ = 0.284) and as a valuable resource (ρ = 0.246)—all p < 0.001.
Discussion
Suggestions for a private home-like space for EOL care are documented8–11 and use of a “cold bedroom” (or special room kept at <50F to slow physical deterioration after death) in British inpatient palliative care centers are reported as having a positive impact for families. 12 Importantly, research has recognized the value of allowing families extended time with their child after death, positively impacting grief and bereavement. 1
Our research has shown the RR to be a viable, alternative model of care. Our primary results demonstrate how use of the RR allowed for a better patient care experience away from an intensive-type environment. Providers identified improved family privacy, increased visitor allowance, and a peaceful environment as the top benefits of the RR. The major disadvantages remain primarily logistic: feeling distant from the unit of transfer, challenging to manage patient assignments in two locations, and cumbersome transportation of medicines necessary for symptom management. Despite these concerns, our results still support the hypothesis that providers would report a positive experience in providing EOL and PM care to children and their families in the RR and, in turn, would recommend this venue to peers. The study's strengths include the number of respondents (>200), the variety of providers who responded (Fig. 5), and their depth of clinical expertise.
The results reflect an increased comfort of providers introducing this location to families coupled with an increased familiarity and practice with managing EOL care and grief in a different location. Involvement of the palliative care team for family and/or provider support may have contributed to this increased comfort. However, ongoing education regarding room purpose and use remains a priority. Familiarity with RR use was a key driver impacting providers' likelihood of suggesting the RR to peers and patients alike. Indeed, our statistical analysis supports a “seeing is believing” aspect to the RR, with the need to have providers experience this space first hand.
Multiple benefits exist. The child and family continue to receive care and support from their original care team, enhancing familiarity and consistency of care, even under extenuating circumstances. For example, Federal and State laws require certain cases to be referred to the medical examiner (ME), for example, suspected nonaccidental trauma or medicolegal concerns. If ME permission is obtained, the RR can give families much needed time and support previously not possible. When a critically ill newborn is emergently transferred before the mother has been discharged from the hospital of birth, transfer of the mother can occur, as ongoing maternal recovery is possible because of the “rooming in” nature of the bedroom. Or, if a child experiences sudden death in surgery, more prolonged psychosocial and grief support can be offered to the family. Families can also receive assistance with funeral planning, allowing the body to be retrieved directly from the RR.
Other proposed benefits include the gift of time to families, including time to:
(a) spend one last night with their child, even PM; (b) take their child outside a hospital room as many have had prolonged hospitalizations or never been home at all; (c) give the child their last bath; and (d) say the impossible goodbye.
One final consideration is the location of the RR at our hospital, which is on a floor different from the ICU/ED/pharmacy. Future RR type design should consider room size, physical access to the patient, and nearness to the ICU/ED/pharmacy. The largest study limitation was the lack of a validated survey tool. Although our survey yielded 201 respondents, there may have been selection bias, whereby only providers interested in EOL or PM care responded as indicated by responses largely from ICU staff (64% of responses) and an 80% use of the RR by ICU patients. Furthermore, our survey was limited to providers and not families themselves.
Conclusion
This study demonstrates how hospitals could consider establishing an alternative location for EOL and PM care such as the RR. We conclude that a private inpatient EOL and PM care location, such as the RR, can improve provider experiences around these exceedingly stressful times. Future research includes plans to evaluate family responses to the RR and to validate our findings in other hospitals. It is hoped that having a space like the RR will create a culture of increased compassion and care from providers, as well as more positive memories for families who experience the death of their child.
Footnotes
Author Disclosure Statement
No competing financial interests exist.