
Abstract
Abstract
Background:
Opioids are the mainstay of pain control for patients with chronic pain. Often, opioids with reported active metabolites, such as morphine and hydromorphone, are thought to increase the risk of neurotoxicity in renal impairment.
Objectives:
To identify and assess the quality of evidence for neurotoxic effects in patients with renal impairment receiving morphine or hydromorphone.
Methods:
Systematic searches were conducted of the following databases from inception to December 2015: MEDLINE, CINAHL, EMBASE, in addition to hand-searching relevant review articles’ citations. Studies were included if they reported neurotoxic effects of either morphine or hydromorphone for chronic or malignant pain in patients with renal impairment. Review articles and case reports were excluded. Narrative review was undertaken. The Grading of Recommendations, Assessment, Development and Evaluation approach was used to assess study quality.
Results:
Six original articles, three prospective and three retrospective studies were identified and assessed. No relevant randomized clinical trials were identified.
Conclusions:
Although morphine and hydromorphone use may be associated with neurotoxic effects in patients with renal impairment, current evidence consists of very low-quality studies with conflicting findings. Clinicians may consider using either morphine or hydromorphone in mild-to-moderate renal impairment, while closely monitoring for neurotoxic effects, particularly when used in high doses and for extended duration.
Introduction
S
The risk of these potentially distressing symptoms may be increased by renal impairment, commonly seen but underrecognized. One study showed that almost 20% of cancer patients have a creatinine clearance of less than 60 mL/min, four times the prevalence in the general population. 2 In addition, patients with chronic kidney disease (CKD) often have chronic pain, placing them at high risk of developing neurotoxicity.3,4
Morphine and hydromorphone, two commonly used opioids, are known to have active metabolites, which may accumulate in renal impairment and potentially cause neurotoxicity. 5
Morphine-3-glucuronide (M3G) and morphine-6-glucuronide (M6G) are the major metabolites of morphine. 6 Lacking opioid receptor affinity, M3G has no analgesic activity. Rodent model studies suggest M3G causes neuroexcitatory effects of hyperalgesia, allodynia, myoclonus, and seizures. 5 However, similar studies of morphine use in patients have been limited primarily to case reports.7,8
Hydromorphone, a semisynthetic derivative of morphine, is primarily metabolized to hydromorphone-3-glucuronide (H3G). Similar to M3G, H3G lacks an analgesic effect but may cause dose-dependent myoclonus, agitation, and seizures in rats. 9 Despite these findings, evidence in humans is conflicting. In a case study, one patient with CKD did not display neurotoxic effects despite having an H3G level 4 times as high as patients with normal renal function. 10 In clinical practice, hydromorphone often is used preferentially over morphine in patients with renal impairment.11,12 However, as hydromorphone use becomes more common, case reports show potential association of its use in renal impairment with development of neuroexcitatory symptoms, such as hyperalgesia, myoclonus, and seizures.13–15
We conducted a systematic review examining the association between either morphine or hydromorphone use in renal impairment and development of subsequent neurotoxicity.
Methods
We conducted this systematic review by searching electronic databases and relevant literature.
Eligibility
We included studies assessing a neurotoxic symptom in patients treated for chronic cancer or noncancer pain with morphine or hydromorphone. Neurotoxic effects were defined broadly as cognitive dysfunction, delirium, agitation, hallucinations, hyperalgesia, allodynia, myoclonus, tremor, or seizures. Relevant studies needed to assess renal dysfunction in some manner (e.g., serum blood urea nitrogen [BUN], serum creatinine, and glomerular filtration rate [GFR]). Renal impairment was specified as renal impairment, kidney disease, kidney failure, or renal failure. Exclusion criteria included non-English studies, review articles, and case reports.
Search strategy
The following databases were systematically searched from inception through December 2015: PubMed, CINAHL, and EMBASE. The reference lists of relevant screened articles were also searched. Search strategies, including MESH terms and free text keywords, are detailed in Table 1.
BUN, blood urea nitrogen.
Data collection and analysis
The titles and abstracts of identified references were screened. Duplicates were removed from the reference library using the EndNote program. If it was unclear whether screened studies fulfilled the review's inclusion criteria, full-text articles were reviewed.
Included studies were independently assessed for quality. Predefined data collection forms were used for data extraction.
Publication details, interventions, study duration, outcome measures, and information relevant to trial quality were determined from each included study. Two reviewers independently performed the reference screening process and reached consensus regarding the included studies. Results are presented as a narrative analysis.
Quality assessment
The assessment of included studies was performed by using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, 16 a widely utilized, proven, and comprehensive method to rate the quality of evidence.
Results
Our electronic database search obtained 1368 references with 4 additional references from reference lists’ searching. Thirteen full-text articles were obtained for further analysis and six met inclusion criteria. The included articles were all observational studies with hospice or palliative care patient populations and three prospective17–19 and three retrospective20–22 studies. Three studies addressed morphine-induced neurotoxicity17,18,20 and three addressed hydromorphone-induced neurotoxicity.19,21,22 No randomized controlled trials were found. The preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart details our study screening process in Figure 1.
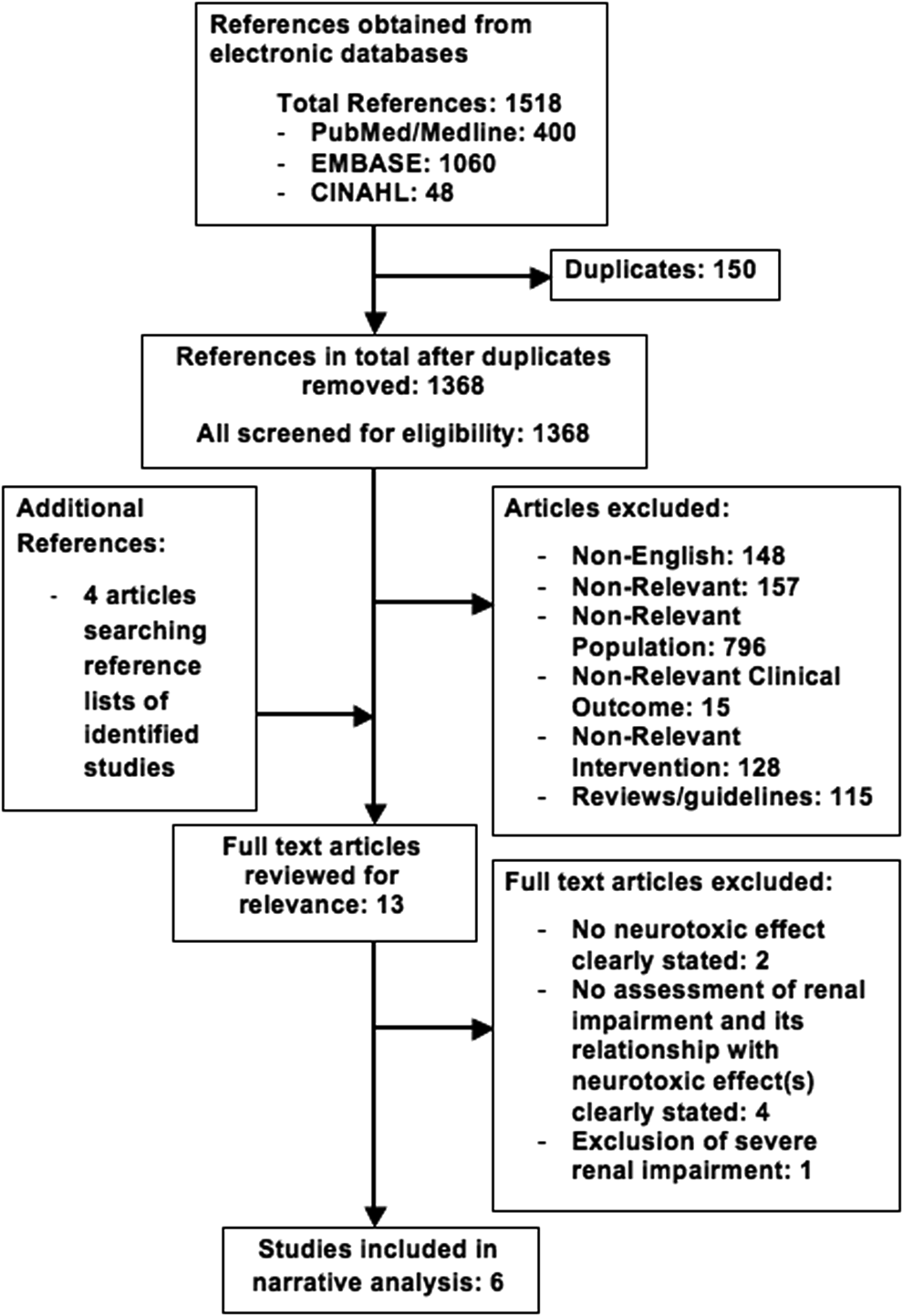
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram.
Of those screened articles further analyzed, two studies23,24 were excluded due to lack of reporting neurotoxicity directly related to renal impairment, although renal function was assessed. Four other excluded studies25–28 did not assess a specific neurotoxic effect. Finally, although one study investigated the association of morphine use with neurotoxic effects and measured renal function, it did not evaluate patients with significant renal impairment. 29 Included studies are described further in Tables 2 and 3.
AE, adverse effects; CG, Cockcroft–Gault; CI, confidence interval; CKD-EPI, chronic kidney disease epidemiology collaboration; Cr, creatinine; EORTC QLC-C30, European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire; GFR, glomerular filtration rate; inpts, inpatients; IV, intravenous; M3G, morphine-3-glucuronide; M6G, morphine-6-glucuronide; MDRD, modification of diet in renal disease; MOR, morphine; OR, odds ratio; pts, patients.
HINE, hydromorphone-induced neuroexcitation; MVA, multivariate analyses.
Morphine
In a prospective study of 109 patients with chronic malignancy-related pain using morphine, Tiseo et al. 17 evaluated the relationship between steady-state morphine and M6G plasma concentrations and opioid adverse effects, including cognitive impairment and myoclonus. Twenty-six percent (n = 28) of patients developed myoclonus, whereas 40% (n = 43) had cognitive impairment. Those receiving oral morphine had a statistically significant nearly threefold higher prevalence of myoclonus than those on parenteral morphine (34% vs. 12%; p < 0.05). Although plasma M6G:morphine ratios were higher in the oral group, it was not independently associated upon multivariate analysis (MVA). Furthermore, despite increased BUN (r = 0.40, p < 0.001) and creatinine (r = 0.45, p < 0.001) having a moderate but significant association with M6G:morphine ratios, neither was associated with cognitive impairment or myoclonus.
Ashby et al. 18 prospectively evaluated plasma morphine levels and M3G:M6G ratios in 36 hospice inpatients with cancer receiving oral (n = 17) and subcutaneous morphine (n = 19). Serum creatinine and morphine-related adverse effects, including delirium, were also assessed. Increased serum creatinine was associated with increased rates of delirium (p = 0.031), as well as greater plasma M3G (p = 0.029) and M6G (p = 0.042) concentrations, even after dose correction.
In a retrospective study using data from the multinational, multicenter European Pharmacogenetic Opioid Study (EPOS) of cancer patients (n = 1147) exclusively treated with one opioid (morphine, oxycodone, or fentanyl) for at least 3 days, Kurita et al. 20 investigated whether opioid use in renal impairment resulted in increased adverse effects, such as cognitive dysfunction. Morphine was used in 50.7% of patients (n = 581) and 11–15% of morphine users had moderate or severe renal impairment (GFR 15–59 mL/min/1.73 m2). Similar to the findings by Ashby et al., mean serum M3G and M6G concentrations were higher in patients with moderate or severe renal impairment (p < 0.01). Patients with high serum M3G concentrations (≥1262.2 nmol/L) were also more likely to report severe cognitive dysfunction (odds ratio: 1.63, 95% confidence interval: 1.03–2.56; p = 0.04). However, on MVA, the authors found no association between renal function and cognitive dysfunction.
Hydromorphone
In a retrospective study of 55 hospitalized palliative care patients switched to oral hydromorphone, Lee et al. 21 examined groups with and without renal impairment to determine hydromorphone's efficacy and associated side effects, those pertinent to this review being cognitive impairment (e.g., confusion, hallucinations, nightmares). The vast majority of patients (n = 54) had a cancer diagnosis. Both groups were switched to hydromorphone from another opioid, most commonly morphine, due to side effects. Those with renal impairment at the time of the switch to hydromorphone had a mean serum creatinine of 1.44 mg/dL with range of 1.0–8.55 mg/dL. There was no statistically significant difference between those with and without renal impairment for cognitive impairment.
Paramanandam et al. retrospectively aimed to determine the prevalence of neuroexcitation in 54 hospice patients with renal insufficiency receiving continuous IV hydromorphone infusion. 22 Neuroexcitatory effects, including tremor, myoclonus, agitation, cognitive dysfunction, and seizures, were assessed. Although none developed seizures, 11 patients (20%) developed tremors, 11 (20%) with myoclonus, 26 (48.1%) with agitation, and 21 (38.9%) with cognitive dysfunction. Tremors, myoclonus, and agitation were not associated with worsening GFR. Patients with cognitive dysfunction significantly had higher GFR than those without cognitive dysfunction (median 46.2 mL/min/1.73 m2 [range, 25.5–59.8 mL/min/1.73 m2] versus median 38.3 mL/min/1.73 m2 [range, 5.8–59.1 mL/min/1.73 m2, p < 0.025]). Nonetheless, all these adverse effects, including cognitive dysfunction, were associated with higher doses and longer duration of hydromorphone administration. In their effort to further assess the association between hydromorphone dose and duration with neuroexcitation, they observed that the prevalence of these effects correlated with increasing quartiles of hydromorphone dose and duration of use. No neuroexcitatory effects were seen for patients in the lowest quartile of hydromorphone dose or duration. Increased agitation and cognitive dysfunction were associated with increased quartile of hydromorphone dose (agitation p < 0.0001; cognitive dysfunction p < 0.0001) and duration (agitation p < 0.0002; cognitive dysfunction <0.002).
Finally, Kullgren et al. prospectively evaluated 156 hospice inpatients receiving regularly scheduled hydromorphone for development of hydromorphone-induced neuroexcitation (HINE), defined as hyperalgesia, myoclonus, allodynia, or seizures. 19 The frequency of presumed HINE was 6.4%. No seizures were noted. Similar to the finding by Paramanandam et al., the likelihood of neuroexcitation increased with larger hydromorphone doses. It also was correlated with increasing age, increasing serum creatinine, and presence of malignancy. 19 Patients who developed HINE symptoms received an average hydromorphone dose of 2.15 mg/h compared to an average hydromorphone dose of 0.88 mg/h in those without HINE. Mean serum creatinine in HINE patients was 3.2 mg/dL, compared to 1.4 mg/dL in non-HINE patients. After MVA, the diagnosis of malignancy was not a significant predictor. Since serum creatinine was not known for all patients, this variable could not be placed in the logistic regression model, limiting its ability to determine renal function as a potential predictor of neuroexcitation development.
Quality assessment
Although these studies suggest an association between hydromorphone and morphine use in renal impairment and neurotoxicity, evidence is of very low quality, seriously limiting the conclusions that may be drawn.
Lee et al. 21 focused on patients who switched from a prior opioid, a potential source of selection bias in preselecting a group intolerant to previous opioid trials, most commonly morphine.
The three morphine studies also evaluated morphine use and subsequent metabolite levels with limitations.17,18,20 Tiseo et al. 17 investigated the potential role of M6G in morphine toxicity but did not assess for M3G, the purported neurotoxic metabolite.
There was also inconsistent study reporting of cohort opioid dosing, a potential confounding factor with increased dosages associated with neurotoxicity development. This made it challenging to compare opioid dosing usage between studies. We attempted to address this issue by converting each study's reported opioid dosing to 24 hours of equivalent oral morphine dosing (Table 4). One strength of the study by Kurita et al. is patients’ exclusive morphine use for at least 3 days. 18 Although most studies reported patients’ morphine or hydromorphone dosing facilitating ease of opioid conversions,17–20,22 Lee et al. were not able to account retrospectively for all patients’ opioid doses. 21
EOM, equivalent oral morphine; HM, hydromorphone; SC, subcutaneous.
Furthermore, the lack of a standardized definition for opioid-induced neurotoxicity also made it difficult to interpret this topic's present evidence. In their review, 1 Pereira and Mercandante define “neuropsychiatric toxicities of opioids” as a wide range of central nervous system effects, but no included study used the entire broad-spectrum definition. Relevant morphine studies included heterogeneous outcomes, such as delirium, 18 confusion, myoclonus, 17 or cognitive impairment/dysfunction,17,20,21 and hallucinations or nightmares. 21 Paramanandam et al. 22 specified neurotoxicity as “neuroexcitation,” defined as tremors, myoclonus, agitation, cognitive dysfunction, and seizures, while the definition of HINE by Kullgren et al. 19 included allodynia, hyperalgesia, myoclonus, and seizures. Such varying outcome definitions may have implications on study findings.
In addition, in most studies, the presence of neurotoxic effects was assessed by a clinician or self assessed by patients without use of formal assessment tools.17–19,21,22 The lack of validated assessment tools without inter-rater reliability risked potential observer bias. In Kurita et al., 20 patients utilized the European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire (EORTC QLC-C30), a symptom self-assessment survey with a severity scale, but this study only captured these self-reports on day of data collection. The authors also never define “cognitive dysfunction,” so no guidelines existed for patients self-rating this symptom.
Moreover, although renal impairment is common, it is often challenging to accurately assess renal function by serum BUN, serum creatinine,17–19,21 or GFR.20,22 Although Kurita et al. attempted to address this challenge with renal impairment defined as GFR calculated using three different equations: Cockcroft–Gault, Modification of Diet in Renal Disease, and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI), 20 it still is limited by its dependence on serum creatinine.
Since its production is associated with patient's muscle mass, age, sex, ethnicity and diet, serum creatinine is limited in its accuracy of assessing renal function. In the seriously ill, renal function is often dynamic and based on acute factors, such as infection, decreased oral intake, or disease progression. One study of cancer patients, who commonly have some degree of renal impairment, showed that less than 10% will have an elevated serum creatinine. 30 Although imprecise, laboratory values are often used due to convenience. Adding to the complexity of measuring renal function in the severely ill, blood draws may not always be consistent with patients’ goals of care and therefore not available.18,19 Another common study constraint was the exclusion of patients with severe renal failure, whether it was related to multiorgan failure.17,18
The nature of severe illness populations, often vulnerable at the end of their lives, also makes rigorous randomized controlled trial designs difficult. 31 Studies commonly lack an adequate control group and blinding17–22 while cohorts are often small, although the multisite international study group of Kurita et al. 20 was quite large. Confounding variables such as interpatient variability/pharmacokinetics, renal failure, concomitant adjuvants for optimal symptom relief, active chemotherapies, and disease progression are prevalent. In these studies, it is often difficult to distinguish between neurotoxic effects associated directly with opioids from those related to such factors. However, clinicians also struggle with similar confounders while making medical decisions in the general hospice and palliative care population.
Discussion and Recommendations
This article aims to review the evidence on the neurotoxicity risk in morphine and hydromorphone use in patients with renal impairment as well as to reassess the current clinical practice of morphine and hydromorphone in this population.
Of note, potential bias existed in retrieval of relevant studies. Language limitations existed due to excluding non-English references, accounting for 10% (148 out of 1368) of nonduplicated references. Studies were also excluded due to their inability to directly evaluate renal impairment with morphine- or hydromorphone-induced neurotoxic outcomes, although most were case reports.32–36 By using an inclusive, broad database search, we attempted to minimize errors due to the exclusion of pertinent studies.
Another factor to consider is potential publication bias; a concern that studies with positive results may more likely be published, skewing our current evidence and recommendations. Of note, three out of six included studies did not show an association between renal impairment, morphine or hydromorphone use, and their neurotoxicity outcome.17,20,21
Opioid-related neurotoxicity is seen in the palliative care setting, but data on its prevalence are lacking. In his review, Mercandante reports a widely varying incidence of opioid-related myoclonus, ranging from 2.7% to 87%, possibly due to differences in each study's nature, assessment, and perception of symptoms, 37 similar to the varying factors in our review's investigations.
Formulation of clinical guidelines for opioid use in palliative care patients with renal dysfunction is challenging in light of the limited available evidence confirmed by this review. While current guidelines are informed by pharmacokinetic studies as well as clinical experience, conflicting pharmacokinetic data exist regarding the potential association between peripheral blood levels of both morphine/hydromorphone metabolites and presence of adverse effects.10,23,24,28
One expert consensus guideline recommends a risk-stratified approach to opioid use in renal impairment based on the presence of potentially active opioid metabolites. 38 It suggests that morphine and hydromorphone may be cautiously used with decreased dosing and decreased dose frequency in mild-to-moderate renal impairment. Particularly with patients at the end of life, clinicians should be cautious of potentially distressing neurotoxic effects related to opioids. Guidelines also advise to avoid morphine in patients with advanced renal failure, designated as an estimated GFR <30 mL/min.12,38,39 Opioids thought to lack clinically significant active metabolites, such as fentanyl and methadone, are thus suggested as first line for those with renal failure, including advanced CKD on hemodialysis.12,38–40
Given these limited studies, such guidelines recommend cautious hydromorphone use in patients with severe renal impairment.39–41 Often in practice, hydromorphone is utilized preferentially, viewed as a safer alternative to morphine with decreased risk of adverse effects. Future collaborative research, sharing databases across multiple academic centers may improve study design and data collection.
In summary, current literature on this topic is sparse and has serious limitations. Based on limited evidence, pharmacokinetic data, and current expert guidelines, hospice and palliative care clinicians may consider cautious use of morphine and hydromorphone in mild-to-moderate renal impairment, closely monitoring for neurotoxic effects particularly when using higher opioid dosing for longer duration of time. In patients with severe renal impairment and/or on hemodialysis, the risk of such adverse effects is likely to be higher with either morphine or hydromorphone use.
Footnotes
Acknowledgment
The authors thank Rachel Pinotti, MLIS, for her aid in creating our electronic reference search strategy.
Author Disclosure Statement
No competing financial interests exist.