
Abstract
Abstract
Background:
Comprehensive information on end-of-life care in specialized palliative care settings is needed to assess the quality of care.
Objective:
This study aimed to investigate medical treatments in the last two weeks of life in a national sample of palliative care units in Japan.
Design:
Retrospective cohort study.
Setting/Subjects:
Medical charts of 2802 consecutive cancer patients who died in 37 palliative care units were reviewed.
Measurements:
Drug usage and treatments during the last two weeks of life were collected. A mixed-effect model was used to estimate the variations in care between institutions.
Results:
Opioid administration increased from 68% (two weeks before death) to 80% (last 48 hours); during the same period, nonsteroidal anti-inflammatory drugs and acetaminophen administration decreased from 59% to 45%, and corticosteroid administration decreased from 62% to 51%. As death neared, parenteral opioid administration increased (41%–74%). Morphine use increased (45%–70%), fentanyl use remained about the same (47%–40%), and oxycodone use decreased (18%–5%). Two thirds of patients received artificial hydration; doses >1000 mL/day (15%) and intravenous hyperalimentation (7%) were relatively rare during the last 48 hours. Variations in end-of-life medical treatments increased between palliative care units as death neared, especially anticholinergic, artificial hydration, oxygen inhalation, and palliative sedation use.
Conclusions:
These findings regarding the general course of palliative treatments for dying cancer patients are useful for clinical audits in general wards, by comparing end-of-life care. Variations in some end-of-life medical treatments between institutions increased as death neared, even in palliative care settings.
Background
P
In Japan, palliative care developed from the inpatient care provided for terminally ill cancer patients. The fee for care in a palliative care unit became eligible for reimbursement under the medical insurance system in 1990. Subsequently, coverage for the costs of care provided by a hospital-based palliative care team became eligible in 2002. A total of 368,000 cancer patients in Japan died during the fiscal year 2014, of which 10% made use of a palliative care unit. Specialized palliative care is steadily growing, with the trend moving away from palliative care units toward palliative care teams and home-based care, driven by government policies relating to palliative care, including the establishment of the Cancer Control Act formulation in 2006. 10 Nevertheless, there is disparity in the end-of-life care provided for dying cancer patients between the general wards and palliative care units in Japan.11–13 A nationwide survey also highlighted the potential differences in medical and nonmedical care performed within palliative care units in Japan; the authors suggested a need for a more detailed survey based on actual patient data. 14 A nationwide chart review of end-of-life medical treatments in palliative care units would document the activities required for end-of-life care not only in palliative care units but also in the general wards.
This study primarily aimed to determine the current status of end-of-life medical treatments in the last two weeks of life in palliative care units in Japan. The secondary aim was to document variations in end-of-life medical treatments between palliative care units.
Methods
We conducted chart reviews as part of the Japan HOspice and Palliative care Evaluation (J-HOPE) study, which was a large, nationwide retrospective questionnaire and chart review study to evaluate the dying experiences of cancer patients in Japan. Detailed methods of the J-HOPE study have been described elsewhere. 15
Participants
Of all the palliative care units (n = 158) in Japan in 2005, we recruited all palliative care units registered in Hospice Palliative Care Japan (n = 153, 97%) for the J-HOPE questionnaire study of bereaved family members with or without chart review study. Of those, 37 (23%) participated in both questionnaire and this chart review survey and 63 participated in only a questionnaire survey. The structure of palliative care units did not significantly differ between participation in chart review study or not, such as number of beds, healthcare professionals, and patients (data not shown).
Potential participants were adult cancer patients who died in the 37 palliative care units between June 2005 and October 2006. The exclusion criteria were that the bereaved family members refused to participate, the patient was hospitalized in a palliative care unit for <3 days, or the address was unknown. We excluded the short hospitalized patients due to be in the middle of arrangement of care during the last 48 hours. The charts of up to 80 cancer patients in each institution were reviewed. We set the sample size to have 50 respondents of questionnaire survey in each institution.
We sent out a letter describing the chart review study to bereaved families with the questionnaire enclosed. The families were instructed to review and return the form if they refused to participate in the chart review study.
Procedures
The medical chart reviews were conducted by physician and nursing staff in each institution in 24 palliative care units and two trained research nurses from the research management office in 13 palliative care units at the request of the institution. The research office requested the former way when possible due to reliability of chart review, although we preliminarily confirmed reliability of the latter way. To assess inter-rater reliability between a palliative care unit staff member and an investigator from the office, 5% of randomly selected medical charts from two palliative care units were independently abstracted. The average rate of agreements was 93%. Subsequently, to assess inter-rater reliability between two investigators from the office, 10% of randomly selected medical charts in 13 palliative care units were independently abstracted. The average rate of agreement was 97%. We did not use kappa coefficient because it becomes unreliable when the distribution of the dichotomous variable is unbalanced; therefore, despite the high level of agreement, kappa would be very low.
The chart review was conducted between May and December 2008. The Ethics Committee of the University of Tokyo and each institution approved this study.
Measures
Four major data categories were collected from the medical charts, using a data collection sheet: patient characteristics, drug usage in palliative care during the last two weeks of life, end-of-life treatments during the last two weeks of life, and quality indicators (QIs) of end-of-life cancer care. Drug usage and end-of-life treatments were reviewed at three time points: two weeks (14–15 days) before death, one week (7–8 days) before death, and during the last 48 hours before death. QIs were assessed for all patients who died in palliative care units, regardless of their length of stay. Feasibility was certified by a pilot test at a single center. 11 Content validity was checked by three palliative care physicians and two research nurses before the medical chart review was conducted.
Patient characteristics included sex, age, marital status, primary cancer site, history of cancer treatment, length of time since cancer diagnosis, palliative care referral, length of hospital stay, length of palliative care unit stay, transfer from a general ward, number of palliative care unit hospitalizations, and oral intake. Symptom-relieving drugs included the 10 classes of drugs that Nauck et al. 16 reported were used most commonly in palliative care: opioids, nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen, corticosteroids, antipsychotics, anxiolytics/sedatives, antidepressants, laxatives, antiemetics, and anticholinergics. End-of-life treatments included the provision of artificial hydration, intravenous hyperalimentation, tube feeding, palliative sedation, antibiotics, oxygen inhalation, or urinary catheterization. Palliative sedation was defined by the dosage amount of sedative drugs, using criterion similar to that used by Sykes and Thorns. 17 We used QIs that Earle et al. 18 identified to assess the aggressiveness of cancer care near the end of life for all patients died in the units: a new chemotherapy regimen within 30 days before death, chemotherapy within 14 days before death, and ≤3-day stay in the palliative care unit during the last month of life.
Analyses
We calculated the relative frequencies for categorical variables and the median and lower and upper quartiles for quantitative variables. We did not statistically test time-dependent changes because the sample sizes at the three time points were unbalanced due to the differences in the length of stay. Next, we visually assessed differences between institutions using box and whisker plots of the adjusted percentages of the patients receiving end-of-life treatments and drugs in each palliative care unit. We used the adjusted percentages to exclude the effect of patient characteristics heterogeneity. A mixed-effect logistic regression model was used to estimate the predicted percentages of each patient, adjusting for patient sex, patient age, primary cancer site, and a random institution effect. The adjusted percentages were means of the predicted percentages. We also calculated variance proportions as indicators of variations in care between institutions. The variance proportion was the proportion of the variance component of the random institutional effect divided by the variance component of the random institutional effect plus error variance. We used a mixed-effect regression model to calculate the variance proportion in a way similar to intraclass correlation coefficients in previous study. 19 A larger variance proportion indicates larger institutional variations. A p value <0.05 was considered statistically significant. All statistical analyses were performed with SAS version 9.3 for Windows (SAS Institute, Cary, NC).
Results
Among the 2935 potential patients, 2897 (99%) medical charts were reviewed; 3 medical charts were excluded because the families refused to participate and 35 were excluded because of missing data. Ninety-five subjects were excluded because the palliative care unit length of stay was <3 days. The charts of 1885, 2352, and 2802 decedents were analyzed for two weeks before death, one week before death, and the last 48 hours of life, respectively. Of 2802 descendants, 176 (6.2%) died in 2005 and 2626 (94%) died in 2006.
The median age of the patients was 72 years, and 55% of the patients were men (Table 1). The primary cancer sites were lung (23%), hepatobiliary and pancreatic (17%), gastric and esophageal (17%), and colorectal (13%). The median lengths of hospital and palliative care unit stays were 34 and 24 days, respectively.
Several total percentages are not 100% due to missing values.
IQR, interquartile range.
Drug usage in palliative care
Many patients were administered opioids and NSAIDs or acetaminophen as analgesics (Table 2). The use of opioids increased from 68% two weeks before death to 80% during the last 48 hours, whereas the use of NSAIDs and acetaminophen decreased from 59% to 45%. As the end of life neared, the use of oral and transdermal opioids decreased (25%–5% and 41%–32%, respectively) and parenteral opioids increased (41%–74%). The use of morphine increased, and the use of oxycodone decreased. The use of antipsychotic, anxiolytic/sedative (parenteral), and anticholinergic drugs increased, while the use of corticosteroid, anxiolytic/sedative (oral and rectal), antidepressant, laxative, and antiemetic drugs decreased.
Several total percentages are not 100% due to missing values.
NSAIDs, nonsteroidal anti-inflammatory drugs; SD, standard deviation.
End-of-life treatments
Table 3 lists the frequencies of end-of-life treatments at the three time points, including separate values for patients with and without oral intake. The use of artificial hydration, oxygen inhalation, and urinary catheterization increased in the last two weeks of life; the use of artificial hydration nearly doubled, and use of oxygen inhalation more than doubled, from the last two weeks to the last 48 hours of life. However, use of hydration >1000 mL/day and intravenous hyperalimentation decreased. The frequency of antibiotic use was almost constant (16%–13%), and tube feeding was infrequent. Palliative sedation was provided for 25% of the patients in the last 48 hours of life.
Several total percentages are not 100% due to missing values.
The definition is the patients who could drink a mouthful of water or less.
Variations in end-of-life drug usage and treatments between the palliative care units
Institutional variations in drug usage in palliative care and end-of-life treatments are shown in Figures 1 and 2. Institutional variations increased for most treatments as death neared. Variations in drug usage in palliative care were relatively large for anticholinergics, antipsychotics, and anxiolytics/sedatives (parenteral agents) during the last 48 hours. Variations in artificial hydration, oxygen inhalation, palliative sedation, and intravenous hyperalimentation during the last 48 hours also were relatively large.
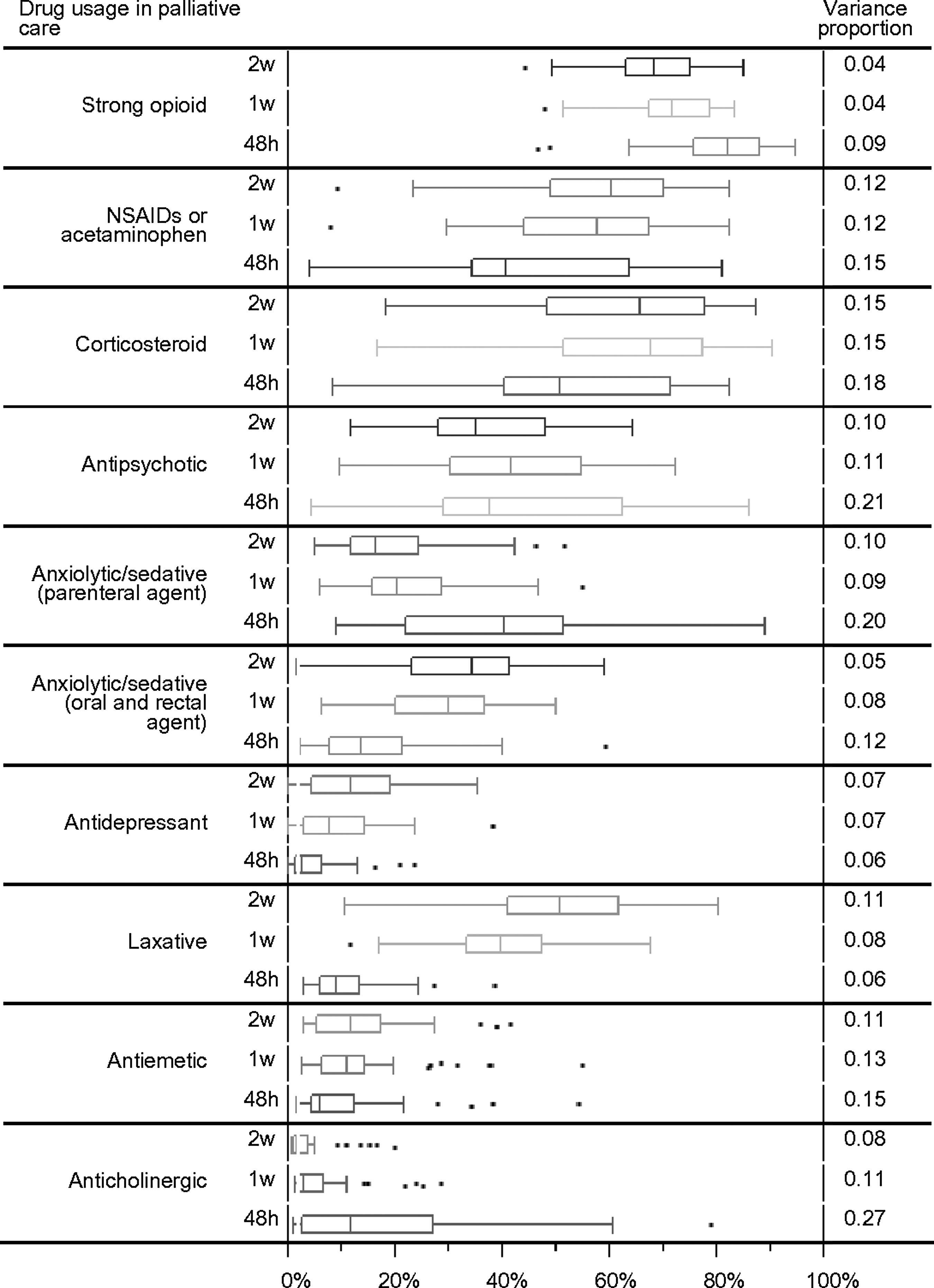
Institutional variations in end-of-life drug usage for patients with cancer in 37 palliative care units. The box and whisker plots represent the adjusted percentages of the patients using drugs in each palliative care unit two weeks before death (2w), one week before death (1w), and in the last 48 hours before death (48h). The box displays the median values and 25th and 75th percentiles of the distribution; whiskers extend to the most extreme data point that is no more than 1.5 times the interquartile range from the box. The variance proportions were indicators of institutional variations.

Institutional variations in end-of-life treatments for patients with cancer in 37 palliative care units. The box and whisker plots represent the adjusted percentages of the patients receiving end-of-life treatments in each palliative care unit two weeks before death (2w), one week before death (1w), and in the last 48 hours before death (48h). The box displays the median values and 25th and 75th percentiles of the distribution; whiskers extend to the most extreme data point that is no more than 1.5 times the interquartile range from the box. The variance proportions were indicators of institutional variations.
Aggressiveness of cancer care near the end of life
A few patients who died in the palliative care units received certain types of aggressive care, such as starting a new chemotherapy regimen within the 30 days before death (n = 19, 0.7%), receiving chemotherapy within 14 days before death (n = 30, 1.0%), or staying in the palliative care unit ≤3 days (3.3%). Of the 19 patients who started a new chemotherapy regimen within the 30 days before death, 14 patients received parenteral treatment; 5 of these patients started treatment in the palliative care unit (paclitaxel, docetaxel, cisplatin, and picibanil). The other 5 of the 19 patients received oral treatment; 2 started treatment in the palliative care unit (cyclophosphamide and gefitinib). Of the 30 patients who received chemotherapy within the last 14 days of life, 11 received parenteral treatment; 9 were treated in the palliative care unit (gemcitabine, paclitaxel, docetaxel, etoposide, leuprolide, interferon, and picibanil). Of the 30 patients, 21 received oral treatment; 16 patients were in the palliative care unit (cyclophosphamide, tegafur, capecitabine, gefitinib, imatinib, and other hormone agents).
Discussion
To the best of our knowledge, this retrospective study is the first to comprehensively examine end-of-life medical treatments provided during the last two weeks of life in 37 palliative care units in Japan and to document variations in these treatments. The findings could be provided as feedback to each institution for check and assessment of end-of-life care.
Institutional variations in some end-of-life medical treatments increased as death neared, even after adjusting for patient age, sex, and primary cancer site, suggesting that end-of-life treatments provided to terminally ill cancer patients who are expected to die within a few days or hours are not standardized. This was especially apparent for anticholinergic, artificial hydration, oxygen inhalation, and palliative sedation use. This variation could be related with differences in disease status and the physician's preferences for care. Previous studies have been conducted for institutional variations in pain management19–21 and regional variations in palliative radiotherapy, 22 advance directives, 23 acute care services at the end of life, 24 and end-of-life costs 25 ; the present study provides a comprehensive view of institutional variations. Therefore, further research is needed to determine the rationale for and outcomes of variations in end-of-life medical treatments that may affect the quality of specialized palliative care services in palliative care units.
Strong opioids were used for 68% of the cancer patients two weeks before death, increasing to 80% in the last 48 hours of life. Opioid usage in the last 48 hours was similar to that reported by surveys of palliative care units in Western countries8,16,26 and parallels the prevalences of pain and dyspnea.27–29 The percentage did not reach 100% because some dying patients do not experience severe distress and other patients experience decreased consciousness. 30 Parenteral administration increased as patients approached death and were unable to eat, although transdermal administration was still used. Morphine was mainly administered parenterally, and its use increased near death, probably because clinicians were accustomed to effectively relieving concurrent dyspnea.31,32
Corticosteroids were consistently used for approximately half of the dying cancer patients within the last two weeks of life, most commonly betamethasone or dexamethasone. A nationwide survey of physician-reported practices and attitudes in 124 palliative care units in Japan found that corticosteroids were commonly used for fatigue, anorexia, and dyspnea. When patient death was imminent, 79% of physicians reported that they abruptly ceased or reduced corticosteroid use. 33 A discontinuation or reduction in corticosteroid use was not observed as often in the present study.
Antipsychotic drugs were used for 37% of the cancer patients two weeks before death, increasing to 44% in the last 48 hours. The drug type changed from haloperidol and atypical antipsychotics to mainly haloperidol; both of these are prescribed for delirium, 34 which is common in the last weeks of life, occurring in 26%–44% of people with advanced cancer in hospitals and up to 88% of people with terminal illness in the last days of life. 35 Haloperidol during the last 48 hours can also be used as a mild or moderate sedative. Institutional variation in the use of antipsychotics was relatively wide and might be related with differences in the clinicians' assessment and treatment of end-of-life delirium, as well as attitudes toward palliative sedation.
Oral anxiolytic/sedative administration decreased, while parenteral administration increased as death approached. Before the last two weeks of life, one third of cancer patients probably received anxiolytic/sedative drugs to treat insomnia. In a systematic review, sleep disturbance was prevalent in 30%–70% of patients in hospice or palliative care units and insomnia was associated with uncontrolled physical symptoms, psychological problems, and poor quality of life. 36 Therefore, insomnia is a common problem requiring treatment in terminally ill cancer patients. In addition, anxiolytic/sedative drugs may be used near death for palliative sedation rather than insomnia. In a large multicenter prospective cohort study, 15% of cancer patients received continuous deep sedation before death, mainly with midazolam. 37 The present study indicated that more patients were sedated because of the intermittent and mild sedation.
Anticholinergics were used almost exclusively during the last 48 hours, suggesting the purpose of alleviating death rattle rather than inhibiting digestive juice secretion in the presence of an intestinal obstruction. The rate of anticholinergic use was less than the prevalence of death rattle at the end of life, which occurs in approximately half of dying patients.30,38,39 In addition, institutional variations in the use of anticholinergics and artificial hydration were relatively large within the last 48 hours, suggesting that treatment for death rattle was not standardized, although the volume of infusion was limited to <1000 mL/day. However, the use of artificial hydration in the palliative care units was generally consistent with the Japanese clinical guidelines for artificial hydration therapy for terminally ill patients. 40
Oxygen has no value in alleviating dyspnea in patients without hypoxemia and may have adverse effects, including restricted activities, possible quality of life impairment, and psychological dependence. 32 Similarly, urinary catheterization might decrease quality of life. However, oxygen inhalation and urinary catheterization were popular in the palliative care units in Japan based on the results of the present study. These are not necessarily contraindications, because proper care must be determined on an individual basis, considering the balance between benefit and harm.
According to the QIs, a relatively small number of cancer patients who died in the palliative care units stayed for only a short time, although long wait times for admission and long hospital stays (median 35 days in 2014) were issues. The difficulty of staying at home at the end of life is a problem in Japan. In addition, a few patients received irregular chemotherapy within the last two weeks of life. However, the development of targeted molecular therapies would complicate palliative chemotherapy at the end of life. Furthermore, palliative chemotherapy may contribute to improved quality of life, such as fighting cancer and maintaining hope, which are a part of the concept of a good death. 41
This study has several limitations. First, we did not collect information about symptoms because of insufficient documentation in the medical and nursing records. Second, multicenter participation in the study limited the standardization of the chart review procedures. The data may be biased, although we demonstrated high inter-rater reliability. Third, the low participation rate might have introduced selection bias; however, one-quarter of the total number of palliative care units that existed at the time of the study was included. In addition, we could not use the administrative data such as insurance claims because it structurally lacked the detailed information about the care provided in palliative care units due to a single fixed medical fee, regardless of the care in Japan. Fourth, we evaluated inter-rater reliability by small sample size due to feasibility of chart review and not by kappa coefficient due to statistical reason. Finally, the data are old. Some new opioid products are now used in Japan.
Conclusions
The findings of this retrospective cohort study that examined end-of-life medical treatments in the last two weeks of life in 37 palliative care units in Japan revealed the general course of palliative treatments for dying cancer patients, which could be used for clinical audits in the general wards, by comparing end-of-life care. Variations in some end-of-life medical treatments between centers increased as death neared, especially in anticholinergic, artificial hydration, oxygen inhalation, and palliative sedation use. Therefore, some end-of-life treatments during the last few days and hours of life were not standardized, even in specialized palliative care settings. Further study is needed to show the rationale for and outcomes of variations in end-of-life medical treatments, to assess the quality of specialized palliative care services in palliative care units.
Footnotes
Acknowledgments
This study was supported by a Grant-in-Aid from the Japan Hospice Palliative Care Foundation. The authors would like to express their gratitude, for collaboration in this study, to Ikue Sato, Higasi Sapporo Hospital; Tetsuro Ogasawara, Miyagi Cancer Center; Takao Yoshimura, Mito Saiseikai General Hospital; Go Kobayashi, Nishigunma National Hospital; Akitoshi Hayashi, St Luke's International Hospital; Natsuki Hori, NTT Medical Center Tokyo; Osamu Akiyama, Japanese Red Cross Medical Center; Yosuke Yamada, Toshima Hospital; Yoshiaki Kanai, Shin-ai Hospital; Kenji Nishitateno, Peace House hospice; Kinzo Sakurai, Nanbugo General Hospital; Toshio Watanabe, Toyama Prefectural Center Hospital; Yasuhiko Tatsuzawa, Saiseikai Kanazawa Hospital; Makoto Hirakata, Suwa Central Hospital; Fumiaki Abe, Yamanashi Prefectural Central Hospital; Akihiko Suga, Shizuoka General Hospital; Satoshi Inoue, Seirei Mikatahara General Hospital; Hideaki Ieda, Nagoya Ekisaikai Hospital; Hiroyuki Nagae, Minami Seikyo Hospital; Yohei Ohashi, Kainan Hospital; Masayuki Ikenaga, Yodogawa Christian Hospital; Hirofumi Abo, Rokko Hospital; Rieko Sai, Higashi-Kobe Hospital; Ryo Tamura, Himeji St. Mary's Hospital; Tatsuhiko Ishihara, Okayama Saiseikai General Hospital; Takashi Iwata, Shimura Hospital; Masahiro Matsuura, Hiroshima City Aki Hospital; Hideki Katayama, Yamagushi-Ube Medical Center; Hiroko Noda, Mitoyo General Hospital; Noriko Tanida, Kondo Hospital; Izumi Iwamoto, Kochi Kosei Hospital; Wataru Hirata, Tatara Rehabilitation Hospital; Kazumi Yamashita, Haradoi Hospital; Misako Matsumoto, Kahan Hospital; Chikako Kato, St. Francis Hospital; Keiji Goto, Kumamoto Regiaonal Medical Center; and Norio Yamaoka, Oita Yufumi Hospital.
Author Disclosure Statement
No competing financial interests exist.