
Abstract
Abstract
Background/Aims:
The optimal regimen of radiotherapy (RT) for bleeding from gastric cancer (GC) has not yet been established. The aim of this study was to evaluate the usefulness of low-dose, short-course palliative RT (LSP-RT) for bleeding from GC.
Material and Methods:
We reviewed the clinical data of 18 patients (26 courses) who received palliative RT for bleeding from GC between 2004 and 2014. The radiation dose was 6 Gy in three fractions. The total courses of RT for each patient were 1–4 (median, 1).
Results:
The treatment success rate of the first and the additional RT at two weeks after RT was 55% and 75%, respectively. Regarding first RT, there was a statistically significant increase in the mean hemoglobin level for one month (p = 0.009) and a significant decrease in the mean number of transfused red blood cell units for one month (p = 0.012). Toxicities were observed in two patients: one patient who received chemotherapy developed grade 3 afebrile leukocytopenia and another who had a malignant stricture suffered from a gastric obstruction. The performance status was improved in 3 of the 12 evaluable patients (25%) and dietary intake became possible one month after RT in three of the four patients who had not been able to eat before RT.
Conclusion:
LSP-RT is expected to be not only an effective and safe treatment option for bleeding from GC, but also repeatable in cases of rebleeding. Furthermore, this treatment modality may be able to improve the patient's quality of life.
Introduction
S
In contrast, RT may be indicated even for patients in a poor general condition and for various types of bleeding, which can control tumor bleeding in 54%–91% of patients.4–8,10 Although 30 Gy in 10 fractions is one of the most commonly used regimens, the usefulness of low-dose, short-course regimens has not yet been investigated.
We evaluated the usefulness of low-dose, short-course palliative RT (LSP-RT) for bleeding from GC.
Material and Methods
We retrospectively reviewed the clinical data of all patients who received palliative RT for bleeding from unresectable GC in our institution between 2004 and 2014. The inclusion criteria were histopathologically proven adenocarcinoma in the stomach, diagnosed bleeding from GC based on endoscopic or computed tomography findings and from clinical symptoms such as melena or hematemesis with the progression of anemia, and patients with uncontrolled bleeding who were unfit for other treatment strategies despite a blood transfusion. The additional treatment was defined as another course after completing the planned treatment regimen with the same indication as already described.
All patients were treated with external beam RT using photons of 4 or 10 MV from a linear accelerator. Only primary lesions were included in the clinical target volume. All patients were treated with opposed anterior–posterior two fields.
The radiation dose of both the first and the additional retreatment was 6 Gy in three fractions.
The effectiveness of RT was evaluated by the mean serum hemoglobin (Hb) level and the number of transfused red blood cell (RBC) units before and after RT. Treatment success was defined as the absence of a decrease in the serum Hb level without any bleeding symptoms.
Treatment toxicities were assessed according to the Common Terminology Criteria for Adverse Events (version 3.0).
All statistical analyses were performed using the SPSS version 22. Wilcoxon's signed rank test was used to compare the mean Hb levels and the number of transfused RBC units before RT with the values after RT. Statistical significance was considered to exist as p values <0.05. The biologically effective dose (BED) was calculated using a tumor alpha/beta ratio of 10.
Results
Eighteen patients had received palliative RT for bleeding from unresectable GC during the study period. The patient characteristics are outlined in Table 1. The median Eastern Cooperative Oncology Group performance status (PS) was 3 (range, 2–4). Dietary intake was impossible in five patients.
ECOG, Eastern Cooperative Oncology Group; RT, radiotherapy.
In 12 patients (66%), bleeding from GC was confirmed by esophagogastroduodenoscopy (EGD). EGD was not performed in six patients because of their poor general condition or because they were unwilling to undergo EGD. However, no other organic lesions were identified as causing bleeding in the previous EGD. Furthermore, all six patients had taken proton pump inhibitor (PPI) before the occurrence of bleeding.
Previous, concurrent, and additional chemotherapy was conducted in 13, 2, and 8 patients, respectively.
Six patients received a total of eight additional courses of RT for rebleeding: five patients received one additional course, and one patient received three additional courses of RT. The median (range) time from the end of the previous RT to the additional RT of 8 courses was 41 (15–231) days. Three patients received the additional RT within four weeks after the first RT. All patients completed the planned regimen of treatment. The total radiation dose of each patient is shown in Table 2.
The treatment success rate of first RT at two and four weeks after the first RT was 55% (10 out of 18 patients) and 44% (8 out of 18 patients), respectively. Three patients died within four weeks after RT. Although the rebleeding rate was 72% (13 out of 18 patients), the rate of RT retreatment was 46% (6 out of 13 patients). The treatment success rate of the additional RT at two and four weeks after the treatment was 75% (six out of eight patients) and 25% (two out of eight patients), respectively. One patient died within four weeks after retreatment. Although the rebleeding rate was 62% (five out of eight patients), the rate of RT retreatment was 40% (two out of five patients). No patients died because of persistent bleeding.
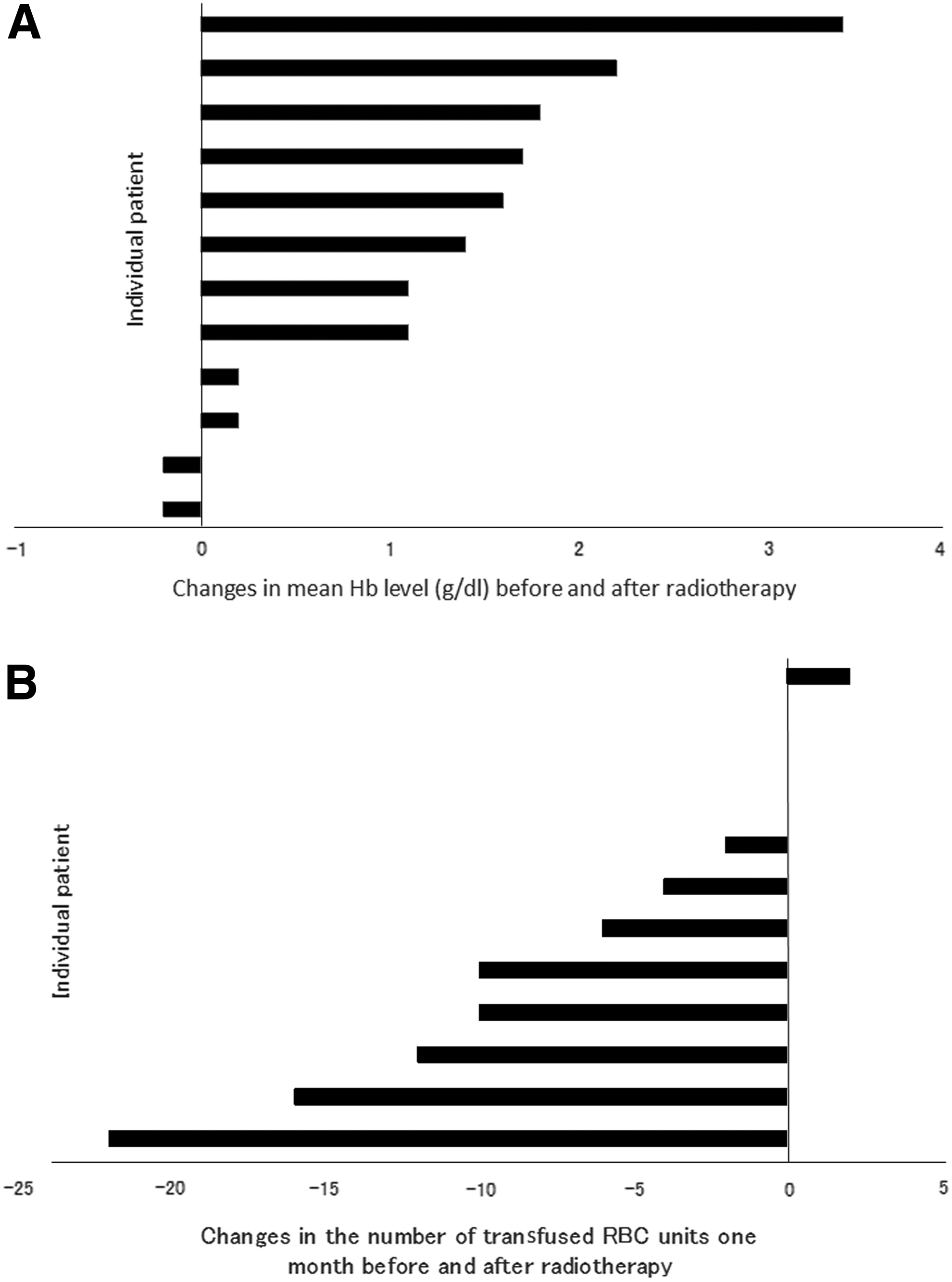
Regarding first RT, in the 12 excluding the 6 patients who died within four weeks and who received additional RT within four weeks, the mean Hb levels one month before and after RT were 7.4 ± 1.0 and 8.6 ± 0.8 g/dl, respectively (p = 0.009) (Fig. 1A). The mean number of transfused RBC units one month before and after RT was 9.5 ± 6.4 and 2.8 ± 3.8, respectively (p = 0.012) (Fig. 1B).
Regarding additional RT for rebleeding, in the seven patients excluding one patient who died within four weeks, the mean Hb levels one month before and after RT were 7.5 ± 0.8 and 8.6 ± 1.1 g/dl, respectively (p = 0.057) (Fig. 2A). The mean number of transfused RBC units one month before and after additional RT was 7.5 ± 2.3 and 4.0 ± 4.6, respectively (p = 0.328) (Fig. 2B).

The distribution of PS 1 month after the first RT among the 12 excluding the 6 patients who died within 4 weeks and those who received additional RT within 4 weeks is shown in Table 2. The PS was improved in three patients (25%), unchanged in eight patients, and deteriorated in one patient. Dietary intake became possible one month after RT in three of the four patients, whereas the dietary intake conditions of the other nine patients did not change.
Toxicities were observed in two patients: one patient who received chemotherapy developed grade 3 afebrile leukocytopenia and one who had a malignant stricture suffered from obstruction that required stenting.
Seventeen patients were treated as inpatients, whereas one patient was treated as an outpatient. Seven of the 17 patients were successfully discharged, whereas 10 patients died during hospitalization.
Discussion
Although various dose fractionation regimens, which ranged from 8 to 60 Gy, have been tested in recent retrospective studies,4–10 the correlation between the dose and response has been controversial. Chaw et al. 8 evaluated the effectiveness of LSP-RT with mainly 8 Gy single fraction (a BED of 14.4 Gy), which demonstrated results similar to those found in other studies. We also showed that LSP-RT was effective by comparing the mean Hb level and the mean number of transfused RBC units before and after RT. All of the patients in our study received 6 Gy in three fractions (a BED of 7.2 Gy), which is the lowest reported BED. Low-dose RT resulted in a temporal hemostatic effect in the majority of the patients, and this result was similar to the results of the higher dose treatment. This may indicate that even low doses of irradiation can lead to vascular damage to the tumor vessels.
The treatment success rate at four weeks after RT was decreased to 44%, which was inferior to that of previous reports. This may suggest that low-dose RT has a shorter effect of hemostasis. However, despite rebleeding, less than half of the patients required repeat RT. The durable effect of RT may prevent massive bleeding from the tumor; thus, slowly progressive anemia cause by slight bleeding may be controlled by appropriate blood transfusion.
We also showed that additional low-dose RT for rebleeding was as effective as first RT without any toxicity. The repeatable use is one of the advantages of low-dose RT.
In the previously reported studies, grades 3–4 adverse events such as leukocytopenia, neutropenia, nausea, vomiting, and anorexia occurred in 0%–21% of the patients. Although two adverse events were observed in this study, chemotherapy-related toxicity was suspected in one patient with leukocytopenia.
The PS was improved and dietary intake became possible in a considerable number of the patients after RT despite the advanced stage of their disease. LSP-RT is not only an effective and safe treatment option but also has a possibility to improve the patient's quality of life (QOL), which appears to be one of the greatest concerns for patients with a limited life expectancy.
There are a few limitations associated with this study. First, this is a retrospective, small sample study, similar to the previously reported studies. It is important to evaluate the promising regimens prospectively and to make efforts to identify the optimal treatment. Second, because we did not perform EGD for all the patients before RT, it is possible that the patients had other bleeding diseases. However, we thought the existence of such diseases to be unlikely because no organic lesions other than GC were identified in the previous EGD, and because all of the patients had been taking PPIs.
Conclusion
LSP-RT is expected to be not only an effective and safe treatment option for bleeding from GC but is also a repeatable treatment in cases of rebleeding. Furthermore, this treatment modality may be able to improve the patient's QOL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.