
Abstract
Abstract
Background:
End-of-life (EoL) care after geriatric burns (geri-burns) is understudied.
Objective:
To examine the practices of burn surgeons for initiating EoL discussions and the impact of decisions made on the courses of geri-burn patients who died after injury.
Methods:
This retrospective cohort study examined all subjects ≥65 years who died on our Level I burn service from April 1, 2009, to December 31, 2014. Measurements obtained were timing of first EoL discussion (EARLY <24 hours post-admission; LATE ≥24 hours post-admission), decisions made, age, total body surface area burned, and calculated probability of death at admission.
Results:
The cohort consisted of 57 subjects, of whom 54 had at least one documented EoL care discussion between a burn physician and the patient/surrogate. No differences were seen between groups for the likelihood of an immediate decision for comfort care after the first discussion (p = 0.73) or the mean number of total discussions (p = 0.07). EARLY group subjects (n = 38) had significantly greater magnitudes of injury (p = 0.002), calculated probabilities of death at admission (p ≤ 0.001), shorter times to death (p ≤ 0.001), and fewer trips to the operating theater for burn excision and skin grafting (p ≤ 0.001) than LATE subjects (n = 16). LATE subjects' first discussion occurred at a mean of 9.3 ± 10.0 days.
Discussion:
The vast majority of geri-burn deaths on our burn service occur after a discussion about EoL care. The timing of these discussions is driven by magnitude of injury, and it does not lead to higher proportions of an immediate decision for comfort care. The presence and timing of EoL discussions bears further study as a quality metric for geri-burn EoL care.
Introduction
I
Although the need for quality EoL care in general ICU populations has been demonstrated, similar concepts remain understudied in the field of geriatric burns (geri-burns). Geri-burn admission usually follows a catastrophic event that frequently leaves elders with a loss of capacity for self-determination, and the surrogates who must be relied on to make decisions with irreversible consequences often grapple with feelings of shock and guilt. In addition, burn care is unique in that optimal care dictates that operative excision of full-thickness burns with skin graft placement should commence at 24 hours after injury. This means that surrogate decision makers must commit the elderly patient to an invasive and painful treatment plan relatively quickly. Burn providers may, in turn, feel compelled to delay having conversations about code status or possible limitations on the aggressiveness of clinical efforts out of respect for the emotional suffering of surrogates or due to the fear of alienating them by discussing EoL care so soon after injury. However, the compressed nature of the time frames for decision making in geri-burn care ensures that there will rarely be a “good time.”
Multiple studies have documented the benefits of documentation of code status in general populations, including a decrease in the number of interventions that patients receive that are not aligned with their values and preferences.8,9 With that in mind, we sought to investigate the impact of the timing of goals of care discussions (including those addressing code status and treatment plans) on outcomes in geri-burn patients who did not survive their injury. We hypothesized that an early discussion (i.e., within 24 hours of admission) would significantly decrease the number of surgical procedures performed on these patients who ultimately died.
Methods
After approval by our local Institutional Review Board, our prospectively maintained burn registry was queried for all patients aged 65 years or older who were admitted to the Parkland burn service between April 1, 2009 and December 31, 2014 and who died during their index admission. Parkland is a Level I burn center that has been verified by the American Burn Association since 1999. All electronic charts were reviewed for basic demographics, preexisting medical conditions (including chronic cardiac, pulmonary, and liver disease or a prior diagnosis of cancer), clinical course, documentation and timing of discussions of code status and treatment plans, and patient or surrogate decisions regarding the plan of care. Frailty syndrome was retrospectively assessed by using the Canadian Study of Health and Aging clinical frailty scale, which assigns a frailty score of 1 (very fit) to 7 (severely frail). 10
On the Parkland burn service, the decision to initiate a discussion regarding code status and aggressiveness of care is always made by the attending burn surgeon. The burn personnel leading the conversation and the manner in which it is conducted are not standardized and occur across a wide spectrum of practice. Given this variability, we elected to simply dichotomize the outcome as to whether documentation of a conversation existed.
The national standard of care for the early management of burn injury is for patients to undergo a vigorous crystalloid resuscitation for the first 24 hours after injury, and at the completion of the crystalloid resuscitation all full-thickness burns should be sharply excised in an attempt to attenuate the hypermetabolic storm that is the hallmark of a severe burn. We, therefore, dichotomized patients into an EARLY group, in which the first discussion about code status and aggressiveness of the care plan took place within the first 24 hours after admission, and a LATE group in which the first discussion took place at any point thereafter. All EoL discussions were conducted with patients or their surrogates by using subjective, nonquantitative estimates of the likelihood of death.
The principle investigator (PI) for this study is a member of the PALLIATE consortium, a multicenter and multidisciplinary group with special expertise in care of the injured elderly patient. In a recent study, the PALLIATE consortium developed a prognosis calculator that is specific to geri-burn patients by using a decade-long national sample from the National Burn Repository that objectively estimates probability of mortality during the index admission 7 (Table 1). This prognosis calculator is based on the Baux score, a scoring system that is widely accepted in the burn community and is easily calculated at the bedside.11,12 The Baux score is simply the patient's age plus their percentage of total body surface area (TBSA) burned. As an example, a 70-year-old who suffered a 40% TBSA burn would have a Baux score of 110. For the present study, we retrospectively applied this prognostic tool to our sample population to estimate the probability of mortality for each subject based on their Baux score. These objective determinations of the probability of death were not available at the time of admission, and they were not used during EoL counseling for the study sample. Student's t test was used for continuous data, and Fisher's exact test was used for proportions. Alpha was set at 0.05.
Baux scores have been grouped by decile, with corresponding likelihoods of death during the index admission for burn injury.
Results
The study sample comprised 57 subjects with a Baux score distribution, as seen in Figure 1. Of this sample, 54 subjects (95%) had at least one documented discussion between a burn physician and the patient or surrogate regarding code status and aggressiveness of the treatment plan. Comparisons of the EARLY and LATE groups can be found in Table 2. Notably, all patients in both groups had a designated surrogate available either in person or via telephone. Of subjects in whom a discussion was documented, 5% expired with a status of full code and while undergoing full resuscitative efforts.
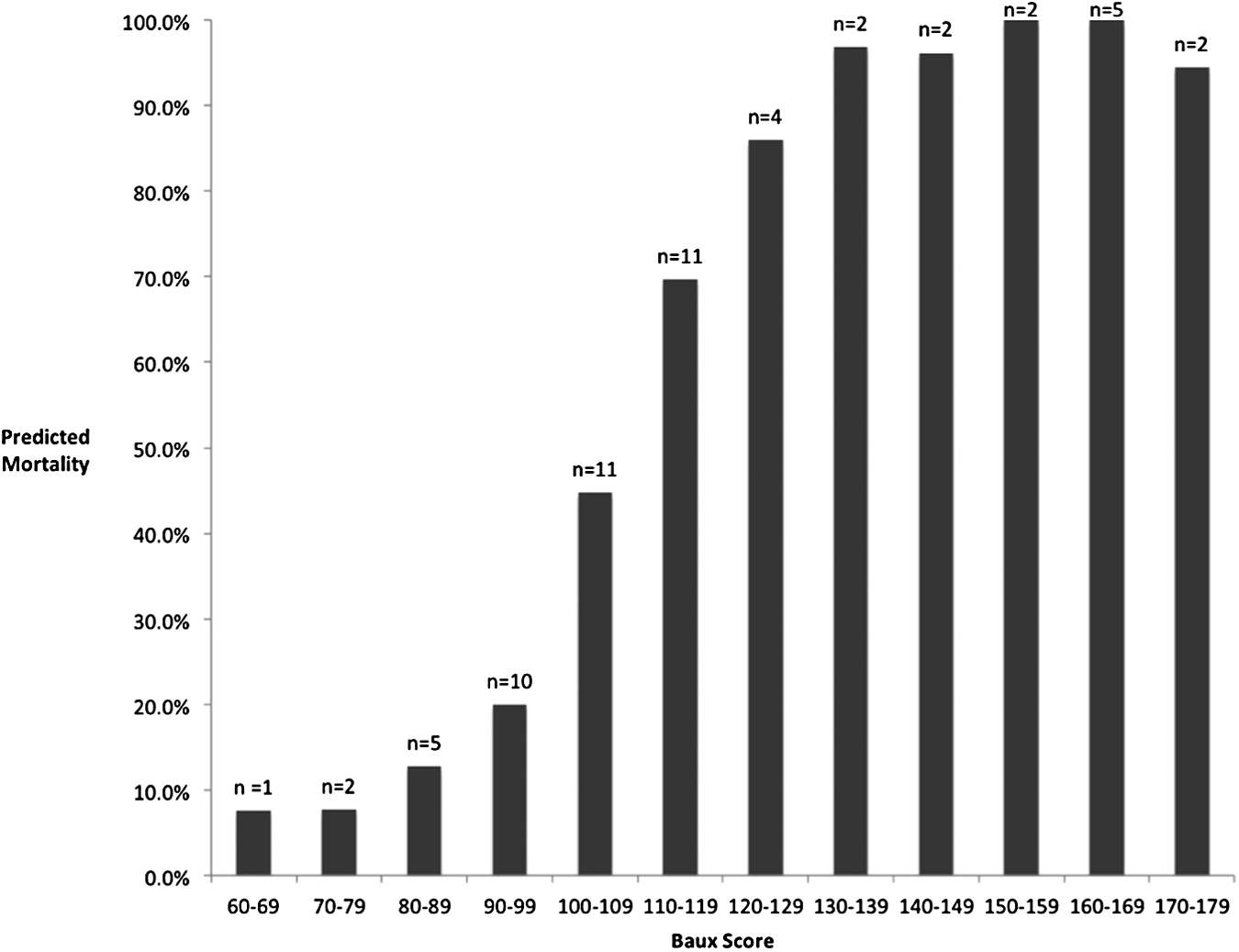
Mortality rates by deciles of Baux scores (i.e., sum of a subject's age and total body surface area burned).
Values are represented in mean ± standard deviation. Bolded values are statistically significant.
Demographically, the LATE group was found to have a significantly greater number of men than the EARLY group. Racial composition of the groups was similar, as were the rates of racial discordance between the burn attending physician of record and the patient/surrogate participating in the discussion. Preburn rates of frailty syndrome were also similar between the groups.
The EARLY group was found to be more severely injured, and rates of immediate decision by surrogates to opt for comfort care were similar between groups. The EARLY group died sooner after the first goals of care discussion than the LATE group (mean of 3.3 days vs. 8.9 days, respectively). Commensurate with this latter finding, only 3% of the EARLY group underwent one or more trips to the operating theater for burn excision and grafting, compared with 44% of subjects in the LATE group (p < 0.001).
Three subjects died without a documented discussion regarding code status or goals of care. A 79-year-old patient with a 30% TBSA burn (Baux score of 109) underwent aggressive burn resuscitation without a documented EoL discussion, despite an estimated risk of mortality during the index admission of 44.8%; this patient gradually decompensated and died with a full code status in place on hospital day 12. The second subject was an 86-year-old patient who was admitted with a 4% TBSA scald burn from spilled coffee. Despite the fact that the patient was clearly quite frail, the treating physician expected a reasonable chance of survival given the relatively minor injury burden. Consequently, no discussions regarding code status were initiated. The patient remained full code and was unexpectedly arrested on hospital day 5; resuscitation efforts were unsuccessful. The final subject was a 70-year-old patient who was admitted after sustaining full-thickness burns to 80% of his body (Baux score of 150, predicted in-hospital mortality of 100%). The burn team was unable to identify and contact family members despite exhaustive efforts. Based on the patient's medical condition and severity of injury, the attending physician felt that aggressive care would be futile. The patient was transitioned to comfort care measures 12 hours after injury and expired shortly thereafter; no family was ever located for this patient.
Discussion
In the setting of no set protocol for the initiation of EoL care for geri-burn patients admitted to our facility, the severity of injury appears to drive our burn surgeons' decisions to initiate a family discussion regarding goals of care for geri-burn patients. We were somewhat surprised to find that there was no association between the magnitude of injury and a decision by surrogate decision makers to proceed immediately with comfort care. Consequently, the finding that subjects having an EARLY discussion had fewer interventions before death appears to be an association with their significantly greater injury burden and, therefore, faster times to death rather than a causative factor in and of itself.
Our burn attending physicians' initial decision to begin the crystalloid resuscitation is a default to an aggressive strategy while patient surrogates are located. Before having an objective prognosis calculator, continuation of the crystalloid resuscitation in the absence of surrogates was driven by the attending physician's assessment of whether the clinical scenario constituted futility of care. Numerous observational studies in a variety of different local and national populations have identified age, percentage of TBSA burned, and presence of an inhalational injury as the primary risk factors for mortality after a severe burn.13–15 During the time period of this study, our burn surgeons appeared to be accurate in assessing these factors for each patient.
Swanson et al. reviewed the trajectories of death in burn patients in the National Burn Repository and demonstrated an asymptotic pattern of death in the elderly (defined as age greater than 55 years). 16 The majority of patients (55%) died within the first 72 hours, whereas 20% died after 72 hours but had evidence in the first 72 hours of early organ failure, and the last 25% of elderly patients survived the initial resuscitation but developed an acute deterioration in their health that was unexpected. Our findings are similar, as evidence suggesting a poor outcome was present in 70% of patients, whereas 30% of patients were believed to be likely to survive at the time of admission but later died due to complications. In our population, it appears that the magnitude of injury was the primary driver for burn clinicians in their prognostic assessment, as patients in the EARLY group were neither more frail than those in the LATE group nor more likely to have advance directives available at the time of admission.
Our group's initial interest in this project was driven by a new appreciation for the importance of providing quality EoL care. The Parkland burn group has energetically participated in the new national trend for quality improvement in multiple areas of clinical care. It is only recently, however, that we have come to consider EoL care as a domain that would also benefit from the evaluation of outcomes and quality measures. Unlike other measures in surgical critical care, however, the quality of EoL care is difficult to measure with traditional metrics due to the fact that life span may be shortened, not extended. 17 Quality geriatric EoL care implies implementation of a care plan that aligns with seniors' values and preferences, which, as shown in previous work, emphasizes comfort and quality of life to survival prolongation if prehospitalization function and independence cannot be restored.18–22 Unfortunately, for the majority of decisions regarding EoL care after a geri-burn, the patient is unable to voice their preferences and, unlike deaths occurring due to chronic illness, the sudden nature of thermal injury often results in surrogates' participating in EoL discussions without knowing their loved one's wishes. Indeed, in our study sample, less than 20% of patients had an advance directive in place at the time of admission.
Family members often express feelings of stress, anxiety, and depression when addressing EoL care, 23 and these negative feelings can be exacerbated by poor communication between physicians and family members regarding the care of their loved ones. When performed optimally, shared decision making for the establishment of goals of care takes into consideration: (1) a treatment plan that physicians feel is reasonable based on the patient's prognosis, (2) what the injured patient's wishes would likely be, and (3) what the patient's family members would consider quality care. However, it is important to note that each of these three contributors is necessarily subjective, which leads to the risk of poor communication between family members and providers. Indeed, factors reported in other studies that negatively influence a family member's perception of quality EoL care are largely centered around communication failures: receipt of contradictory information or lack of coordination of care, confusion over the identity of the primary physician, feelings of hostility or a lack of concern from physicians toward family members and/or the patient, and an increasing number of physicians involved in care.23–25
In contrast, EoL discussions that accurately convey information between the key stakeholders are characterized by perceptions of open, honest communication, as well as an increased frequency of communication, and communication that occurs early in the patient's hospital course. Such high-quality discussions often lead to greater concordance between the actual treatment plan and the family member's understanding of the treatment plan, as well as an increased likelihood of an early transition to comfort care measures. 26 Our results suggest that our burn surgeons' early communication and goal setting is typically driven by a lower probability of survival rather than a routine part of practice. We have identified this as a potential area of improvement for our care of the geri-burn population. Although we did not find that these earlier conversations about EoL care impacted the timing of decision making by surrogates, the patient and surrogate satisfaction scores found with early goal setting in these previously mentioned studies would seem to make this a worthwhile practice.
In an attempt to minimize variation, the Robert Wood Johnson Foundation (RWJF) Critical Care End-of-Life Peer Workgroup developed seven domains of quality of EoL care based on evidence in the literature and consensus approval. 27 These domains include shared decision making, improved communication among physicians and with family, continuity of care, symptom management, family spiritual support, and emotional support for care providers. Although these domains apply to quality markers in general medical populations, as mentioned earlier there are unique features of geri-burn care surrounding the timing of invasive interventions and we feel that our results suggest that a documented family meeting within the first 24 hours is a worthwhile target for further study. Other work that could inform the search for geri-burn quality EoL care markers has been done by Pham et al., who developed a protocol for EoL care after burn injury. 28 In this protocol, before the first family meeting, the nursing and physician staff caring for a severely burned patient performed an initial evaluation and arrived at a consensus regarding likelihood of survival and potential quality of life. If patients were considered unlikely to survive, surrogates were counseled as such and if comfort care was chosen by the decision maker, a standardized protocol with predefined EoL measures was set in motion. Through use of this protocol, the authors demonstrated better pain and sedation management, fewer deaths on ventilator, and increased utilization of bereavement support. Others have examined the inclusion of bereavement support pamphlets, early inclusion of palliative care members on daily rounds, and structured conferences with families, all of which have demonstrated improved concordance among families and physicians, less use of nonbeneficial interventions, and lower rates of emotional distress in families after death.29–31 Within these findings lie the elements for the future development of metrics for the delivery of quality EoL care.
Conclusion
Greater severity of injury prompts our burn surgeons to hold earlier discussions about code status and aggressiveness of care with surrogate decision makers of geri-burn patients. The early nature of this discussion and the greater magnitudes of injury do not, in turn, lead surrogates to decide on comfort care more quickly, however, and the significantly fewer interventions undergone by these patients is attributable to their dying more quickly as a consequence of their injury. Future work on metrics of quality EoL care for geri-burn patients should focus on surrogate satisfaction with the practice of performing a goal-setting conversation within 24 hours of admission.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
A version of this original work was presented at the 2016 annual meeting of the Trauma Association of Canada.