
Abstract

Dear Editor:
We experienced a case of unexpected sudden death that occurred during palliative radiotherapy for the terminal phase of childhood cancer.
The patient in the abovementioned case was an 18-year-old boy who had been diagnosed with osteosarcoma of the right femur at the age of 12 years. Four years after remission of the osteosarcoma, a lung metastasis was found. Despite the remission induction therapy, it progressed to multiple bone metastases. He received palliative chemotherapy and fentanyl patch, which failed to control his pain. Although the pain resolved transiently after the administration of Strontium-89 (85.5 MBq/body), he presented his complaints of left-sided lumbago and high grade fever eight weeks before his death. The results of cardiac and pulmonary function tests were within normal ranges. A computed tomography scan showed an iliac bone and lung metastases. At this point, embolic lesions were not observed in lung or inferior vena cava (IVC). Palliative radiotherapy for the pelvic bone metastatic region (3 Gy/session, nine sessions) was started. On the 11th day from starting radiotherapy, he took breakfast without having nausea or vomiting and interacted with the nursing staff as usual. Then, he suffered a sudden cardiopulmonary arrest. Immediate cardiopulmonary resuscitation failed to revive him. Peripheral blood examination at that time revealed many clusters of large cells (Fig. 1A), which were negative for leukocyte common antigen (Fig. 1B). The cells were found to be osteoblastic tumor cells morphologically. Although we could not confirm the cause of his sudden death by autopsy or by autopsy imaging because we could not obtain an agreement for them from his family, it was suggested that the tumor cells spread through the blood stream and caused systemic embolization.
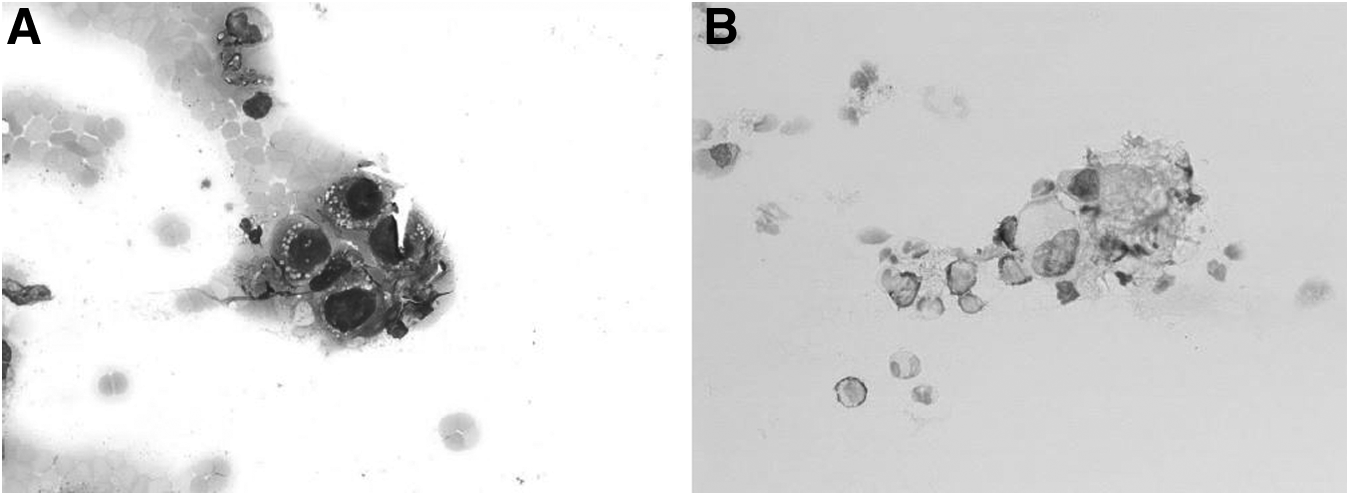
Peripheral blood examination revealed many clusters of large cells, it was confirmed that these large cells were osteoblastic cells morphologically
Thromboembolic events often occur in cancer patients. 1 In a previous report, 2% of patients with soft tissue or bone sarcomas were accompanied by intravascular thrombi, which was associated with poor prognosis. 2 In contrast, osteosarcoma with an extensive tumor thrombus is very rare. A review of the literature reveals 15 cases of tumor thrombus arising from osteosarcoma; the first case was reported in 1957 and the latest in 2013. 3 Tumor thrombus was mostly incidentally found during the period of assessing the stage of the disease by diagnostic imaging. In almost all cases, the site of tumor thrombus was the pulmonary artery or IVC, and survival time from the diagnosis of thrombus ranged from less than 1 month to 13 months. There was no case of sudden death by tumor thrombus among these 15 cases.
Osteosarcoma most frequently metastasizes to lung and bone. In contrast, it was suggested that tumor cells spread through the blood stream and caused systemic thrombus in this case. It is possible that radiation leads to the fragmentation of the tumor, which migrated in the bloodstream. We should be aware of this possibility even during palliative radiotherapy for terminal cancer patients. In addition, the pathophysiology of this condition that was triggered by radiotherapy should be clarified.