
Abstract
Abstract
Background:
Seriously ill older adults in the emergency department (ED) may benefit from palliative care referral, yet little is known about how to identify these patients.
Objectives:
To assess the performance and determine the acceptability of a content-validated palliative care screening tool.
Design:
We surveyed Emergency Medicine (EM) attending physicians at the end of their shifts using the screening tool and asked them to retrospectively apply it to all patients ≥65 years whom they had cared for. We conducted the survey for three consecutive weeks in October 2015.
Setting/Subjects:
EM attending physicians at an urban, university-affiliated ED.
Measurement:
Patient characteristics, acceptability rating, and time per patient screened.
Results:
We approached 38 attending physicians to apply the screening tool for 69 eligible shifts. Physicians agreed to participate during 55 shifts (80%) and screened 207 patients. On 14 shifts (20%), physicians declined to participate. Mean age of the screened patients was 75 years, 51% were male, and 45% had at least one life-limiting illness. Overall, 67 patients (32%) screened positive for palliative care needs. Seventy percent of physicians (n = 33) found the screening tool acceptable to use and the average time of completion was 1.8 minutes per patient screened.
Conclusion:
A rapid screen of older adults for palliative care needs was acceptable to a majority of EM physicians and identified a significant number of patients who may benefit from palliative care referral. Further research is needed to improve acceptability and determine the appropriate care pathway for patients with palliative care needs.
Introduction
T
To address this gap, George et al. convened a panel of palliative care experts and used a modified Delphi technique to develop a content-validated tool to screen patients for palliative care needs in the ED (Fig. 1). This tool combines clinician's overall assessment and the validated prognostic question “Would you be surprised if this patient died in the next 12 months?”13,14 to screen patients for palliative care needs. 15 Although the acceptability among physicians of this tool has been demonstrated in hypothetical case vignettes, 16 the acceptability and feasibility in the ED settings are unknown. Our objective was to test the acceptability of this tool in an urban, academic ED and characterize actual older adults identified as having palliative care needs.

Content-validated palliative care screening tool in the ED (reproduced with permission from the publisher). ED, emergency department.
Materials and Methods
Study design
The study was conducted at an academic, urban ED with an annual volume of 60,000 visits, 24% by adults aged ≥65 years. One hour before the end of each shift, a research assistant (RA) asked EM attending physicians to apply the screening tool to all patients ≥65 years whom they had cared for during that shift. Physicians were also asked to report the time taken to complete the tool and its acceptability before they left their shifts.
We included all attending physicians who cared for at least one patient aged ≥65 years during 7 AM to 4 PM shifts, 12 PM to 9 PM shifts, or 11 PM to 8 AM shifts every day for three consecutive weeks in October 2015. We excluded physicians who were unable or unwilling to participate, as well as shifts when the RA was physically unavailable. The study protocol was approved by the institutional review board.
Measures
EM attending physicians administered the screening tool (Fig. 1). They also responded to questions that rated the tool's acceptability (unacceptable, somewhat unacceptable, neutral, somewhat acceptable, and acceptable) and level of confidence in the information they used when completing the tool (5 point scale: 1—not confident, 3—neutral, 5—extremely confident).
After the ED screening, an RA trained on how to identify life-limiting illnesses in the electronic health record (EHR) reviewed the medical records of all patients screened to abstract data elements included in the screening tool using a standard method 17 (e.g., “Does this patient have advanced cancer?”). The RA was blinded to the physician survey results. Data were abstracted using the Research Electronic Data Capture database (REDCap). 18 To determine the quality of chart abstraction, the PI (K.O.) independently reabstracted data from 10% of patient medical records.
Analysis
To compare the overall clinical assessments for palliative care needs of patients who screened positive or negative, we used two-sample test of proportions. We used McNemar's test to compare the life-limiting illnesses reported by physicians with the same information abstracted from the EHR. To demonstrate the inter-rater agreement of the chart abstraction by the RA and PI, we used proportion of agreement rather than kappa coefficient because of high concordance, resulting in paradoxical kappa from unbalanced marginal totals. 19 We used p < 0.05 for statistical significance.
Results
There were 69 eligible ED shifts during our study period. Thirty-eight physicians provided care to more than one patient ≥65 years during these shifts. A survey was completed during 55 shifts (80%) and physicians declined to participate during 14 shifts (20%). Overall, 33 physicians (86%) participated. On average, physicians had been in practice for 9.2 years and 67% were male. These 33 physicians screened 207 patients with a mean of 2.8 patients screened per shift (SD 2.5). The mean patient age was 75 years (SD 7.5), 51% were male, and 44% had at least one life-limiting illness (Table 1).
CHF, congestive heart failure; CNS, central nervous system; COPD, chronic obstructive pulmonary disease; ED, emergency department.
Sixty-two patients (33%) screened positive for palliative care needs. Forty-eight of these patients (77%) were admitted. For 55 of the patients who screened positive (83%), the physicians stated that they “would not be surprised” if the patient died in the next 12 months. The majority of physicians (n = 23, 70%) found the use of the screening tool “acceptable” or “somewhat acceptable,” and the average time spent was 1.8 minutes per patient screened (SD 1.3) (Table 3). The majority of physicians (n = 27, 82%) reported being “extremely confident” or “somewhat confident” about the clinical information they provided.
When compared with patients who screened negative, patients who screened positive were perceived by the physicians to have higher proportions of frequent recent ED visits (79% vs. 24%, p < 0.0001), uncontrolled, distressful symptoms (57% vs. 7%, p < 0.0001), functional decline (59% vs. 19%, p < 0.0001), uncertainty about goals of care (17% vs. 4%, p = 0.0019), and more clinicians would not be surprised if the patient died in the next 12 months (85% vs. 35%, p < 0.0001) (Table 2). Physician statements about patient life-limiting illnesses were less complete than documentation found in the EHR for CHF (p = 0.046). There was a nonstatistically significant trend in other conditions (Fig. 2). There was 90% agreement in chart abstracted data between the RA and PI.
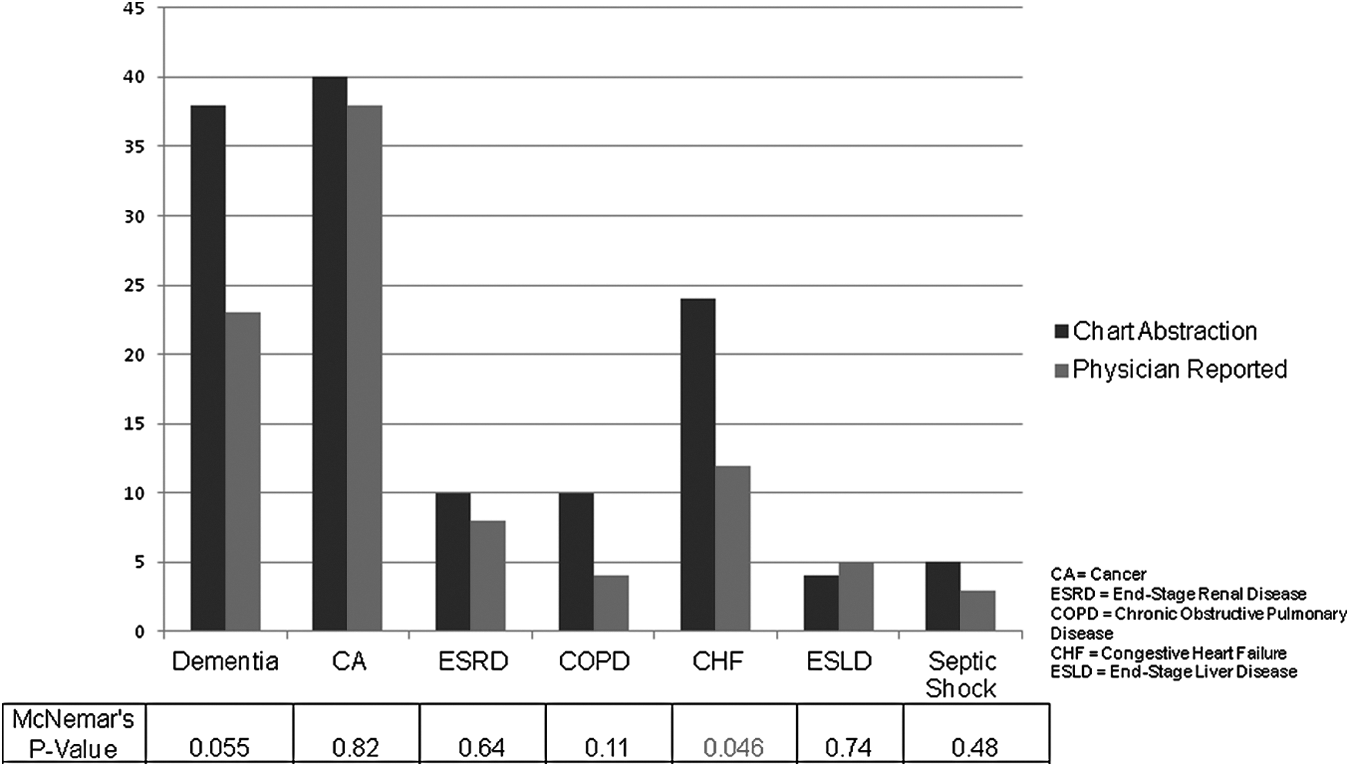
Accuracy of life-limiting illness information based on physicians' report compared with chart abstraction.
The same palliative care needs assessment questions were asked for patients who did not screen in at step 1 as well.
Discussion
We tested an expert panel-generated palliative care screening tool administered by EM attending physicians in a consecutive sample of older adults cared for in an urban academic ED. We found that the tool was generally acceptable to attending physicians. It demonstrated that one-third of patients screened might benefit from palliative care services. The short administration time (1.8 minutes per patient screened) makes this tool attractive for wider dissemination and testing. Furthermore, our study confirmed the feasibility and reliability of such screening on actual ED patients instead of hypothetical case vignettes. 16
Few studies have examined the incidence of patients with palliative care needs in the ED. 20 Those that have found a high rate of ED presentations among patients with nonsmall cell lung cancer, 21 and that over half of older adults with functional impairment who presented to the ED 22 had palliative care needs.
Our finding that the number of most life-limiting illnesses identified through chart abstraction in these patients was not statistically different from the physicians' report raises the possibility that these life-limiting illnesses could be automatically elicited from the EHR (Fig. 2), further reducing physician burden. This type of staged screening process is also supported by a recent review that found that such tiered screenings seem to capture more patients than a screening relying solely on physicians. 12
Limitations
There were several limitations to this study. We collected data on consecutive shifts, but 14 out of 69 shifts attempted were incomplete because of physician refusal. The response rate was adequate for internal validity (86%, 33 out of 38 eligible physicians), but may not reflect what the use of this tool would be in other settings. Our sampling strategy also did not allow us to screen the total number of patients ≥65 years seen in the ED. We can only estimate that 32% of older adults seen by EM attending physicians at our institution have palliative care needs. In addition, there is not an agreed-upon criterion standard for “palliative care eligibility” 23 ; hence, it is difficult to characterize the sensitivity and specificity of the screening tool. Other clinically useful means to identify ED patients with palliative care needs and specific care pathways for such patients must be further defined to meet the needs of the ED patients. Lastly, we followed recommended practices for chart abstraction, 17 yet there was a 10% disagreement between the abstracters. Finally, the high rate of older adults with cancer seen at our ED (44%) results from its affiliation with a major cancer center; thus, this rate may not be generalizable to other settings.
Conclusion
Screening older adults for palliative care needs in the ED with a structured tool is acceptable to a majority of EM physicians and identifies a significant number of patients who may benefit from palliative care referral. This tool may require modification to increase physician acceptability before wider dissemination. Further research is warranted to determine the clinical significance and appropriate care pathway for patients who screen positive for palliative care needs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.