
Abstract
Abstract
Background:
Increasing longevity for Inuit living in Nunavik, northern Quebec, has resulted in heightened rates of cancers and chronic diseases necessitating complex treatments. Consequently, end-of-life (EOL) care, once the domain of Inuit families and communities, has come to include professionalized healthcare providers with varying degrees of awareness of factors to consider in providing care to Inuit populations.
Objective:
To better understand the factors shaping EOL care in Nunavik to support the development of a sustainable model of care.
Methods:
Using focused ethnography, we conducted participant observations and informal and semistructured interviews with 103 participants (community members, healthcare practitioners, and administrators) across Nunavik and in Montreal, the affiliated tertiary care center. Data domains included the following: care trajectories; patient and family experiences receiving and providing EOL care; local and urban resources and challenges; and ways forward.
Results:
Sociocultural, historical, and geographic factors shape EOL care in Nunavik, presenting a complex set of challenges for Inuit patients, families, and healthcare providers. A sustainable model of EOL care requires building on shared initiatives, capitalizing on the existing strengths in communities, and attending to the multiple bereavement needs in the region.
Discussion:
Building a sustainable model of EOL care requires respectful collaboration among governing structures, healthcare institutions, and community members. It must centrally value local knowledge and initiatives. To ensure Inuit families and patients are supported throughout the dying process, future initiatives must centrally include local stakeholders in both the design and evaluation of any changes to the current healthcare system.
Introduction
I

Map Nunavik.
In Canada's Indigenous communities, efforts are being made to reduce the legacy of colonialism in health planning. 5 Referencing end-of-life (EOL) care, researchers have underlined the need for a “bottom-up” inclusive approach in which community specifics and cultural realities are incorporated into local Indigenous EOL policy and programming.6,7 Addressing palliative care needs of Indigenous peoples, Castleden et al. 8 emphasized the importance of care-giving environments that do not repeat historical patterns of forced institutionalizations, and in which training is focused on local cultural practices in death and dying. The success of the Helping Hands program in Alaskan remote communities, a program built on the capacities of community volunteers working in collaboration with health institutions, had a significant impact on meeting the wishes of patients to die in their homes. Within a four-year period, the percentage of patients dying in their homes from cancer, chronic obstructive pulmonary disease, congestive heart failure, or renal disease increased from 33% to 77%. 9
Changing morbidity rates and life expectancies necessitated a reexamination of practices and policies for EOL care in Nunavik as Northern communities and health centers were able to address the needs of the increasing numbers of elders and patients with complex illnesses nearing the EOL. Upon the invitation of local health administration concerned with the changing demographics and rising EOL care needs, this study was designed to identify key factors shaping historical and current care provision with the goal of contributing knowledge to future initiatives by local municipalities and health institutions as they engage in the development of a sustainable model of EOL care services.
Methods
Recognizing that Inuit in Nunavik have been providing EOL care to community members since long before local healthcare centers were established, we used a community capacity theoretical perspective to orient this study.10,11 Identifying existing community strengths through this approach is one means through which palliative care programs have been developed in remote regions in Canada. 12 We used this approach to identify and appreciate the measures that families and communities historically have used to provide EOL care in Nunavik. This appreciation then served as a foundation upon which to imagine how current and future innovations and collaborations could extend from these existing capacities.
Given the importance of understanding how the sociocultural context affects care practices, we used a focused ethnographic methodology. 13 Focused ethnography is a qualitative methodology from the anthropological tradition; it uses participant observation and interviewing to study health phenomena embedded in complex cultural and historical processes. It is particularly useful for within tight-knit communities. 14 Our ethnographic methods included field visits over a 12-month period between 2014 and 2015 during which we conducted observations (e.g., community events, family visits, churches, health centers, elders homes, hospitals, home care nursing rounds, and funeral practices), and informal as well as semistructured interviews in individual and group formats. Interviews were conducted by the first author. Interview domains were created deductively from a review of current literature. 15 The interview guide was pilot tested with stakeholders and adjusted. Additional domains were added inductively as the study progressed (e.g., euthanasia). We contextualized the interview data with information from health reports, documentaries, news sources (e.g., Nunatsiaq online, a popular local source), books, art, museum exhibitions, and academic articles.
Field visit durations ranged from 1 to 6 weeks for a total of 14 weeks onsite. We also conducted onsite interviews in the urban hospital center in Montreal that receives Nunavik patients with complex needs; these participants were recruited through snowball sampling and included nurses, physicians, social workers, interpreters, and spiritual advisors. Interviews and field notes were coded and analyzed using NVIVO software. Major analytic domains included the following: geography (e.g., community health centers, centralized institutions, and homecare contexts); care trajectories; experiences of, and local resources for, care; strengths and challenges in care provision; and ways forward. The Institutional Review Board at McGill University and the board of directors overseeing the health centers in Nunavik formally approved our project. We obtained permission from leaders of local community organizations and institutions to enable entry and data collection in Nunavik communities.
Findings
The Inuit have a long tradition of providing EOL care to the dying. Current sociocultural, geographic, medical, and structural realities have impacted those traditions. Families and medical professionals reported that many patients are no longer dying in community settings and instead are dying in centralized hospitals in Nunavik, or in tertiary care facilities in Montreal. Family and community members often have limited access to these patients once in these distant centers. The findings from this study identify the key contextual factors in which EOL care is currently provided to Inuit patients, and theorize their complex interrelationships. If patient's and family's wishes are to be taken into account, we suggest that these factors must be integrated into future care models.
In total, we spoke with 103 participants in the context of health centers, schools, municipal offices, family homes, churches, and community organizations (Table 1). Participants were from the four Nunavik communities with the largest aging populations as well as from Montreal. They were recruited through snowball sampling in schools, municipal offices, churches, elder's homes, and health centers. Some of nurses and physicians with whom we spoke worked as part of a rotating team providing EOL care in Nunavik's smaller communities. Others encountered these patients and families in the context of care in Montreal. We drew on accounts of their experiences in providing EOL care to patients and families from these settings as well. EOL care was offered by family members, community volunteers, and paid healthcare professionals. Experience varied from 2 to 20 years of working alongside Inuit patients requiring EOL care.
Then and now: Contextual factors in Inuit EOL caregiving values and traditions
The Inuit practice (of caregiving) is very strong. If you care for that person and the passing of life, your heart is going to be peaceful. If you don't care for the person, your heart is going to suffer (Inuit elder).
Evidence of nomadic Inuit communities in Nunavik dates back to 2000 BC. 16 The shift to a sedentary development began with European quests for furs in the early 1700s,17,18 followed by missionaries seeking to convert Inuit populations in the early 1800s, 18 and Canada's quest for sovereignty of Arctic lands in the early 1900s.17,19,20 Starting in the 1940s, resettlement processes were formalized by the federal government 21 : Inuit were forced to adopt village-based communities, compelled by federal policies such as the slaughter of sled dogs, which were essential for nomadic survival, 22 and the practice of compensating families with food and clothing only if they were living in settlements. Policies associated with resettlement resulted in a legacy of mistrust that remains today. 23
Inuit participants recounted to us an oral history of rich caregiving traditions in which the sick and elderly were collectively cared for by family and clans who shared social responsibilities (e.g., child-rearing, the search for food and shelter, and the making of tools and clothing). When clan size and general wellbeing permitted, the nomadic clans would reorganize themselves so that caregivers could temporarily settle to provide care for the sick and dying. This care tradition was disrupted when epidemics of small pox and tuberculosis brought by early European settlers and traders wiped out entire families and clans.18,20 Furthermore, in the 1950s, family members who were diagnosed with tuberculosis were forcibly hospitalized in sanatoriums in the South. 24 Those who died were buried in the South, at times without families being contacted about the death or burial place. 19 Forced displacement of Inuit children in federal residential schools starting in 1950s and continuing until the 1970s had a long-term impact on the continuation of traditional Inuit healthcare practices. When children were separated from family homes and communities, these teachings could not be passed down to them. 25
Today, ∼11,000 Inuit live in Nunavik (Fig. 1). 2 They reside in 14 coastal communities accessible to each other only by plane. Despite the profound disruptions caused by colonial policies, many communal caregiving practices remain evident today. Participants told us that dying patients usually wish to die at home in their community.
When this is possible, during the final stages of the dying process, homes are filled with family and friends of all ages. Participants described that as adults and children are present, this accompaniment may include conversation, song, silence, prayer, games, storytelling, laughter, sharing of food, and assistance with the activities of daily life. At EOL, food preparation, housecleaning, mortician services, and funeral preparations are shared among family members, members of faith-based women's auxiliaries, and others close to the patient or family. Family members may also work alongside of nurses and physicians to provide direct care. In addition, the community-run hunter's support group and the local cooperative store supply families with food as needed. Notably, the local cooperative movement has been key in bringing some degree of economic stability and autonomy to communities26,27 and participants told us that local stores provide resources such as food baskets to families during and after the death of a family member.
Current living conditions, however, are not always amenable to EOL care provision. Living conditions in Nunavik are marked by disparities in education, income, and housing 28 with 42% of Nunavik homes officially declared unsuitable for living. 26 Furthermore, health institutions in Nunavik have a history of disregarding interventions and traditional Inuit cultural values. 18 Our participants indicated that gaps in collaboration remain between those working in institutions and those engaging in traditional care practices.
Several factors are essential to understanding the current EOL context in Nunavik, including religion and language. European missionary influences have had a significant impact on religious practices and rituals. This influence is present in the prayers and scripture reading accompanying patients at the EOL, beliefs concerning whether or not to communicate terminal diagnoses, beliefs about death and the afterlife, and funeral preparation. The majority of Nunavik residents (94%) identify an affiliation with the Anglican faith,2,29 a church that had historically been active in building places of worship, providing material aid, and establishing residential schools. 30 Each community has an Inuit-trained Christian pastor who conducts funeral services rooted in European missionary traditions, including hymns, prayers, scriptures, and burial. Participants stated that pre-Christian grief and burial traditions were evidenced in archeological sites, although were no longer present in communities.
Another important local influence on EOL care is language: 95% of local residents speak Inuktitut as their primary language with English a common second language for those younger than 40 years, with a few speaking French. 2 This contrasts the licensed healthcare providers whose primary language is French, although many speak some English. 2 Nurse and physician positions require a postsecondary education that can only be obtained outside of Nunavik and as French language competence is required by Quebec licensing bodies. We were told that two local Nunavik residents practice nursing, both of whom were participants in a time-limited local training initiative offered several years ago. All other formally educated healthcare professionals in Nunavik are non-Inuit, from southern urban centers.
Sociogeographic locations of care and associated challenges
EOL care in Nunavik is currently offered in three sociogeographic locations: homes, local healthcare centers in Nunavik, and centralized hospital centers in Montreal. Each location is important for the development of an integrated approach to EOL care, yet each has its own strengths and challenges, as follows:
EOL care in home and community contexts
I'm sick again. I want to be able to die at my house. I don't want to be stuck in the hospital, being fed by and trying to be kept [alive] by, equipment… I know I'm going… we are all going to die. So I would like to die at my house. (Daughter's account of father's words)
There is a belief that you have to take care of your family. What is in the home stays home and shouldn't really be going out. So even though they [family members] are ‘burning out,’ they don't reach out for help (Family member).
Family members and healthcare providers reported that most persons wished to die in their home communities, surrounded by families and friends. Stories were told of elders who died in the community without requiring medical intervention and who refused treatment rather than be placed in a hospital center away from home. For those who required medical intervention, had been hospitalized, and wished to receive care or die at home, wishes were accommodated where possible. Arrangements were made by home care social workers, nurse and physicians for dying patients to return home with an explicit palliative care protocol. Extra nurses were flown into communities when personnel resources were already overextended or when home care nurses were not on site. Families were provided with the beds and other physical materials necessary to provide care. Exceptions included patients whose care had deteriorated to such a degree that a return home was not feasible, or patients who did not have adequate family and community care in place.
Healthcare providers and family members described how in certain communities, family-based caregiving practices were declining. They felt that while families believed that they should care for patients at home, members were often unable to commit to this process. They attributed this decline to five main factors: (1) some families who wanted to provide EOL care became overwhelmed by the daily expectations related to care-time demands combined with lack of emotional reserves and physical support. They were hesitant to ask those outside of the family for help. (2) The introduction of television and Internet resulted in reduced informal social interactions upon which the collective approach to EOL care had been founded. (3) Knowledge concerning EOL care was not always successfully transmitted from one generation to the next, leaving family members uncertain as to how to prepare for or to support the dying process. (4) Intergenerational trauma rooted in colonial practices resulted in social suffering, which manifested through substance abuse, suicide, accidental deaths, or child abuse and neglect. Participants stated that when family members had not received adequate psychosocial care, the dying process of loved ones aggravated these memories. Community members and nurses expressed concern over the lack of both mental health and bereavement services for Nunavik children and adults. (5) Increased formal employment opportunities with fixed hours and travel commitments meant that family members could not always reorganize themselves to provide care as they had in the past.
EOL care in local institutions
Each of Nunavik's 14 communities has a health clinic staffed around the clock by a minimum of two nurses onsite during the day and on call evenings and weekends. Twelve of these clinics do not have mandates to support in-patient care. Communities with populations over 900 have a physician located onsite; otherwise physicians are flown in monthly. Other medical specialists (e.g., pulmonologist and psychiatrist) circulate in the communities four times per year when possible. The 14 communities divide into two coastal regions, Hudson on the west and Ungava on the east, with 7 communities each. There is one acute in-patient hospital center per coastal region. Each of these in-patient centers has two beds for palliative/EOL care although often more beds are used for these purposes. There is also one 12-bed in-patient facility in the Ungava region for adults with disabilities and chronic medical conditions, including elders with dementia.
EOL care in southern institutions
Patients with complex treatment needs beyond what can be accommodated in Nunavik are flown to acute and long-term center in Montreal, upwards of 2000 km away. Given the shortage of beds in Montreal, long-term patients are required to return to the local in-patient centers, who are often themselves faced with overcrowding. Patients often find themselves rotating between home, Nunavik in-patient hospital centers, and Montreal hospital centers.
In a typical scenario, a patient will come to their local health clinic where a nurse or, if present, a physician will conduct an initial assessment. If further evaluation or treatment is needed, the patient will be referred to their coastal in-patient health center or, if needed, to Montreal. EOL care planning is set into motion if the treating physician declares there are no interventions to reduce or halt the imminent and terminal progression of the illness, or if the patient refuses medical interventions (e.g., a patient who chooses to return to their community rather than seek cancer treatments or kidney dialysis). The location in which EOL care could be provided is determined by several factors, including the following: the potential medical complications and the capacity for families and communities to deal with these; whether there is a palliative care protocol in place for the patient; whether there are adequate numbers of family members and healthcare professionals available to provide the care; whether there are beds available in a Nunavik in-patient health centers; and/or whether the patient can tolerate air transportation back to their community.
Difficulties in delivering care are compounded by workforce issues. Liaison nurses, pivot nurses, interpreters, and social workers, in both Montreal and across Nunavik, work to assist patients in negotiating the healthcare network. Nurses described how the consequences of high staff turnover rates and being understaffed impacted the timeliness of care and adequate patient support. In addition, liaison nurses were increasingly presented with comorbidities requiring complex care, placing growing demands on their time in setting up appointments and providing follow-up care. Communication challenges also impacted how care unfolded. Interpreter services were needed for the affectively laden and informationally loaded EOL care conversations with Inuit patients and families, although healthcare providers and interpreters stated they were lacking in training of how to best work together.
Sociocultural factors in care and associated challenges
Each time we are here (in Nunavik), we push limits to exhaustion, physical and mental… you have to be really balanced and really well with yourself (Nurse).
Here we do it with what we can, but have a ‘criminal’ lack of support for the family (Nurse).
Qallunaat is a term meaning “white people” and is locally designated for non-Inuit medical staff living in Canada's circumpolar regions. Qallunaat described for us experiencing varying degrees of acceptance in the northern communities, feeling that they always remained “outsiders” regardless of the length of their time in the region. Before arriving, nurses and physicians receive only two days training: one day on Inuit culture and the second on preparing for life in an Artic context. They told us that this training portrayed an idealized version of Nunavik and its people. On-site training focused on whatever was urgent, for example, provision of acute medical care. Many felt unprepared for the cultural and social realities in which they found themselves.
Turnover rates for nurses in Nunavik are high, many remaining for one or two years or less. As newcomer nurses had minimal prior knowledge of cultural communication models and local daily traditions, they had to learn these elements by trial and error, thus making many mistakes along the way. Nurses described how interpreters were key to providing the contextual factors, essential in filling in knowledge gaps concerning cultural communication norms and local traditions. Interpreters stated that this additional “informal” expectation could be fatiguing as they were regularly intervening to avert potential errors, which could have significant effects on patient–provider relationships. Each time a new nurse arrived without adequate background, the interpreters needed to begin this “training” anew.
Nurses and physicians often had no specialty training in meeting the physical and emotional needs of palliative patients as emergency and pediatric medical skills are in much higher demand in the north. Many nurses spoke of the burden of physical and emotional care that they assumed in working with patients and families. Few mental health services, and the lack of local informal and formal family supports, meant that nurses were expected to respond to emotional suffering. Nurses often felt pushed to their limits. As one nurse commented, “Just because we are given many hats to wear, it does not mean that we are capable of assuming all of them.”
The importance of trust between patients and care providers
What they (family) came away with… was the sense that I was a disrespectful white doctor who wanted to ‘pull the plug’ on their family member rather than providing him with the best possible care, because there's a lot of mistrust there. (Physician)
My father says that it was the morphine that killed his uncle. (Family member)
The first thing you need to treat is to treat the person spiritually and mentally instead of with pills. (Nurse)
In light of the sociocultural and historical context in which institutional care is provided in Nunavik, and the minimal cultural training offered to healthcare providers, it is not surprising that trust emerged as central in our findings. Physicians, nurses, and social workers described lacking opportunities to engage with communities outside of their work context. Participants, both Inuit and Qallunaat, expressed concern regarding the unseen impact of colonial practices that resided in the collective memories of families and how traces of these practices remained in service delivery. Consequently, errors in communication were made, often unintentional and unrecognized, which potentially led to breakdown in trust. Examples of Qallunaat social workers arriving uninvited to the home of a grieving family, of an interpreter required to work when a family member had died, of country food not permitted in health center premises, of community members not given space to wash the body of the deceased or, these and other breakdowns in communication were described as avoidable with adequate training.
Prior trust relationships with family members were key to success in EOL care decision making. A physician described her attempts to explain to a family that she had just met that it was in a patient's best interests to remove life support. These comments were perceived by the family as the physician's desire to prematurely end the patient's life. This mistrust surfaced in several conversations with family members for whom the physicians intent concerning the prescribing of morphine had come into question; the physician's choice to prescribe morphine at the EOL was interpreted as hastening—if not actually causing—the death of the patients.
These accounts contrasted with successful experiences with family meetings concerning EOL care; for example, by physicians who had worked with the same patient over several months, by spiritual care advisors whose role consisted of building trust, and by home care providers who saw their patients over time. A nurse told us that after three years, she finally felt welcome in the homes of patients. Having worked previously in Indigenous community contexts, she had the patience and determination to wait until families were ready to receive her. She became a strong advocate for her patients, seeking funding to develop additional programs such as public meeting places for elders, transportation, and exercise programs. To do so, she frequently worked beyond her shift. Her care and respect for patients resulted in public acts of appreciation by families.
Development of sustainable EOL care
Figure 2 outlines what participants identified as important elements for the development of a sustainable program of EOL care for both community and institutional settings. Participants agreed that both Inuit and Qallunaat had the combined expertise, knowledge, and resources necessary to develop a program attentive to the increasing numbers of patients requiring EOL care. In family contexts, recommendations centered on education concerning disease progression, care provision, and the dying process. Respite services were singled out as needed for families, and it was suggested they could be provided through collaborative efforts of municipalities and health centers. Key also were resources allocated for communities to provide culturally informed psychosocial and bereavement supports to their members, many of whom were suffering under the weight of unresolved grief related to histories of traumatic experience in their families. In terms of institutional care, emphasis was placed on palliative care training (including psychosocial support), facilities, increased staff, and specialized training for interpreters.
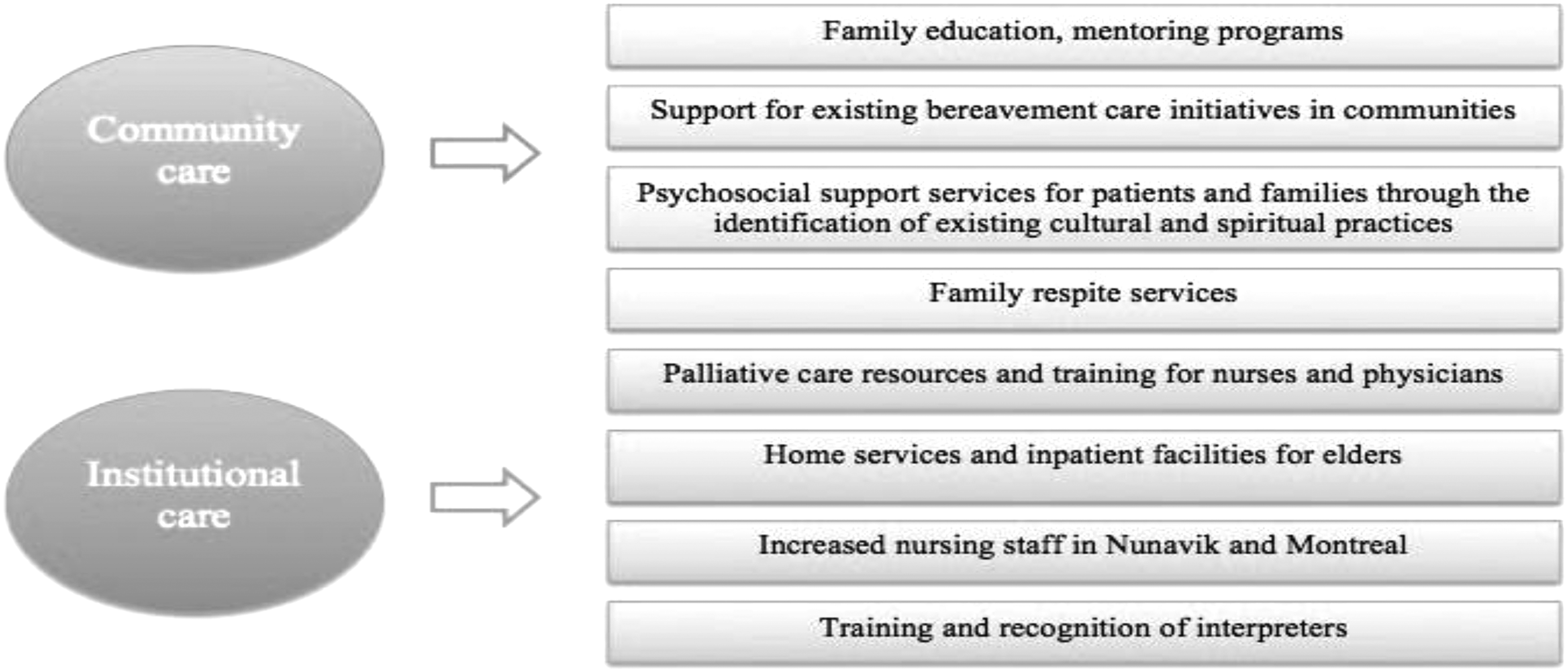
Moving forward, end-of-life care in Nunavik.
Discussion
Researchers working to develop EOL care programs in Indigenous communities in Canada favor an approach in which communities are engaged with institutional care providers in developing services specific to their populations, and these services are built upon existing capacities in communities.31–34 Although we focused on larger communities in our studies, physicians and nurses who worked with patients in smaller communities indicated that both challenges and solutions are similar. Our findings indicate that three preconditions are necessary for moving forward in Nunavik. First, provide adequate training for healthcare concerning the historical, social, and cultural realities that underlie relationships between Qallunaat and Inuit alongside of culturally informed palliative care materials and mentors; second, equip communities to build on existing practices that address the suffering in families (as grief and other psychosocial issues are addressed, family caregiving capacity will increase); and third, invite communities to identify sources of knowledge that inform their EOL care practices. Below we offer some recommendations concerning how this may be accomplished.
Trust building in community collaborations
Trust and confidence in the nurses and physicians were necessary conditions for Inuit patients and families to open up to healthcare providers. This reality has been noted in other EOL studies.35–37 Nurses and physicians were at times perplexed and confused by the difficulties they had to attain this trust. Macaulay 5 provides insight into this question in stating that the promotion of Indigenous health includes advocating for multidisciplinary teams, increased Indigenous control over health programs, and funding support for collaborations in healthcare. In Inuit contexts, this includes local training options adapted to Inuit realities. 38
Adequate professional cultural training to Qallunaat before arriving in Nunavik is essential, including actual accounts of the challenges faced and successful strategies by Qallunaat and Inuit in building trusting relationships. This training may potentially reduce risk of errors in communication leading to breakdowns in trust, some of which are described in the literature as “microaggressions.” 39 Microaggressions are “banal and unintentional practices of the dominant group members,” who intend no malice and although are perceived as racist by the minority group. 40 These errors and their consequences may be distressing for both groups. During the writing of this article, we spoke with an Inuk woman who described a community in a neighboring region who coordinated “culture days” for employees. Organized by healthcare centers and local municipalities, Qallunaat are released from work obligations and invited to learn about Inuit history, customs, and practices through outings with local Inuit guides. In addition to being educative, such events may also reduce the degree of alienation that Qallunaat feel when working in communities and allow Inuit to be sensitized to the challenges faced by nurses and physicians working in remote communities where they are dealing with geographic isolation and adapting to an unfamiliar cultural environment.
Social suffering and bereavement needs
The theory of social suffering invites us to examine how political, economic, and institutional power may inflict adversity on individuals as well as groups. 41 As was reiterated by participants throughout our study, Inuit families have suffered from epidemics, starvation, loss of livelihood, and disrupted relationships directly resulting from colonial policies and structures. 18 Inuit in Nunavik live daily with the consequences of this history, some coping in ways that actually multiply this suffering.
Many researchers have highlighted the importance of physical and mental health support for patients and families at EOL.35,42,43 In Nunavik, this need goes beyond individual forms of health to addressing the collective suffering of the region. Participants in community and health center contexts indicated the need for culture-specific services to address the deep and multilayered grief experiences that exist before, and are exacerbated by, patient illnesses. Funds that are allocated for health workers rotating through communities from Southern institutions may be accompanied with research identifying successful community-based grassroots initiatives and organizing opportunities for knowledge exchange that incorporate these practices.
Knowledge exchange
“Indigenous” or “traditional” knowledge is not a static entity; knowledge is constantly modified by internal changes in the community and influences from without. 44 These modifications are evidenced in EOL care in Nunavik where both medicine and religion have shaped modern EOL care practices. Nevertheless, existing healthcare structures have a responsibility to preserve capacities for Indigenous to valorize their knowledge and resources.44,45 In the context of Nunavik, we found that both elders and younger members of the community continue to draw on land-based food sources and embodied practices in EOL care and several were happy to describe these to us. Traditional family values related to the grief process had also been maintained. These practices are at risk of disappearing when undervalued by healthcare structures. Inviting this knowledge and these practices into collaborative care would permit better EOL care provision. In turn, translating “medical knowledge” into audiovisual materials translated in Inuktitut concerning disease progression, palliative care interventions, and options to patients and families will serve to reduce some of the confusion concerning advanced care planning decisions.
Conclusion
Nunavik Inuit have cared for the dying in family dwellings, applying caregiving practices passed down for generations. Over the past 70 years, sociocultural, geographical, and structural factors have given rise to a tenuous partnership between the Nunavik communities and healthcare institutions seeking to meet the needs of Inuit requiring medical intervention at the EOL. Establishing a sustainable approach to EOL care requires transparency concerning the sociohistorical environments in which institutional care was developed, as well as a deeper understanding of successful EOL care practices offered by communities. Rather than viewing the above-mentioned challenges as indicative of failure, they may be considered inherent to a process of change. An Inuit participant in her late 30s contextualized the current struggles faced by her community in stating, “We are the in-between generation,” straddling the consequences of historical events and the future of a thriving community. Perhaps those of us who come from outside these communities may see ourselves the same way—an “in between-generation” cognizant of the history in which institutional care was developed in Nunavik and now finding our way forward.
Footnotes
Acknowledgments
We would like to acknowledge the continuous support of the Nunavik Regional Board of Health and Social Services, our participants and the community members who supported our study. Thank you also to our reviewers. This study was funded by the Fonds de recherche du Québec–Santé (FRQS).
Author Disclosure Statement
No competing financial interests exist.