
Abstract
Abstract
Background:
Palliative care consultation improves quality of care through symptom management, communication, care coordination, and earlier hospice referral, and it may decrease burdensome hospital readmissions at the end of life.
Objectives:
To compare 30-day readmission rates for patients admitted with exacerbation of congestive heart failure (CHF) receiving palliative care consultation services compared with controls.
Design:
Retrospective cohort study using propensity score matching. A secondary, subgroup analysis compared patients with palliative care consults and patients with an incomplete consult order.
Settings/Subjects:
Single-center study in an academic acute inpatient setting. Of a pool of 8215 admissions from January 1, 2011 to April 6, 2014, 356 included a palliative care consultation, and 356 matched controls were found.
Results:
The 30-day readmission rate was 50.8% for admissions including a palliative care consult and 36.0% for controls (OR 1.8, 95% CI 1.4–2.5). Those with a completed consult had fewer readmissions compared with those with an incomplete order, but this difference was not statistically significant (43% vs. 53%, χ2 = 1.9, p = 0.171).
Conclusion:
No reduction in the risk of 30-day readmission was observed in the palliative care group, suggesting that palliative care services may not have the same effect on readmission rates in CHF patients compared with others. The subgroup analysis suggests that the difference between palliative care and control groups may reflect residual confounding, possibly due to critical social variables that are not captured in the electronic medical record, highlighting the difficulty in studying this population.
Introduction
M
An estimated 20% of Medicare beneficiaries discharged from a hospital are re-hospitalized within 30 days, and unplanned re-admissions cost Medicare about $17.4 billion of the program's $102.6 billion total costs in 2004. 7 In addition, medical care near end of life accounts for almost 1/3 of annual Medicare expenditures. 8 Thus, as part of the ongoing efforts to improve quality and to slow the growth of healthcare costs, the Centers for Medicare and Medicaid Services (CMS) and other healthcare stakeholders are increasingly examining new strategies to decrease unplanned readmission, including financial penalties of up to 3% of total Medicare revenue for hospitals with higher than average readmission rates. 9 State Medicaid programs, for example, the New York State Delivery System Reform Incentive Payment Program (DSRIP), are also aiming at reducing readmissions. 10 CMS began by focusing these efforts on three admitting diagnoses: congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia (PNA).
Studies report that cohorts of patients who receive palliative care services during the index admission have lower rates of readmission and improved quality of life for both patients and families.2,5,11–13 However, previous studies have focused mainly on cancer patients receiving palliative care.2,11,12 CHF patients, who are likely to be represented in the CMS Hospital Readmission Reduction Program, have benefited from inpatient palliative care services, showing improved symptom burden, quality of life, and depressive symptoms. 14 Preliminary data suggested that palliative care services may also reduce readmissions for patients admitted with AMI, CHF, and PNA. 15 However, there has been a recent shift in the field of palliative care toward a broader scope of practice serving high-risk patients earlier in the course of their terminal illness, and the effect of palliative care on readmission rates may be different in this population.
Recently, methods using propensity scores have become more frequently used in the palliative care literature given the high risk of bias by indication in observational studies of palliative care interventions.13,16,17 This study aims at examining readmission rates between patients admitted with CHF receiving palliative care consultation compared with usual care patients using propensity score matching.
Materials and Methods
This study was conducted within Montefiore Medical Center, an academic medical center in the Bronx, NY, consisting of three general hospitals with 1491 beds. The medical center provides care to many underserved and minority patients and serves as the University Hospital of the Albert Einstein College of Medicine.
Data were extracted from a replicate of Montefiore's Clinical Information System using healthcare surveillance software (Clinical Looking Glass™; Emerging Health Information Technology; Yonkers, NY). Clinical Looking Glass was queried to identify adult admissions for AMI,* CHF,† or PNA,‡ at all three of Montefiore Medical Center's main campuses from January 1, 2011 to April 6, 2014. 18 This study was approved by the Montefiore/Einstein Institutional Review Board.
Inclusion and exclusion criteria
Cases
Patients were included if they were ≥18 years of age, nonpregnant, admitted to the medical intensive care unit (MICU), any surgical ICU, the cardiac care unit (CCU), general medicine, surgery or surgical subspecialty service, family medicine, cardiology, or oncology service between January 1, 2011 and April 6, 2014 with the primary diagnosis of CHF and were seen by the palliative care consultation service during the index admission. Admissions to pediatrics, obstetrics, and psychology services were excluded. Patients who died during the index admission or who were discharged against medical advice were excluded. 19 During the study period, a program to provide a palliative care consultation to all patients evaluated for left-ventricular assist devices (LVADs) was initiated at our institution. Given that these patients may be at high risk for readmission, LVAD patients were also excluded. Because PNA and AMI are acute events with clear curative therapies, admissions for PNA and AMI were excluded and this study focused on CHF admissions only. A sensitivity analysis was conducted, excluding patients with a hospital length of stay of three days or less or palliative care consultation two days or less before discharge as in previous studies,20,21 because brief palliative care involvement is less likely to impact utilization outcomes.
Controls
Propensity-matched controls were drawn from a large pool of inpatients using the same inclusion and exclusion criteria as cases with the exception of palliative care consultation.
Development of propensity score
A number of covariates that have been linked to risk of readmission were examined and considered as candidates for inclusion in the propensity score model including age,7,22 race,7,22–25 gender,7,22,26 Charleson Comorbidity Index,27,28 comorbid cancer,23,26,28 comorbid renal failure,7,23,26 comorbid mental illness,23,29 comorbid anemia, 23,28,30 comorbid chronic obstructive pulmonary disease,26,30 comorbid diabetes, 30 comorbid substance abuse, 29 comorbid CHF,23,26 comorbid dementia, comorbid HIV infection, documentation of weight loss, 23 insurance status at time of index admission,22,26,31 length of stay for index admission,7,23,26,28,30,31 admission source on index admission (e.g., from home, nursing home, other), 23 primary language, 23 primary care physician listed in chart (yes or no), 31 lowest albumin level during admission, lab-based acute physiology score, systolic blood pressure <90, number of prior all-cause admissions in the past year, and socioeconomic status.
A propensity model predicting palliative care consultation was built. Variables considered if they were potential covariates related to both treatment group and outcome, as well as those previously shown to be strongly related to outcome.17,32 Balance of propensity score across treatment and comparison groups was achieved with nine blocks. Approximately 50 iterations of the model were run to obtain adequate balance of the variables across blocks. The final model remained unbalanced for the variables quartile of hospital length of stay in block 1 and comorbid cancer and comorbid psychiatric disorder in block 3. This was considered adequate balance. 17 The final model included 34 variables representing socio-demographic variables, co-morbid conditions, and clinical measurements.
Outcome
All-cause 30-day readmission was the primary outcome due to the difficulty in distinguishing between planned and unplanned readmissions for the entire cohort. Reason for readmission was examined in more depth after propensity matching was completed.
Mediation
Discharge with hospice services was examined as a potential mediator. 22
Statistical analysis
Admissions that were not within the area of common support were excluded. Matched controls were found by using nearest-neighbor 1:1 matching by propensity score of patients with palliative care consultation with controls. Proportion of palliative care patients readmitted within 30 days was compared with proportion of propensity-matched control patients readmitted within 30 days. Mantel-Haenszel bounds were computed to explore the sensitivity of the estimated effects. A secondary analysis was conducted to evaluate discharge as a potential mediator, using the Sobel-Goodman test for mediation. Date of death was obtained from Clinical Looking Glass, but we were unable to include deaths not recorded within the Montefiore system. A Kaplan-Meier survival curve was constructed by censoring at date of death when available. At least 270 patients were needed to have a power of 0.80 to detect a reduction in rate of 30-day readmissions from 25% to 15% between groups at a significance level of α = 0.05. Statistical analysis was conducted by using statistical software (STATA) STATA/IC software, version 12.1 (StataCorp, CollegeStation, TX).
Results
Eight thousand two hundred fifteen acute care admissions for CHF were included in propensity score development (Fig. 1). Of those, 356 included a palliative care consultation, and 356 propensity matched controls were found, resulting in a total sample size of 712 admissions of 583 unique patients. Most clinicians ordering a palliative care consult listed multiple reasons for consult (mean and median = 2 reasons). Common reasons included goals of care discussion (72%), symptom management (41%), patient or family psychosocial support (32%), hospice eligibility or transfer to the palliative care/hospice inpatient unit (31%), pain management (14%), and withdrawal of life-sustaining treatments (4%). Table 1 shows the baseline characteristics of palliative care patients and propensity-matched controls along with summary data of the pool of unmatched controls.
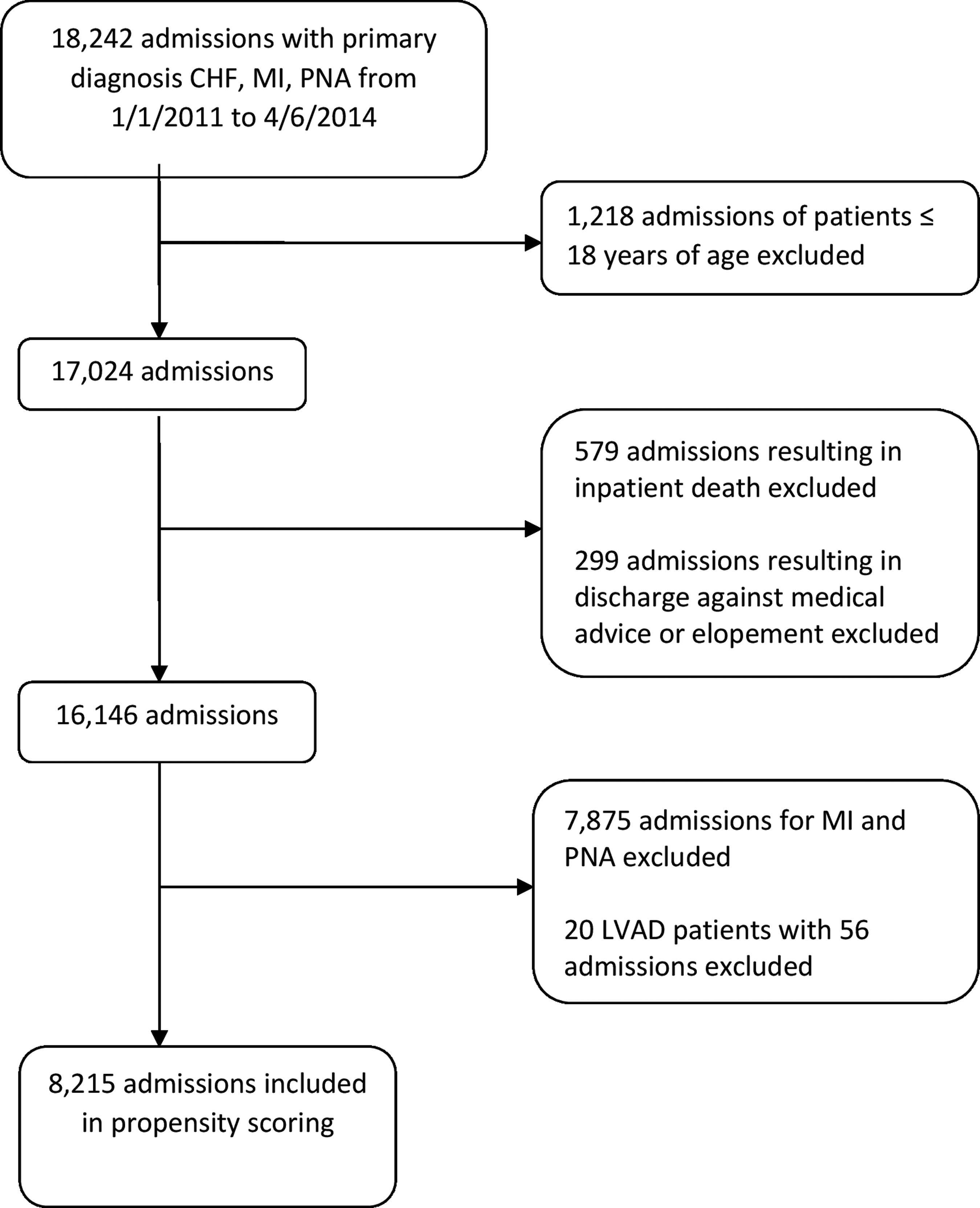
CONSORT flow diagram.
Of the admissions including a palliative care consultation, 50.8% resulted in readmission within 30 days compared with 36.0% of propensity-matched controls (OR 1.8, 95% CI 1.4–2.5) (Fig. 2). Sensitivity analysis showed that these results are insensitive to bias that would increase the odds of palliative care consultation by 40% or less. Excluding patients with a hospital length of stay three days or less or palliative care consult two days or less before discharge did not substantially change the results. Most of the patients (497, 85%) had at least one readmission during the study period (observed for at least six months after last index admission). Of these readmissions, 56% were related to the index admitting diagnosis, 11% were due to exacerbations of another comorbid condition, 18% were due to a new problem other than sepsis, and 14% were due to sepsis. These proportions remained similar when restricting to readmissions within 30 days and between patients seen by palliative care and controls (Table 2). There were no planned readmissions (e.g., for staged procedures, chemotherapy, etc.) within 30 days in this sample.
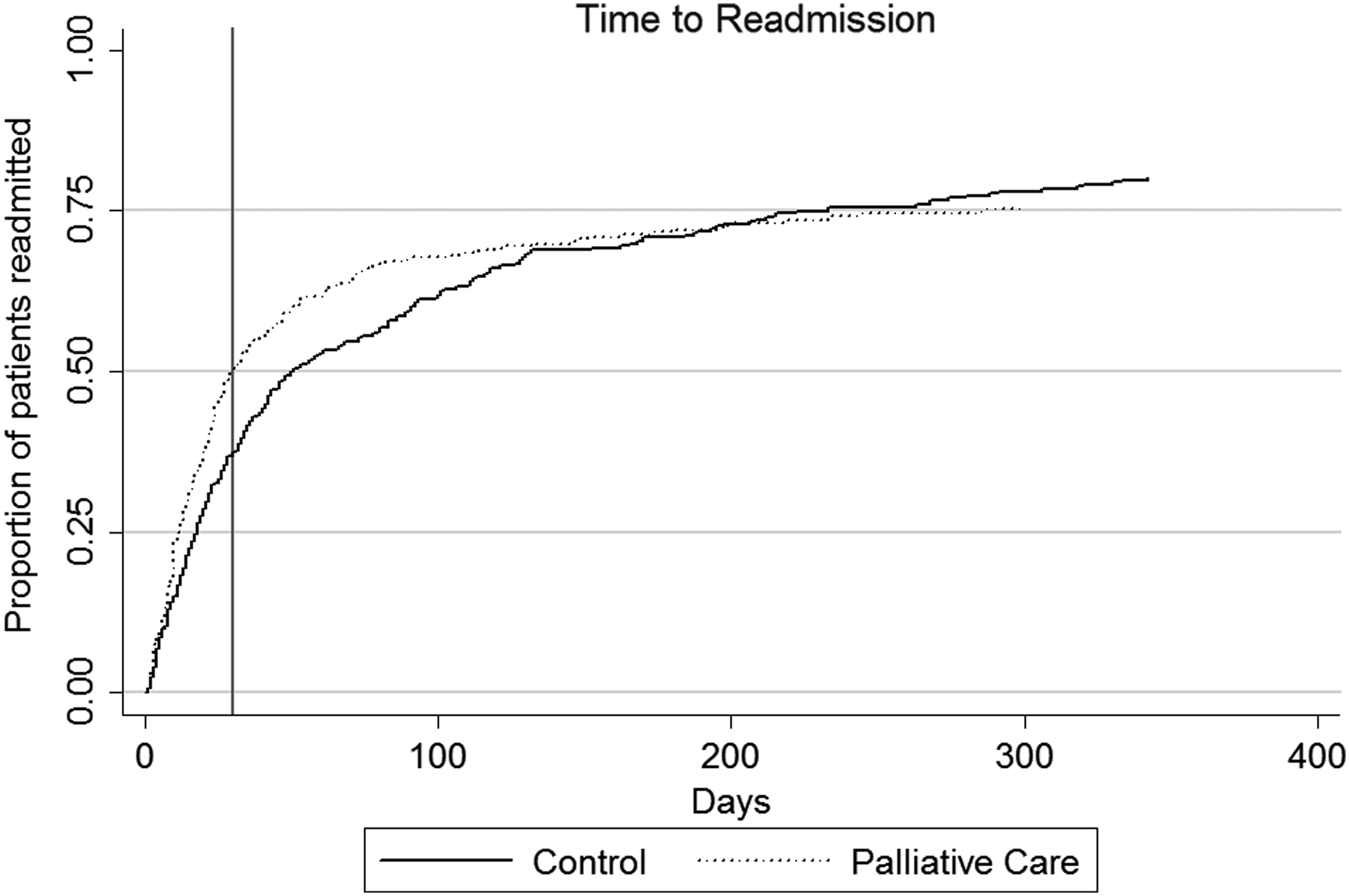
Kaplan-Meier curve showing time to readmission for palliative and usual care patients.
During the study period, 138 (39%) of the patients who received a palliative care consult had a death recorded in Montefiore's electronic medical record, compared with 132 (37%) who did not receive a consult (χ2 = 3.6, p = 0.057). Average time to death was 136 days (median 50 days, SD 194 days) in the palliative care group compared with 262 days (median 156 days, SD 269 days) for patients not receiving palliative care consultation (K-S = 0.33, p < 0.001).
A total of 46 patients (13%) in the palliative care group and 10 patients (3%) in the control group were discharged home with hospice services. Hospice discharge was not a significant mediator of the relationship between palliative care consultation and readmission (Z = −0.28, p = 0.777).
A subgroup analysis was performed by using the 285 patients with palliative care consultation orders for whom data on completeness of the order were available. Of these patients, 57 (20%) had orders placed in our electronic ordering system for palliative care consultation, but the order was not completed, typically due to retraction of the order by the primary team, and occasionally due to the patient being discharged before being evaluated by the palliative care consultation service. Fewer patients with a completed palliative care consult were readmitted compared with those with a consult ordered, but not completed, but this difference was not statistically significant (43% and 53%, respectively, χ2 = 1.9, p = 0.171).
Discussion
These findings do not support the hypothesis that palliative care consultation is associated with reduced 30-day readmissions in patients admitted to the hospital for CHF. Most health service outcome studies in palliative care have focused on patients with cancer,11–13 and little is known about palliative care outcomes in heart failure. 2 However, patients with cancer represent only a portion of all patients dying in the United States. In fact, cardiovascular disease is the leading cause of death. Although both hospice and palliative care services have been available to patients with non-cancer terminal illness, the integration of this care with traditional disease-directed therapy and the evidence base for palliative care best practices for non-cancer terminal illness are still in their infancies. 33 Patients with non-cancer terminal illness face different functional trajectories, different symptom management issues, different prognostic dilemmas, and different interactions with the healthcare system in their decline toward death.34,35 Strategies that work well for terminally ill cancer patients may not translate well to patients with other disease states. In fact, analysis of secondary endpoints in a previous study of inpatient palliative care for patients with CHF also failed to show an association between palliative care consultation and reduction in readmissions. 14
Cancer patients typically have a period of relative clinical stability followed by a shift toward rapid decline ending in death. This creates a natural inflection point that helps clinicians identify when hospice referral is appropriate. In contrast, patients with terminal illness due to end-organ failure typically have a waxing and waning clinical course with slow steady decline interrupted by periods of clinical crisis followed by a return to function that is often only slightly lower than baseline. 35 It is difficult for clinicians to determine at what point the patient is less likely to benefit from disease-directed therapy. In addition, prognostic prediction models have had disappointing reproducibility.36,37
Best practices of subspecialist physicians treating end organ disease are often palliative in nature. For example, inotropes used for treatment of advanced heart failure increase risk of death but are often used for successful palliation of symptoms. 38 Financial constraints make it difficult for most hospice agencies to provide inotropes. 36 Patients may also feel more comfortable in the hospital environment where they can undergo aggressive diuresis with addition of inotropes, making hospitalization an acceptable outcome. In fact, even hospice referral did not significantly mediate readmission in this cohort.
These findings differ from earlier data from our institution. 15 We previously analyzed 30-day readmissions in a smaller group of patients admitted for CHF, PNA, and AMI from 2011 to 2013 and found that palliative care consultation was associated with a lower 30-day readmission rate (22.7% vs. 27.3% in controls matched on comorbidity, gender, and age only). The comparatively very low rate of readmissions in the palliative care group in our previous study is likely accounted for by the inability to control for death within 30 days of readmission. Before 2012, palliative care was often consulted very late in the course of illness for CHF patients, mostly in the last days to weeks of life. Subsequent quality improvement efforts at our institution led to earlier palliative care involvement with patients who may be more likely to survive to readmission within 30 days.
The average 30-day readmission rate for CHF admissions at our hospital during the study period was 25.6%, which is lower than the control group in this study due to propensity matching, which selected for the most frail and vulnerable among the CHF patients. Given the pressures to reduce readmissions, palliative care may have been called on to assist with our institution's “superutilizers,” 39 thus selecting for the population most likely to be readmitted.
The main limitation of this study is that it is a retrospective observational study. Indication bias is a particular concern for this study, because patients with poorer prognosis and increased risk for adverse events, including readmission, are more likely to be referred to palliative care services. It is likely that the propensity matching process failed to completely control for confounding by indication. In fact, the patients seen by palliative care had a higher mortality and shorter average time to death compared with controls. In addition, we were unable to adequately control for social support; only proxy variables such as socioeconomic status and race/ethnicity were available in our EMR data that do not reveal important factors such as availability of an informal caregiver. Physicians may consult palliative care more often in patients with poor social support, who may also be more likely to be readmitted. In addition, palliative care consultation teams may provide psychosocial support in the hospital that is unavailable to patients in the community.
Sensitivity analysis indicated that a bias that would increase the odds of palliative care consult by 45% could change the results. If variables such as poor health literacy or lack of availability of an informal caregiver increase the odds of palliative care consult by at least 45%, the absence of these variables in the analysis could explain our findings. In fact, in the secondary analysis, patients with a completed consult had a slightly lower frequency of readmission compared with those with a cancelled or retracted order. This has important implications for research in palliative care and should be further investigated. However, this limitation applies to previous studies that explored 30-day readmissions and does not explain the difference between our findings and those of other palliative care cohorts, making it likely that there is an important difference in patterns of readmission between palliative care patients with CHF and other terminal illnesses.
Finally, we did not have data on the number of palliative care follow-up consultations during admission in this dataset. It is unknown whether there was sufficient contact with the palliative care team to develop rapport and establish goals; however, excluding short admissions (three days or less) and consults two days or less before discharge did not change the results.
One conclusion that could be drawn from these results is that patients with heart failure have an unacceptably high rate of readmission near the end of life and quality improvement efforts should be focused on improving outpatient palliative and hospice care for these patients. For example, some of the local hospice agencies in our area are now providing continuous infusions of inotropes at home for palliation of symptoms. Another view, however, is that hospitalization may serve an important palliative goal of aggressive symptom management in patients with advanced cardiac disease, a topic that should be investigated further by using qualitative methods, such as in-depth interviews of patients and caregivers, to clarify the meaning of hospitalization for them. It is likely that palliative care consultation improves symptom management and provides valuable psychosocial support for patients hospitalized with exacerbation of advanced heart failure. These services should be augmented by improved community-based palliative care. The use of 30-day readmission rates as a quality indicator for these patients may need to be examined more carefully, and continued exclusion of terminally ill patients from CMS readmission reduction incentive programs is appropriate.
Footnotes
Acknowledgments
The authors would like to thank the Centers to Advance Palliative Care (CAPC) for guidance in conceptualizing the propensity score matching for this study. They are especially grateful for the input of Melissa Aldridge, PhD, MPH, MBA and Helene Starks, PhD, MPH. They would also like to thank Dr. Andrea Lyman, MD, MSc, MS, Director of the Public Health/Preventive Medicine Residency Program at the New York City Department of Health and Mental Hygiene, for her insights on an earlier draft of this article.
Author Disclosure Statement
No competing financial interests exist.