
Abstract
Abstract
Background:
The Latin American Association for Palliative Care (ALCP) developed 10 indicators to monitor the development of palliative care. The indicators have been applied across Latin American countries but have not been used internally.
Objective:
The aims of this study were to document the development of palliative care in Argentina at the national and provincial levels by using a selection of the indicators developed by the ALCP and identify the difficulties and needs of healthcare professionals working in palliative care. This is the first study to apply the indicators intranationally.
Methods:
This was a cross-sectional pilot study based on two questionnaires with representatives from each province, one workshop, and telephone conversations to corroborate the collected data. These data were used to calculate a preselection of eight ALCP indicators covering four main areas of development: education, policy, service delivery, and medication. A total of 30 participants took part in the study.
Results:
The application of the ALCP indicators at the province level led to the identification of inequalities in the development and distribution of services across the country. The provinces in the north-west were identified as the region with the greatest need for development. The main difficulties for healthcare professionals were lack of national service registries, certified palliative care specialties, and opportunities for continuous training.
Discussion:
The ALCP indicators are useful tools for mapping palliative care development within countries. Further work needs to be carried out to increase their specificity and integrate them in policy design and service delivery.
Background
P
The Latin American Association for Palliative Care (ALCP) developed 10 indicators to monitor the development of PC and promote the establishment of regional and national strategies.7,11 These indicators were organized in four categories: policy, education, service provision, and opioids.
The aims of the ALCP were to compare the status of PC development across Latin American countries using these indicators and provide national governments with a tool for monitoring PC development in their countries. Previous studies have already used the indicators to compare the delivery of PC across Latin American countries. 7 The indicators have not been used to look at the development of PC within countries. In this article, we present the findings of a study that focused on mapping the development of PC in Argentina at the national and provincial levels, using a preselection of eight indicators of PC development established by the ALCP. This is the first study to apply the indicators intranationally.
Palliative Care in Argentina
Argentina is the second largest Latin American country with regard to territorial extension, after Brazil. Argentina is divided into 23 provinces and the autonomous city of Buenos Aires. Sixty percent of its population lives in the provinces of Buenos Aires, Córdoba, and Santa Fé. With 40 million inhabitants, 10.2% of the population with 65 or more years of age and 14.3%, with 60 years or more, 12 Argentina ranks third in Latin America with regard to the size of its aging population, after Uruguay and Cuba. 13 The health system is divided into three main types of providers: public services (covering approximately 50% of the population), mutuals or social plans (45%), and the private sector (5%).14,15 Each province has its own provincial health program and autonomous Health Ministry, reporting to the National Health Ministry. Healthcare delivery varies considerably across and within provinces. 16
Palliative care in Argentina has a history of 30 years.17–20 The Argentine Association of Medicine and Palliative Care (AAMYCP) was established in 1994. In 2015, the National Health Ministry promulgated the medical specialty in PC (Resolution 1814/2015), yet it is still not regulated equally across the country. There are only two provinces with an accredited PC specialty: Santa Fé and Neuquén. The variability in PC delivery and training opportunities for professionals across provinces is evident, but has not been fully documented (for the mapping of pediatric PC services, see Ref. 21 ). Previous studies have ranked Argentina fourth in Latin America with regard to PC development, but these rankings do not take into account the uneven internal development and distributions of services.5,7
Aims
The aims of this study were as follows: (1) document the development of PC in Argentina at the national and provincial levels by using a selected number of the indicators developed by the ALCP and local experiences of service delivery, (2) identify the difficulties and more frequent needs of healthcare professionals working in PC, and (3) identify the areas that require development at a national level taking into consideration differences among provinces.
The indicators we used are presented in Table 1. This selection of indicators was informed by our knowledge of the available data on PC as well as previous published studies that used ALCP indicators.6,7
Design
This is a cross-sectional pilot study. 22
Data collection
Data were collected through two questionnaires and one workshop with study participants.
First questionnaire
We distributed the first questionnaire via e-mail to all participants. This questionnaire was designed in collaboration with [Prof. Gomez-Batiste], adapting the methodology (quantitative and qualitative) used to map and evaluate the Catalonia WHO Demonstration Project.23,24 This questionnaire requested general information on the province (population, disease incidence, etc.), general information on PC service delivery, the main difficulties encountered by PC staff, and the resources they need to further develop PC services in their regions. A description of the items included in the questionnaire can be found in Appendix A1.
Second questionnaire
After carrying out preliminary analysis of the first questionnaire, a second questionnaire was developed to collect targeted information aimed at calculating the ALCP indicators. The participants were asked about the existence of PC plans or programs, educational programs on PC for doctors and nurses, the availability of medical teams and specialized physicians, and the availability of opioids in pharmaceutical establishments. Detailed definitions of the indicators were provided to ensure the standardized collection of information and participants were provided with instructions on how the numerators and denominators needed to be built. A description of the questionnaire can be found in Appendix A1. The participants were contacted via telephone to corroborate our interpretation of the data, identify the data sources that were used, and address issues of missing data.
Workshop
All participants were invited to a workshop with the aim of discussing preliminary findings in greater detail. The participants were asked to share their experiences of the development of PC services in their provinces. The discussion was facilitated through the use of participatory methods such as graffiti wall and problem trees. 25 The discussions that took place during the workshop were recorded in the form of field notes.
Recruitment and sample
Participants were recruited from February 2015 to March 2016. The identification of potential participants was based on the screening of institutional lists (hospitals and hospices) for renowned professionals in the field and referrals from other professionals (snowball sampling). We sought to recruit at least one participant from each province and asked them to act as a representative for their province. This recruitment method has been used in previous PC mapping studies.26,27 The inclusion criteria were healthcare professionals who played a key role in the delivery of PC and acted as directors or coordinators of PC teams in public or private hospitals or hospices. The participants also needed to have access to relevant data sources in their provinces. Potential participants were identified using institutional records such as hospital directories. The potential participants were contacted via e-mail and provided information about the study and what their participation would entail. They were then asked if they would like to take part.
Data analysis
Data from the first questionnaire were used to create a profile for each province and identify the most frequent difficulties and needs reported by the province representatives. Data from the second questionnaire were used to calculate the indicators at the national level and at the level of each province. The process for calculating each indicator is outlined in Table 2. Additional data sources were consulted for some of the provinces. The full list can be found in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/jpm).
Atlas Federal de Legislación Sanitaria de la República Argentina (Federal Atlas of Health Legislation of the Argentine Republic), Ministry of Health. 28
University Career Guide, Sistema de Información Universitaria (System of University Information). 29
Accreditation of Graduate and Postgraduate Courses, Comisión Nacional de Evaluación y Acreditación Universitaria (National Commission of University Evaluation and Accreditation). 30
2010 National Census carried out by the Instituto Nacional de Estadística y Censos (National Institute of Census and Statistics of Argentina). 12
The field notes from the workshop were analyzed using content analysis and were mainly used to expand our understanding of the difficulties faced by staff delivering PC services. The workshop and telephone conversations with the participants were fundamental components of the study and ensured our accurate interpretation of the data.
Ethical approval
The study protocol was reviewed and approved by the Independent Ethics Committee of the Foundation Huesped. An informed consent process was followed with the research participants where they were informed that their participation in the study was voluntary; they could withdraw at any time; and the information they provided would remain confidential.
Results
A total of 30 participants took part in the study. Nobody refused to participate. Participants acted as representatives for their provinces. We were able to recruit representatives for all provinces except for two (Salta and Jujuy). Data for the missing provinces were obtained through other data sources (Table 2) and representatives from other provinces. We were able to collect data on the rest of the provinces, with the exception of some missing data for Buenos Aires province, the city of Buenos Aires, and Tierra del Fuego (Table 4).
Eighteen of the participants were women and 12 were men. Almost all of the participants were doctors, 28 with the exception of two psychologists. All of the participants worked full-time in the delivery of PC services. Their experiences in this field ranged from 1 to 10 years. Most participants 21 worked in the public sector, eight worked in the private sector, and one participant worked in both the public and private sectors. The details of the data sources each participant was able to access can be found in Supplementary Table S1.
Indicators at the national level
The indicators at the national level are summarized in Table 3. Argentina does not have a national PC plan or program. There are guidelines for specific diseases (i.e., the Programa Nacional de Cuidados Paliativos developed by the National Cancer Institute for cancer patients) and populations (i.e., pediatric patients), but there are no plans with clear policies and budget aimed at the delivery of PC for all patients at the national level. In terms of the training of medical professionals, 19% of the medical schools and 8% of the nursing schools include PC in their curricula, and there are nine PC educational programs for doctors accredited by a wide range of universities.
Not at the national level, but two provinces have palliative care programs (Table 4).
Based on census data from Instituto Nacional de Estadistica y Censos. 12
Based on census data from INDEC. 12
The program only exists in Rosario, the capital of the province.
In the private healthcare system.
—, Missing data.
PC is included in the primary care list of services in 12 provinces. There are ∼73 PC services in the country and 166 accredited doctors. Approximately 316 pharmaceutical establishments dispense opioids, including public and private facilities.
Indicators at the province level
Table 4 presents a breakdown of the data by province. There is great variability in the development of PC across the country. The province with the highest level of development is Neuquén. This province has a PC program, it provides undergraduate training for doctors and nurses in all schools, and has one accredited specialty in palliative medicine. As we were finishing this article, the first PC doctor gained accreditation. It includes PC in the delivery of services at the primary care level and has an adequate distribution of services, specialized doctors, and opioids in relation to its population size. In contrast, other provinces such as Salta and Jujuy do not have any development of PC services.
Only two provinces (Neuquén and Santa Fé) have an established PC plan, but more than half include PC in the delivery of services at the primary care level. Neuquén distributes services homogeneously across the province, while in Santa Fé, these services can only be found in the capital of the province (Rosario). Other provinces do not have established programs, but have created networks of providers to deliver community-based care. This is the case of Rio Negro, where a network of multidisciplinary teams has been developed to provide hospital-based and home-based care across five regions (Viedma, Cipolletti, Villa Regina, General Roca, and San Carlos de Bariloche). At the national level, there is an unequal distribution of PC services (including specialized doctors) and pharmaceutical establishments that dispense opioids. As seen in Figure 1, there are still evident gaps in services in the northern provinces and those located in the west.
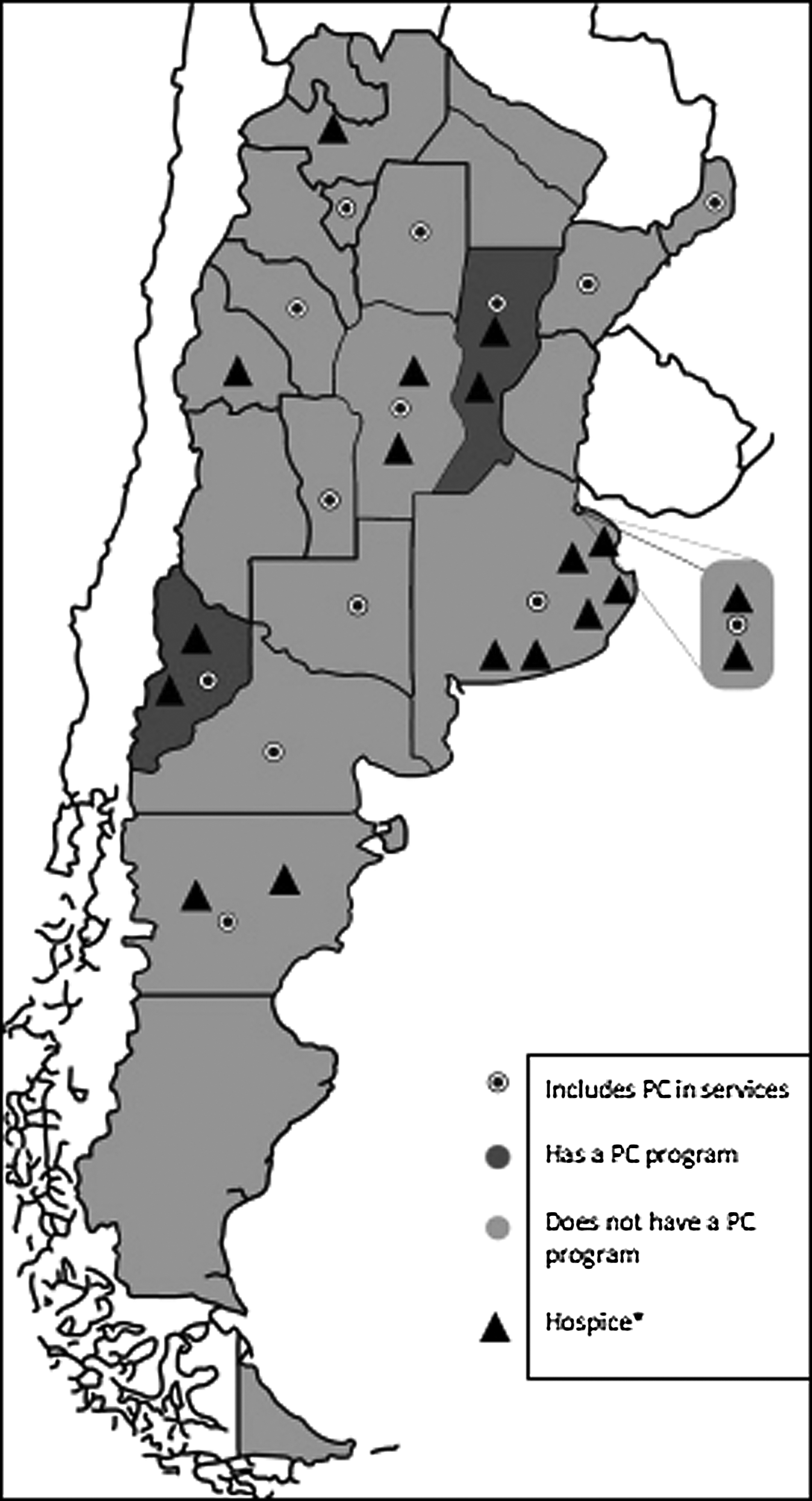
Mapping of inclusion of palliative care services (PS.1), existence of palliative care programs (PO.1), and distribution of hospices. *Hospices are defined as institutions caring for patients until death, and in some cases, bereavement. The concept of hospice used here does not include care in the patient's home.
Difficulties and challenges in the development of PC
The first questionnaire asked the representatives to identify their main difficulties and challenges as well as their needs. Their responses are summarized in Table 5. It is evident that there are barriers operating in the development of PC services at the province level. These barriers mainly concern issues related to the design and implementation of PC policies, the training of healthcare professionals, the funding of PC development and delivery, the creation of national registries, and the equal distribution of opioids. The representatives requested assistance with all of these issues and proposed strategies to work collaboratively with other provinces, sharing experiences and establishing bilateral training opportunities.
Discussion
Our calculation of the ALCP PC indicators highlighted important trends in the development of PC in Argentina at the national and provincial levels. At the national level, the results of our indicators differ from those reported in prior studies. For instance, we found a smaller quantity of services per million inhabitants (1.82) compared to the indicators published by Pastrana et al. (3.76). 7 This could be due to differences in reporting, or it could potentially be linked to the dissolution of services in some areas of the country. We are aware of two services that closed recently, one in Buenos Aires and the other one in Tierra del Fuego.
Our calculation of the number of doctors working in PC per million inhabitants was 4.13, compared to 2.50 reported by Pastrana et al., 7 which could suggest an increase in professional training opportunities in the PC field. We found that the number of specialized PC educational programs for doctors was twice the number found in previous studies (eight in our study vs. four in Pastrana et al. 7 ), but the proportion of medical schools that include PC education in undergraduate curricula was 19% while Pastrana et al. 7 documented 22%.
During our study, we were able to collect data to calculate indicators that had not been calculated before for Argentina. This is the case of ED.2, the proportion of nursing schools with PC at undergraduate level (8%), and ME.3, the number of pharmaceutical establishments that dispense strong opioids per 1 million inhabitants (7.88).
Argentina is classified by the Worldwide Palliative Care Alliance (WPCA) as a level 3b 5 and has an ALCP index of 4.39, 7 appearing to be one of the Latin American countries with the highest development of PC (ranked fourth in Latin America according to the ALCP index). However, when the ALCP indicators are used at the province level, we are able to see that the development and distribution of services are unequal across the country. Services are concentrated in Neuquén, and Rio Negro, with a homogeneous distribution of services, and Buenos Aires, and Santa Fé, with a heterogeneous distribution and some areas where PC is not available. The northwest region has severe deficiencies in care delivery, training opportunities for healthcare professionals, and the availability of opioids in pharmaceutical establishments. This situation poses pressing questions regarding the type of PC patients are receiving (or not receiving) in these areas of the country.
The analysis of the indicators as well as the difficulties and needs reported by the province representatives pointed to the lack of standardized registries and training opportunities for healthcare professionals. Future areas of short- and long-term development in Argentina could be the following: (1) the elaboration of a service registry by province, standardized at the national level, (2) the development of opportunities for PC training (basic and continuous training), and (3) the regulation and certification of the palliative medicine and nursing specialties (already promulgated by the Ministry of Health in resolution 1814/2015 for medicine and 199/2011 for nursing).
The findings of this study should be interpreted with their limitations in mind. The indicators measure the presence of services and professionals, but do not allow us to assess the quality of care or the degree to which services are used by the population. Some of the indicators are too general and might not reflect the ways in which services or professional activity are organized. For instance, the number of specialized doctors working in PC per one million inhabitants does not specify if they are full-time or part-time doctors (or both), or acknowledge that these doctors' services might be spread out over the public and private sector. The PS.1 indicator documents the inclusion of PC in primary care, but it does not make a distinction between different components of primary care such as GP or community practices, hospices, or home care.
In addition to the limitations of the indicators, our study is limited in the sense that it relied on data reported by the study participants, potentially leading to skewed or missing data. We were able to cross check some of the provincial data with national databases, but this was not possible for all indicators. The study participants have provided a list of the data sources consulted in each province, but in some cases they could only rely on information obtained by consulting with local providers or pharmaceutical establishments (Supplementary Table S1). Provincial registries and databases are not standardized and the quality of the data is not assessed routinely. This being said, we believe that the participatory approach we used in the study led to the engagement of the study participants during all stages of research, facilitating data collection and analysis. Our sample size is small and future studies should focus on collecting data from larger groups of experts.
Conclusions
The results of this study point to evident inequalities in the development and distribution of PC services in Argentina. The ALCP indicators are not only useful tools for mapping PC development across Latin American countries but can be used to explore service delivery and training opportunities within countries as well. Further work needs to be carried out to increase the specificity of the indicators so they can accurately represent what occurs in practice. In addition, national standards need to be set to identify quality-of-care targets and tailor service delivery accordingly. We are planning further research on national differences in the quality of PC, focusing on patients' and carers' experiences of care and staff members' experiences of care delivery. We hope to identify the factors acting as barriers in the development of PC in Argentina and inform the development of national and regional interventions focused on addressing them.
Footnotes
Acknowledgments
We thank the support provided by members of Red Federal de Atención Paliativa y Cronicidad Avanzada: Mc Garrell Daniela; Carrizo de la Fuente Virginia; Coller Maria; Cattaneo Walter; Simó Mariela; Rey Victoria; Solorzano Fabian Roberto; Pordomingo Virginia; Nespral Alejandro; Gill Mabel; Alassia Alejandro; Nieva Mariela; Barra Luis Pablo; Vargas Mariela; Perez David; Torresi Victoria; Felix Alicia Nora; Pirchi Mariangeles; Marchetti Fernanda; Colautti Norma; Jury Graciela; De Muria Mariano; Del Colle José; Leisa Julián; Besil Belén; Yori Mariana; Jozami Paula; Bunge Sofía and Junín Marta and Najún Matías. We also thank Bruno Vindrola-Padros for his comments on earlier versions of this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.