
Abstract
Abstract
Background:
Methadone has been associated with lower overall survival (OS) in patients with chronic pain. There are no data available on the association of methadone with OS in cancer patients.
Objective:
Our aim was to compare the OS in cancer outpatients undergoing opioid rotation (OR) to methadone and other strong opioids.
Design:
Demographics, symptoms, and morphine equivalent daily dose (MEDD) were collected in patients who underwent OR from strong opioids to either methadone or other strong opioids and returned for a follow-up within six weeks.
Setting/Subjects:
Nine hundred thirty-eight consecutive outpatients to the supportive care center of a tertiary cancer center were reviewed.
Measurements:
Kaplan–Meier curves were used to evaluate survival.
Results:
Of a total of 164 eligible patients, 54/76 patients who underwent OR to methadone and 48/88 patients who underwent OR to other opioids returned for a follow-up visit. The median age was 56 years, 54% were male, and 87% had advanced cancer. There were no significant differences between the two groups in patient characteristics, performance status, MEDD, and pain scores. The Kaplan–Meier curves revealed no significant difference in median OS between all patients undergoing OR to methadone and other opioids [3.75 months (95% confidence interval, CI, 2.30–6.46) vs. 2.62 months (95% CI 1.74–4.33); p = 0.35] and also among those who returned for a follow-up following an OR to methadone and other opioids [5.15 months (95% CI 3.64–7.41) vs. 5.90 months (95% CI 2.62–9.28); p = 0.89].
Conclusions:
We observed no significant difference in OS in cancer patients in methadone group compared to other opioids.
Introduction
M
Methods
This study represents an ad hoc analysis of a study previously reported by our group and was approved by the institutional review board at The University of Texas MD Anderson Cancer Center. 12
The supportive care center (SCC) in our institute includes an interdisciplinary palliative care team that practices a standardized model of care using several validated tools.25,26 We retrospectively reviewed the charts of consecutive patients seen in our outpatient supportive care center in 2008 to identify patients undergoing OR from other strong opioids to methadone and from other strong opioids to another strong opioid. Data regarding demographics, patient characteristics, Edmonton Symptom Assessment System (ESAS),27,28 Memorial Delirium Assessment Scale (MDAS), 29 Cut-down, Annoyed, Guilty, Eye-opener (CAGE) questionnaire for screening for alcoholism, 30 pain characteristics, opioid doses, morphine equivalent daily dose (MEDD), 25 and survival (from tumor registry) were collected from the patient's medical record. Successful OR was defined as 2-point or 30% reduction in pain score in patients undergoing OR for uncontrolled pain, resolution of OIN in patients undergoing OR for OIN, and similarly resolution of nausea, constipation, or pruritis in patients undergoing OR for those reasons.12,31,32
Statistical method
Data were summarized using standard descriptive statistics such as mean, standard deviation, and median and range for continuous variables; and frequency and proportion for categorical variables. Difference in categorical variables between two groups was examined by Chi-Squared test or Fisher's exact test when appropriate. A paired t-test was used to examine the change in ESAS from baseline to follow-up. Wilcoxon-Mann-Whitney test was used to compare age, MEDD, and the change of ESAS pain score between two groups. The clinical endpoint was OS time from OR, calculated as time from OR to death (event) or from OR to the last follow-up time (censored), which was estimated using the Kaplan–Meier method and the comparison between patients' characteristics groups was evaluated by log-rank test. All computations were carried out in SAS 9.3 (SAS Institute Inc., Cary, NC) and R 3.1.1.
Results
A total of 938 patients were seen in our SCC in the year 2008 and 190 patients underwent OR. Of those, 26 patients were already receiving methadone and underwent a partial OR of the breakthrough opioid only, and were excluded. Of the remaining 164 patients, 76 underwent OR from a strong opioid to methadone and 54 returned for a follow-up visit. Similarly, 88 underwent OR to another strong opioid and 48 returned for a follow-up visit (Fig. 1). There were no patients who underwent OR from methadone to another opioid. The median mg (range) of methadone used was 15 (5–105).

Flow chart of eligible patients.
Table 1 shows that, of the eligible 164 patients, mean age was 56 years, 54% were male, 73% were white, and 87% had advanced cancer. CAGE score was positive in 12%, 54% had a history of smoking, and 6% had a history of drug abuse. The most common pain type was nociceptive (62%). Uncontrolled pain (79%) was the most common reason for OR followed by OIN (16%) and 69% underwent a successful OR. There were no significant differences between the methadone group and the other opioid group in patient characteristics, cancer type, advanced disease status, performance status, pain description, prerotation MEDD, baseline ESAS scores, and multiple other variables tested. Table 2 shows that there were no significant differences between the two groups in the kinds of antineoplastic treatments received at the time of OR.
CAGE, Cut-down, Annoyed, Guilty, Eye-opener questionnaire to screen for alcoholism; MEDD, morphine equivalent daily dose; OIN, opioid-induced neurotoxicity; OR, opioid rotation; SD, standard deviation.
p-Value comparing among uncontrolled Pain, OIN, and the rest.
There was a significant improvement in the median ESAS pain score in both the methadone group (−2, p < 0.0001) and the other opioid group (−1, p = 0.0034) at the time of follow-up after OR. However, the methadone group had a significantly higher improvement of median pain score compared to the other opioid group (p = 0.045).
The Kaplan–Meier curves (Fig. 2) revealed no significant difference in OS between the methadone group and the other opioid group [median OS: 3.75 months (95% confidence interval [CI] 2.30–6.46) vs. 2.62 months (95% CI 1.74–4.33); p = 0.35]. Among patients who followed up after OR, the Kaplan–Meier curves did not also reveal any significant difference in the OS between the methadone group and the other opioid group [median OS: 5.15 months (95% CI 3.64–7.41) vs. 5.90 months (95% CI 2.62–9.28); p = 0.89].
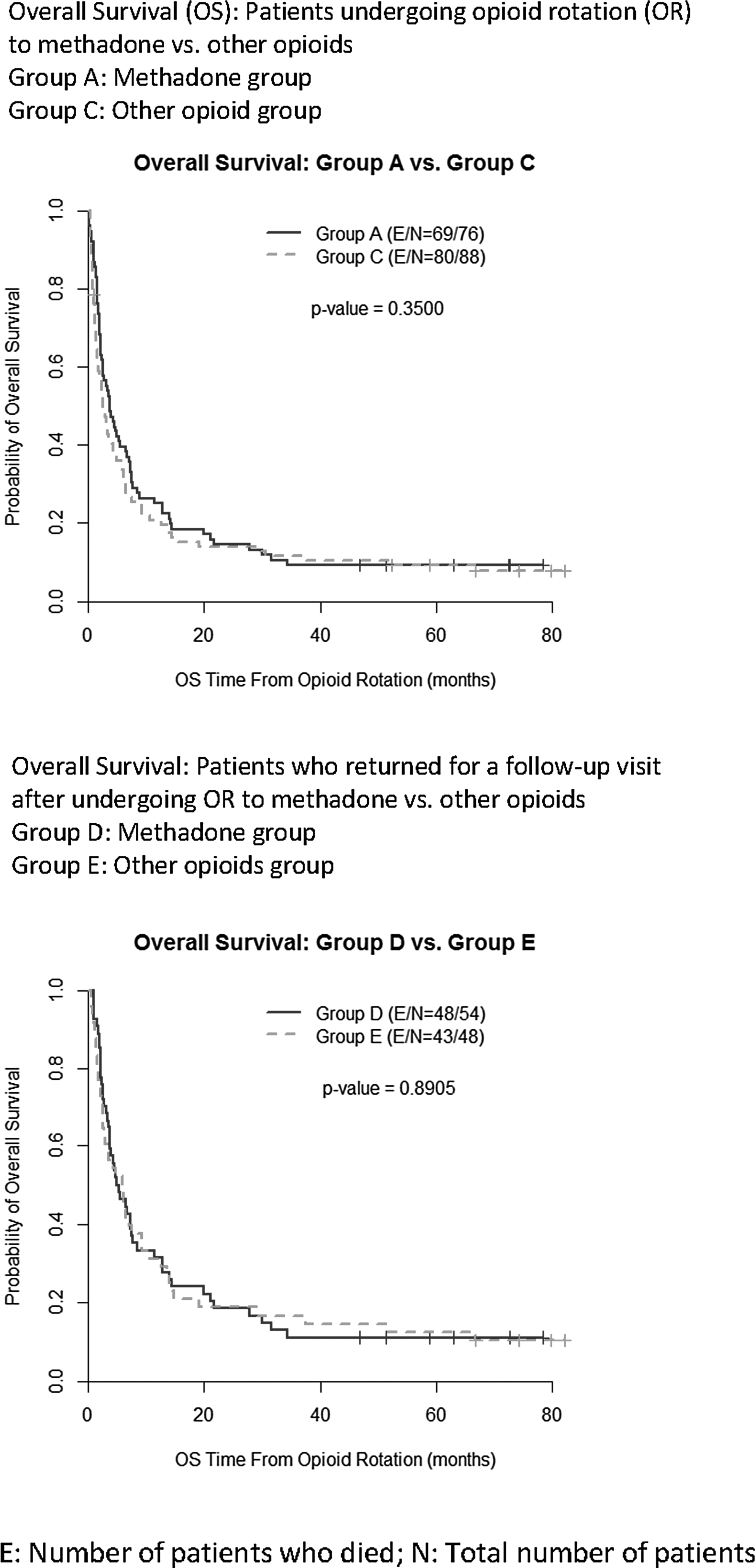
Kaplan–Meier Survival Estimates.
Discussion
Our study did not show any difference in OS in cancer patients receiving methadone compared to other opioids. 33 To our knowledge, this is the first study to evaluate the effect of methadone on OS in patients with cancer. A previous report on cancer outpatients undergoing OR revealed that patients who do not follow up after an OR have a shorter OS. 34 In our study, there was no difference in survival in patients who returned for a follow-up after undergoing OR to methadone or other opioids.
Although not statistically significant, a higher percentage of patients achieved a successful OR to methadone than to other strong opioids. Similarly, the patients rotated to methadone experienced a statistically higher improvement in their pain score when compared to other opioids, underscoring the role of methadone as an important tool in refractory cancer pain and complex pain syndromes. Previous studies demonstrated that rotation to methadone in cancer patients was 84% successful in the outpatient setting and 77% successful in the inpatient setting, and resulted in a long-lasting improvement in pain.3,6,13,35,36
Comorbidities, drug interactions, and concurrent benzodiazepine and other sedating drug use have all been identified as risk factors for increased mortality with methadone.7,8,37,38 An expert panel rightfully recommended extensive counseling for patients and families on methadone safety, routine use of electrocardiography monitoring of the QT interval, assessment of comorbidities and drug interactions, careful initiation and titration, and very close monitoring and follow-up in all patients being prescribed methadone for chronic pain management. 8
Previous studies have shown that very few cancer patients report any deviations from prescribed opioid dose when educated by an interdisciplinary palliative care team, 39 highlighting the importance of patient and family education when prescribing methadone to cancer patients. Our group previously reported that the lower doses of methadone that are typically prescribed to closely monitored cancer patients very rarely result in significant increases in QT intervals, 40 which justifies the frequent use of methadone in cancer pain management. Guidelines for the use of methadone on the lines of those released for chronic pain patients, but stratified based on illness trajectory and prognosis are urgently needed in cancer patients receiving palliative care.
The role of methadone as an adjuvant for treating various malignancies is poorly understood. Our study did not show any therapeutic benefit of methadone on survival in cancer patients15–24 However, a much larger sample size would have allowed us to determine the OS in patients undergoing OR to methadone according to different cancer types, specifically lung and breast cancers along with leukemia. Well-designed and adequately powered studies are clearly required to explore this fascinating association.
This preliminary study shows no impact of methadone use on OS in cancer patients, most of whom had advanced disease. The main limitations of this study are its retrospective design, and the patients had a variety of primary malignancies. However, it is reassuring that cancer types, stage, and performance status were not significantly different between the two groups. Our study did not report the duration of methadone used by the patients. It must be noted, however, that the vast majority of cancer patients stay on methadone and very rarely undergo OR to another opioid. Moreover, there were no patients in this study who underwent an OR from methadone to another opioid. These results must be validated in larger studies. Our team recommends the continued use of methadone as the go-to drug for difficult-to-treat pain syndromes in diligently selected cancer patients, while participating in the usual precautions, careful monitoring, and patient education.
Footnotes
Acknowledgment
This study was supported, in part, by MD Anderson Cancer Center support Grant No. CA016672.
Author Disclosure Statement
No competing financial interests exist.