
Abstract
Abstract
Background:
Few data are available describing the involvement and activities of social workers in advance care planning (ACP).
Objective:
We sought to provide data about (1) social worker involvement and leadership in ACP conversations with patients and families; and (2) the extent of functions and activities when these discussions occur.
Methods:
We conducted a large web-based survey of social workers employed in hospice, palliative care, and related settings to explore their role, participation, and self-rated competency in facilitating ACP discussions. Respondents were recruited through the Social Work Hospice and Palliative Care Network and the National Hospice and Palliative Care Organization. Descriptive analyses were conducted on the full sample of respondents (N = 641) and a subsample of clinical social workers (N = 456). Responses were analyzed to explore differences in ACP involvement by practice setting.
Results:
Most clinical social workers (96%) reported that social workers in their department are conducting ACP discussions with patients/families. Majorities also participate in, and lead, ACP discussions (69% and 60%, respectively). Most respondents report that social workers are responsible for educating patients/families about ACP options (80%) and are the team members responsible for documenting ACP (68%). Compared with other settings, oncology and inpatient palliative care social workers were less likely to be responsible for ensuring that patients/families are informed of ACP options and documenting ACP preferences.
Conclusions:
Social workers are prominently involved in facilitating, leading, and documenting ACP discussions. Policy-makers, administrators, and providers should incorporate the vital contributions of social work professionals in policies and programs supporting ACP.
Background
A
Practice developments in ACP stress the importance of ongoing, in-depth conversations that identify a person's goals, values, and priorities for care rather than primarily focusing on completing advance directives or other legal documents. This process-oriented approach involves an ongoing dialog among the individual, family, and healthcare team about quality of life, personal values, goals of care, and care plans that best effectuate these preferences. 8 Decisions are facilitated regarding preferred medical treatment, approaches to care (e.g., comfort vs. curative care), and places of care (e.g., hospital, institution, or home). 9
Social workers are core members of the interdisciplinary healthcare team and often perform ACP services. They are trained to understand complex family dynamics that are often part of ACP discussions. 10 Many are highly skilled in facilitating difficult conversations among individuals, family members, and the healthcare team on goals of care and treatment options. Furthermore, social workers are skilled at integrating relevant cultural values and norms into patient and family care, as well as addressing cultural barriers to ACP. 11 Finally, the profession's commitment to client self-determination as a core value supports social work advocacy on behalf of patients' preferences. 12
Despite this experience and expertise, social workers may find themselves excluded from policies and programs designed to promote ACP. For example, 2015 Medicare regulations reimburse physicians, nurse practitioners, and physician assistants for limited ACP discussions, but exclude social workers from such payments. 13 While this proposal is an important step forward in promoting ACP, it may prevent social workers—major providers of ACP services—from being appropriately reimbursed for their services and expertise.
Few data are available on how ACP is implemented in current practice. In particular, there are currently no studies describing the involvement of social workers in ACP across the United States. To address this gap in knowledge, the Social Work Hospice and Palliative Care Network (SWHPN)—a professional organization representing hospice and palliative care social workers—partnered with the National Hospice and Palliative Care Organization's (NHPCO) Social Work Section to conduct a survey of social workers in the fall/winter 2015 to collect data about ACP practices. Additionally, this study was developed to provide data to policy-makers, including the Center for Medicare and Medicaid Services (CMS), about (1) the degree to which social workers in hospice and palliative care settings are having ACP conversations with patients and their families; and (2) the extent of their various functions and activities on the healthcare team when these discussions occur. SWHPN provided CMS with preliminary data from this study to advocate for including social workers in the new CMS regulations on reimbursement for ACP discussions.
Methods
Design
We used a cross-sectional, web-based, self-report survey (using SurveyMonkey 14 ) of social workers employed in hospice, palliative care, and related settings to explore their role, participation, and competency in facilitating ACP discussions. Survey participants were recruited from two main sources: (1) a SWHPN e-mail distribution list, which included ∼4000 e-mail addresses for members, former members, SWHPN conference participants, and allied organizations and professionals (955 individuals from this group opened the survey); and (2) NHPCO November 2015 electronic Newsbriefs newsletter, disseminated to members of the NHPCO professional practice membership group, with a companion survey link posted to the Social Work Section website. There is likely overlap between both organizations' distribution lists. The data collection period spanned from August to December 2015. Due to a lack of information about our sampling pool, precise estimates of the response rate are unavailable. Participation was entirely voluntary and respondents provided informed consent before beginning the survey. Respondents were not compensated for their time. Study procedures were approved by the Yeshiva University Institutional Review Board.
Sample
The sample included social workers from hospice, dedicated inpatient and outpatient palliative care, and related settings. To isolate respondents who interact with patients and families in their clinical practice—and who therefore have an opportunity to engage in ACP discussions—we constructed a subsample of respondents who reported having a current patient caseload (the clinical sample).
Measures
Demographics
The survey included items about respondents' gender, race/ethnicity, education, employment status, job role, practice setting, years of hospice/palliative care work experience, and patient caseload size. Based on U.S. census tract delineations, geographic region was determined using respondent's IP address, which is estimated to be ≥95% accurate. 15
ACP roles, responsibilities, and behaviors
Respondents provided information about ACP roles, responsibilities, and activities for social workers. Specifically, they were asked whether social workers in their respective department/agency are conducting ACP conversations with patients/families [Yes/No]; whether social workers are responsible for ensuring that patients are informed about ACP options in their given practice setting [Yes/No]; and whether social workers are primarily responsible for documenting patient/family preferences about ACP in their setting [Yes/No].
Respondents were also asked several questions about how often they engage in ACP with patients and families: “In a typical month, how often do you participate in advanced care planning discussions with patients or families?” Six possible responses were offered and coded as follows: 1 = Never/hardly ever; 2 = 1–2 times; 3 = 3–5 times; 4 = 6–10 times; 5 = 11–20 times; and 6 = More than 20 times. Using the same response set, participants were also asked about the frequency with which they lead ACP discussions: “In a typical month, how often do you lead advanced care planning discussions with patients or families?”
Additionally, to understand whether ACP conversations were generally single conversations or an ongoing series of discussions, the survey posed the following: “In a typical ACP process with a patient/family, how many sessions/discussions are required?” Four response possibilities were given: 1, 2, 3, or more than 3.
Self-rated competency
Respondents in the clinical sample were asked to assess their own competency with conducting ACP conversations using a single item measure: “On a scale of 1–10, how would you rate your competence in facilitating advanced care planning discussions with patients and families?” Response options ranged from 1 = not at all competent to 10 = expert competence.
Analysis
Data were cleaned to eliminate duplicates and cases with substantial missing variables (>50% of variables missing—not due to skip logic). In this process, 41 cases were deleted, thus reducing the initial sample from 690 cases to 641.
Among the 641 respondents in the full sample, 144 indicated a caseload of zero, while 41 cases had missing data for the caseload item. This left 456 cases (71% of the full sample) in the main analytic sample (i.e., the clinical sample), which consisted exclusively of respondents reporting a patient caseload.
Sample characteristics for both the full sample and clinical sample of respondents with a patient caseload were summarized using frequencies and percentages for key demographics. Descriptives for variables describing ACP practices were conducted for the clinical sample. The clinical sample was also exclusively used for all bivariate analyses. Bivariate tests (i.e., chi-square for nominal data, Kruskal–Wallis test for ordered categorical data; and analysis of variance [i.e., ANOVA] with Bonferroni's correction for continuous data) explored differences for the following practice settings of interest: community-based hospice, community-based palliative care, inpatient hospice, and inpatient palliative care and oncology. When reporting frequency of involvement in ACP discussions (ordered categorical data), we present means as well as medians to facilitate interpretation of results. Spearman's correlation coefficient was used to determine the strength and direction of the relationship between self-rated competency and (1) years of hospice/palliative care experience; (2) frequency participating in ACP discussions; and (3) frequency leading ACP discussions.
Results
Full sample
As shown in Table 1, 676 respondents were included in the full sample, most of whom were female (88.5%), white (88.3%), and with a masters-level social work degree or higher (93%).
The clinical sample includes only respondents with a patient caseload.
LCSW license typically requires an MSW or equivalent graduate degree. Not all states have licensing and licensing nomenclature varies by state.
Clinical sample
Table 1 also shows that 456 respondents reported having a current patient caseload and were thus included in the clinical sample. Among these respondents, 90% were female, 88% white, and most (87.3%) were employed full-time. Over three-quarters (77%) reported their primary job role as clinical social worker with the second most common response (11%) being multiple roles. Based on U.S. census tract categories, respondents were geographically dispersed across the United States. Caseload size varied widely. Nearly half (46.9%) reported having a patient caseload ranging from 1 to 39, while 53.1% had caseloads of 40+. The clinical sample was relatively seasoned, with 57.2% reporting six or more years of hospice/palliative care experience. Respondents came from a range of settings, with the majority (32.5%) coming from community-based hospice, 20.2% from oncology, and 16.2% from inpatient palliative care.
ACP roles, responsibilities, and behaviors
As shown in Table 2, among respondents in the clinical sample, the vast majority reported that social workers in their department/facility are conducting ACP discussions with patients and/or families (96.3%). Nearly four-fifths (79.6%) indicated that social workers in their department/facility are responsible for ensuring that patients/families are informed about ACP options. Two-thirds reported that social workers in their department/facility are primarily responsible for documenting ACP (67.8%).
ACP, advance care planning; SD, standard deviation.
The vast majority (97%) of clinical social work respondents reported being involved in ACP discussions in a typical month. Similarly, a large proportion (93%) of respondents indicated taking the lead in such discussions in a given month. In fact, over two-thirds (69%) reported that they participate in ACP discussions at least six or more times per month, while slightly fewer (60%) reported leading ACP discussions at least six or more times in the typical month. Seventy-eight percent reported that ACP sessions/discussions require at least two or more encounters.
Self-rated competency
When asked about their level of competence in facilitating ACP discussions, respondents generally rated themselves highly. With higher ratings indicating greater competence, the mean rating was 8.0 (standard deviation [SD] = 1.6) on a 1–10 scale. Just under a fifth of the clinical sample (18.6%) rated themselves a 10, the highest possible competency rating, and two-thirds (67.3%) rated themselves either an eight or higher.
Differences by practice setting
When considering ACP discussions by practice setting, there were significant differences. As displayed in Figure 1, differences were found in whether social workers are primarily responsible for documenting ACP preferences (p < 0.001) and whether they are responsible for informing patients/families about ACP options (p < 0.001). In general, social workers in oncology and inpatient palliative care settings were less likely to be responsible for documenting ACP and ensuring that patients/families are informed about ACP options.

Social workers' ACP responsibilities by practice setting. SWs, social workers; ACP, advance care planning. Differences across settings were statistically significant for both ACP responsibilities (i.e., documenting and informing; p < 0.001).
Practice settings also differed in terms of the frequency of social work involvement (p < 0.001) and leadership (p < 0.001) in ACP discussions. As shown in Figure 2, oncology social workers were also less frequently involved in ACP discussions (median 3–5 times/month) than other settings. When focusing on social work leadership in ACP discussions, most social workers reported leading ACP conversations on a routine basis (Fig. 3). However, oncology social workers reported that they less frequently had a leadership role in ACP discussions (median 3–5 times/month) relative to other practice settings.
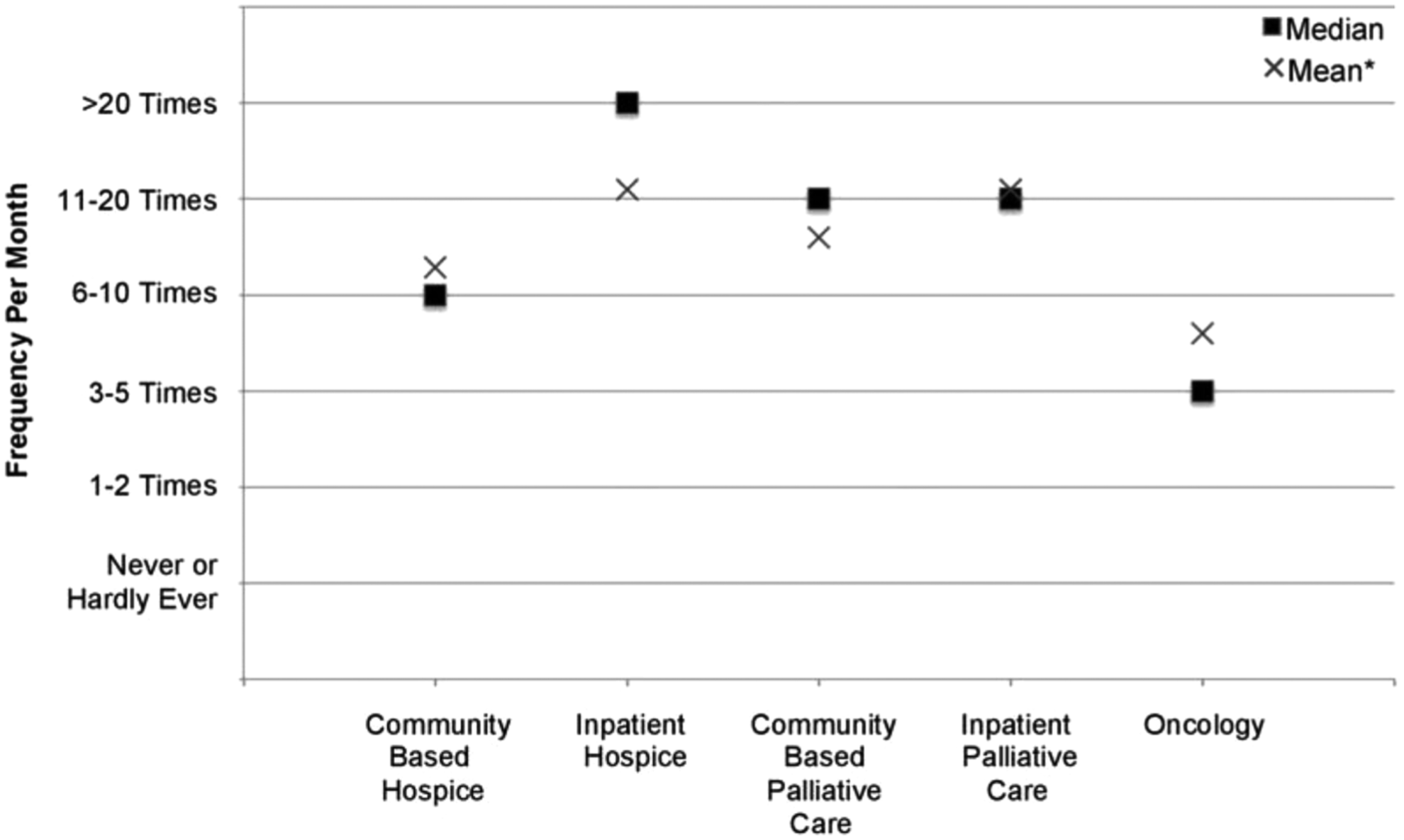
Frequency of social work participation in ACP discussions with patients or families by setting. *Mean and median values are reported to illustrate the central tendency of responses. Means are derived from the following coding scheme: 1 = Never/hardly ever; 2 = 1–2 times; 3 = 3–5 times; 4 = 6–10 times; 5 = 11–20 times; and 6 = More than 20 times.

Frequency of social work leadership in ACP discussions with patients or families by setting.*Mean and median values are reported to illustrate the central tendency of responses. Means are derived from the following coding scheme: 1 = Never/hardly ever; 2 = 1–2 times; 3 = 3–5 times; 4 = 6–10 times; 5 = 11–20 times; and 6 = More than 20 times.
Self-rated competency to facilitate ACP discussions (1–10) differed by setting (p = 0.034), but post hoc tests to isolate differences were not statistically significant. Oncology social workers rated themselves lowest, with an average rating of 7.6 (SD = 1.7), while inpatient hospice social workers rated themselves highest (M = 8.7; SD = 1.4).
Other associations with competency
Years of experience in hospice/palliative care positively correlated with self-rated competency to facilitate ACP discussions (Spearman's rho = 0.41, p < 0.001). Additionally, self-rated competency positively correlated with frequency of participating in, and leading, ACP discussions with patients or families (Spearman's rho = 0.32 and 0.38, respectively, p < 0.001 for both). Self-rated competency, however, did not differ by education (i.e., as indicated by highest social work degree) or licensure.
Discussion
This is the largest known study describing the ACP practices of social workers in hospice and palliative care settings in the United States. While many hospice and palliative care social workers know of their own meaningful involvement with ACP, there is scant evidence documenting these roles and responsibilities. This study has clarified the prominent level of involvement, suggesting that most social workers in palliative care-related settings contribute to ACP through an array of critical activities—patient and family education, facilitating discussions, documenting discussions or plans, and team leadership.
Strikingly, the vast majority (97%) of respondents with clinical responsibilities reported being involved in ACP discussions on a regular basis (at least monthly) and 93% reported leading such discussions. Thus, our evidence suggests that social workers are heavily involved in facilitating ACP discussions on a routine basis. To ensure individuals are adequately informed about their ACP options—and that their treatment preferences are honored—healthcare providers and policy-makers should both recognize and support the prominent and indispensable role social workers have in conducting ACP discussions. This role is likely rooted within a strong interdisciplinary network as a defining characteristic of palliative care is the complementary involvement of peer disciplines such as nursing, medicine, and chaplaincy. Future research should examine how interdisciplinary teams delegate ACP responsibilities among team members.
Despite high levels of reported involvement in ACP activities across all settings, educating individuals and their families about ACP options and documenting ACP preferences differed among settings in meaningful ways. Higher proportions of hospice social workers, whether working in residential or community-based care, and community-based palliative social workers performed these activities than their hospital-based colleagues in palliative care and oncology. This finding may reflect greater opportunity for hospice social workers on interprofessional teams to develop ACP activities than hospital-based social workers. 16 Other possibilities for this finding may be that hospitalization is often a time of crisis and is not the ideal setting for ACP or that hospital stays are too short for the relationship-building and multiple discussions that may be needed for effective ACP. 17 Furthermore, hospital-based practice may reflect the physician-led medical model, with physicians and nurses more likely to perform these functions than social workers; ACP may be viewed more as a team responsibility in hospice and other community settings. 18 Additional research is needed to explore differences across settings.
Our findings suggest high levels of self-rated competency among social workers conducting ACP activities, with two-thirds of respondents (67%) rating themselves an eight or higher (on a 1–10 scale). It is expected that few MSW programs provide formal education on ACP; therefore, social workers are likely to acquire these skills through on-the-job experience, shadowing skilled professionals, and mentorship. Social workers with strong ACP skills are vital resources for educating other social workers and team members, as well as for competent provision of care. However, ratings of self-competency are by nature subjective and are not based on objective standards. With calls for greater use of ACP, such as from the National Academy of Medicine (formerly the Institute of Medicine), a consensus is needed on the requisite knowledge and skills necessary for competent ACP practice, in addition to objective measures of competency across health professions.
Limitations
This study used nonprobability sampling methods, which limit the generalizability of the resulting data. Additionally, we were unable to determine the impact of non-response due to a lack of information about non-responders; it is possible that non-response bias may have impacted results. This being said, the sample was dispersed geographically and respondents reported working in a variety of practice settings, which suggests that respondents represent a broad cross section of social workers affiliated with hospice and palliative care.
Some survey items may have been interpreted differently by different respondents, thus complicating the interpretation of results. For example, we asked respondents whether they were primarily responsible for documenting patient/family ACP preferences. It is possible to interpret this item as asking whether the primary role of the social worker is to document ACP (rather than engage in other activities), or whether the social worker is the one who is primarily responsible for documenting ACP (among the members of the healthcare team). Future work should clarify the social worker's role in documenting ACP.
Our sample was relatively homogeneous, with only 8% of respondents identifying themselves as nonwhite (Table 1). This suggests a pressing need for greater diversity among hospice and palliative social work professionals and may have implications for diversity among other palliative care professionals as well. Greater diversity in the profession may, in turn, help address the disconcerting racial/ethnic disparities observed in hospice and palliative care as African Americans and Latinos are less likely to access these services.
While this survey provided respondents opportunities to elaborate on their answers through open-ended responses—which will be analyzed in a separate article—qualitative research is needed to better comprehend the ACP perspectives and experiences of hospice and palliative care social workers.
Conclusion
Social workers are core members of the healthcare team performing ACP. These findings provide compelling evidence that social workers frequently play a prominent role in ACP discussions. A majority of our sample of social workers work to ensure that patients and families are educated about ACP options, as well as participate in, lead, and document ACP discussions. Therefore, providers and administrators should support social work participation in their ACP programs. Furthermore, policy-makers, including CMS, should incorporate the contributions of social workers in policies and programs supporting ACP, such as those that reimburse healthcare professionals for their time when engaging in ACP conversations.
Footnotes
Author Disclosure Statement
No competing financial interests exist.