
Abstract
Abstract
Background:
Discussing goals of care and advance care planning is beneficial, yet how to best integrate goals of care communication into clinical care remains unclear.
Objective:
To develop and determine the feasibility of a structured goals of care communication guide for nurses and social workers.
Design/Setting/Subjects:
Developmental study with providers in an academic and Veterans Affairs (VA) health system (n = 42) and subsequent pilot testing with patients with chronic obstructive pulmonary disease or heart failure (n = 15) and informal caregivers (n = 4) in a VA health system. During pilot testing, the communication guide was administered, followed by semistructured, open-ended questions about the content and process of communication. Changes to the guide were made iteratively, and subsequent piloting occurred until no additional changes emerged.
Measurements:
Provider and patient feedback to the communication guide.
Results:
Iterative input resulted in the goals of care communication guide. The guide included questions to elicit patient understanding of and attitudes toward the future of illness, clarify values and goals, identify end-of-life preferences, and agree on a follow-up plan. Revisions to guide content and phrasing continued during development and pilot testing. In pilot testing, patients validated the importance of the topic; none said the goals of care discussion should not be conducted. Patients and informal caregivers liked the final guide length (∼30 minutes), felt it flowed well, and was clear.
Conclusions:
In this developmental and pilot study, a structured goals of care communication guide was iteratively designed, implemented by nurses and social workers, and was feasible based on administration time and acceptability by patients and providers.
Introduction
S
There are a number of patients, providers, and system barriers to integrate goals of care communication into clinical care.8–14 To address some of these barriers, specifically patient difficulty in identifying values and lack of physician time, we built on others' work7,15–19 to develop a structured goals of care communication guide for nurses and social workers. Such a guide could be used by a range of healthcare providers to help patients to identify their healthcare values, enhance illness understanding, and increase patient readiness to engage in other advance care planning steps with their physicians, such as having prognosis discussions and documenting their wishes in legal documents. Here we describe the development and pilot testing of a structured goals of care communication guide.
Methods
Development
The communication guide was developed to facilitate goals of care communication among patients, families, and healthcare providers in the outpatient or home setting. The following objectives shaped the development of the communication guide: (1) be within the scope of practice for a general medical nurse or social worker, (2) be salient across different serious illnesses, (3) be structured to promote reproducibility and scalability, (4) yield clinically relevant results that can be integrated into the medical record, and (5) provide a clear path for next steps in goals of care communication. Building on prior work,7,15–19 a nurse (J.P.), social worker (R.J.-K.), and physician (D.B.B.) jointly developed the initial goals of care communication guide.
The initial guide included questions for nurses or social workers to initiate goals of care communication, provided scripts to anticipate and respond to patient reactions, and included ways to customize questions and response options. This guide was presented for feedback to a group of 6 multidisciplinary palliative care researchers (physicians, psychologists, and nurses), and subsequently to a larger group of 30 multidisciplinary providers (chaplains, social workers, nurses, and physicians) from multiple specialties (primary care, geriatrics, oncology, and palliative care). The guide was additionally reviewed separately by several other nurses, a palliative care psychologist, and two advance care planning and communication researchers.
Pilot testing
We piloted the goals of care communication guide with a convenience sample of patients with New York Heart Association (NYHA) III or IV heart failure or Global Initiative for Obstructive Lung Diseasse (GOLD) III or IV chronic obstructive pulmonary disease (COPD) from the VA Eastern Colorado Health Care System who would be able to provide feedback on the guide. This population was chosen in preparation for a clinical trial that is evaluating the effect of palliative care in heart failure and COPD. 20 There were no exclusion criteria. Patient demographic/clinical information was not collected because analyses based on this information were not planned. Informal caregivers were present per participant request. This study was reviewed by the Colorado Multiple IRB and deemed exempt.
A social worker and nurse took turns using the guide to lead one-on-one patient or patient and surrogate goals of care discussions. Study staff took notes during the discussions, and these notes along with social worker and nurse observations and reactions (elicited after each goals of care discussion) were compiled in a semistructured debrief form (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/jpm). After the discussion, patients were asked semistructured, open-ended questions (Supplementary Fig. S2) to obtain reactions to the communication guide as well as to elicit feedback regarding improvements.
Process for making revisions
Revisions to the communication guide were made after input from patients and healthcare providers at each step of guide development and refinement based on consensus within the core analytic team (J.P., R.J.K., and D.B.B.). During pilot testing, data from the patient interviews and the nurse/social worker debriefing form were placed into a matrix and compared and contrasted throughout the study to identify commonalities that should lead to changes in the goals of care communication guide. 21 The core analytic team discussed communication guide changes every three to five patients. Pilot testing was continued until no new information was obtained from patients or nurse/social worker debriefing. After pilot testing was completed and feedback incorporated, the revised communication guide was reviewed by a VA-based clinical team comprising a geriatrician, pulmonologist, internist, and cardiologist to obtain additional perspectives.
Results
Development
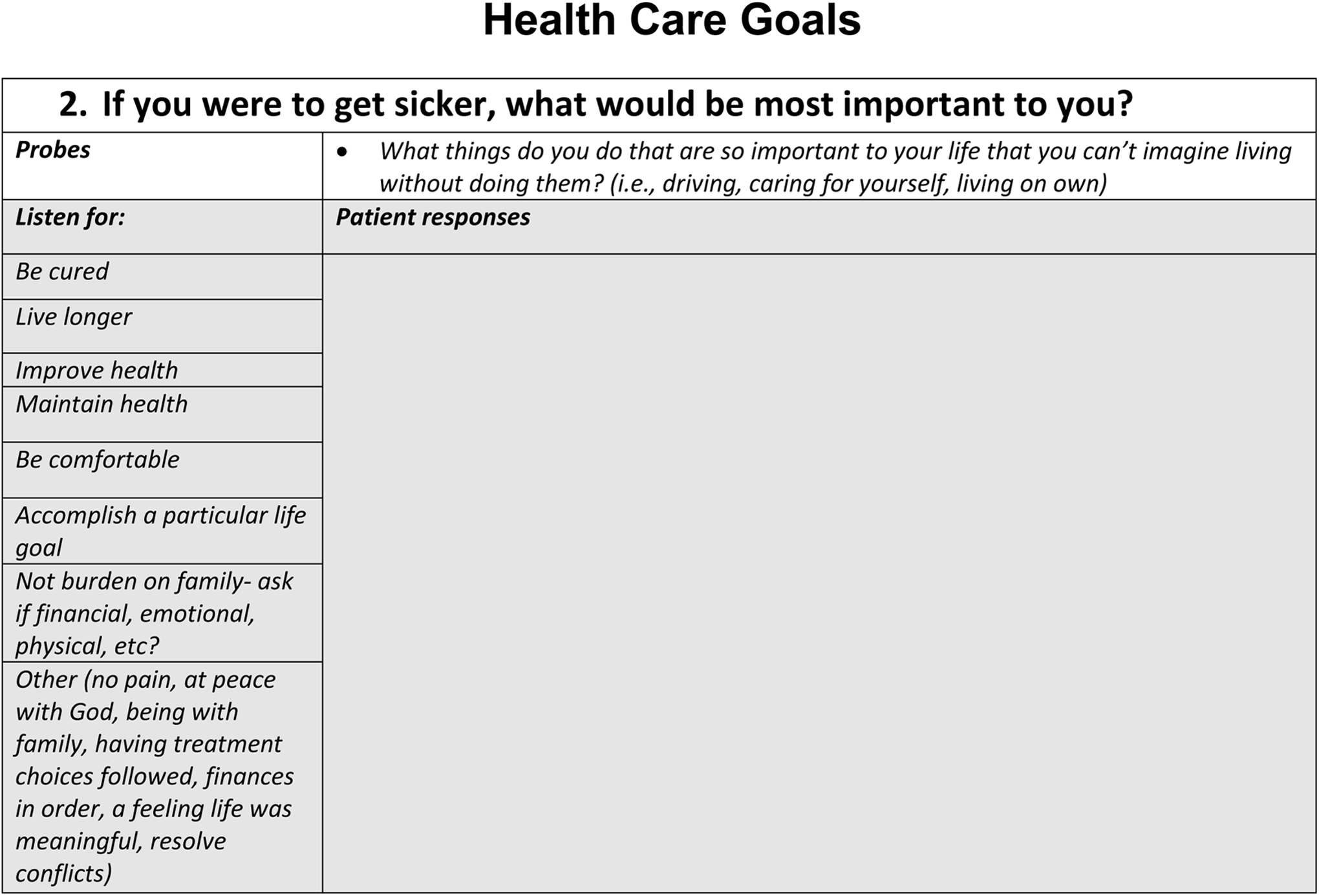
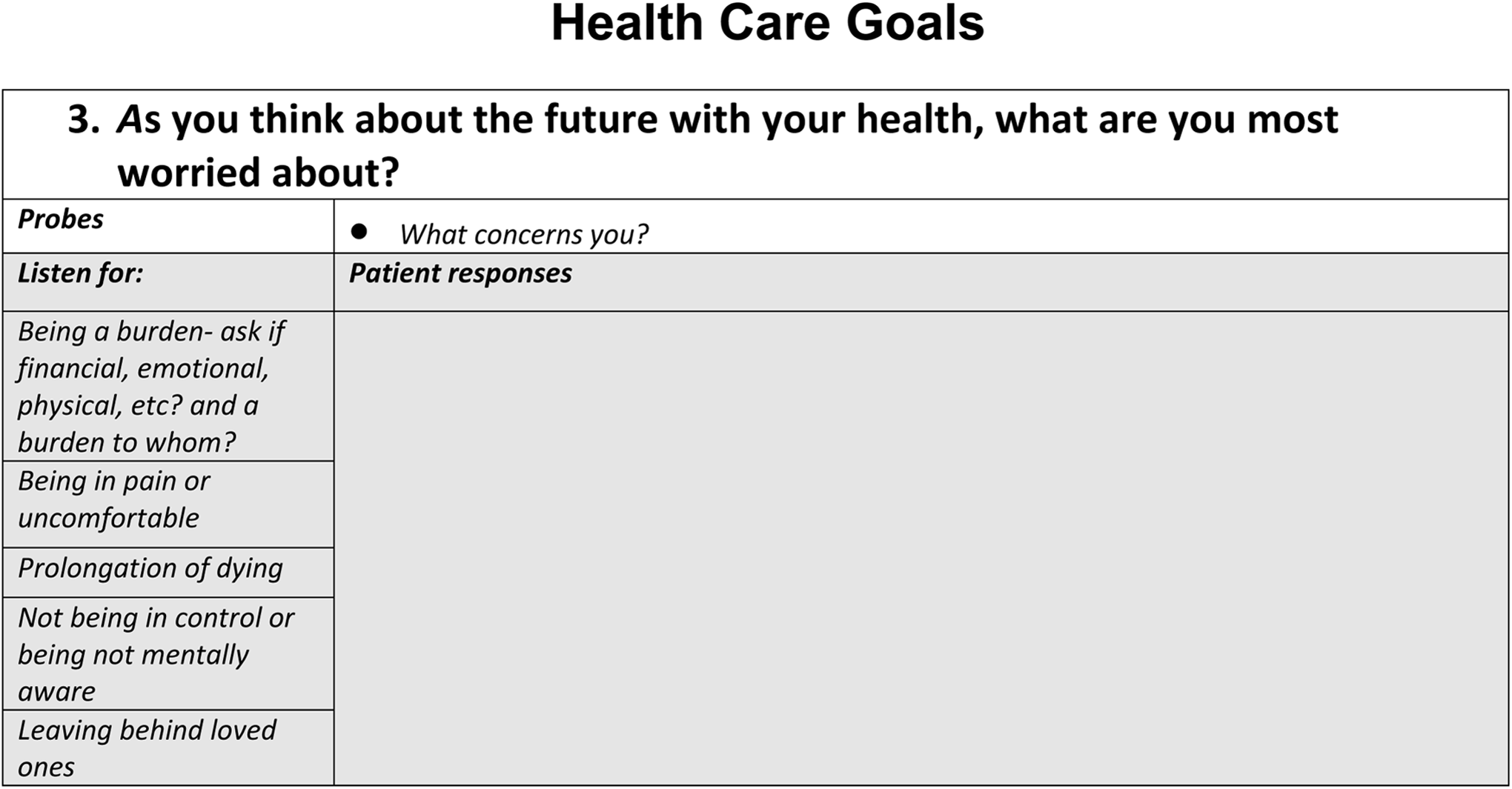
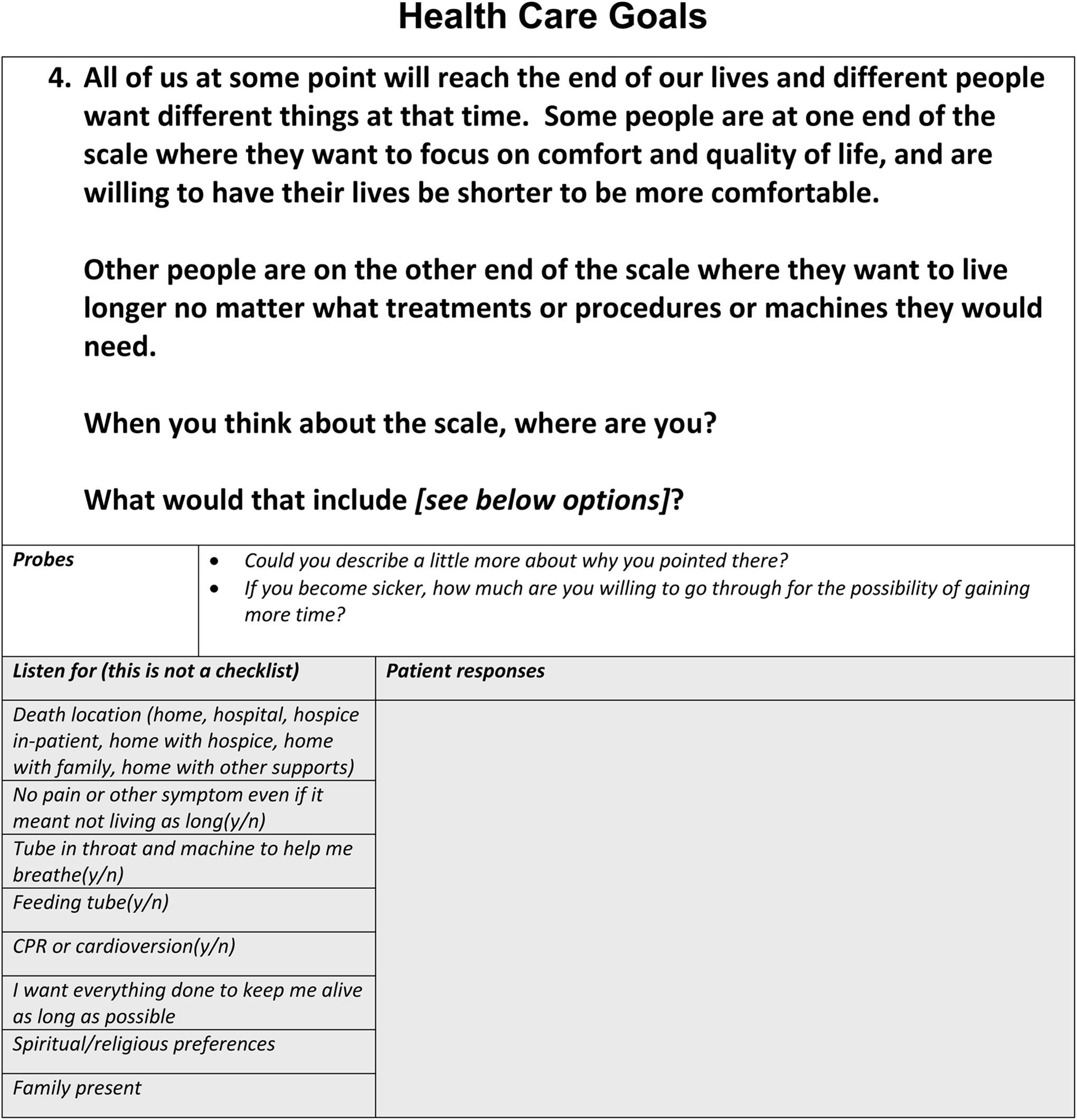
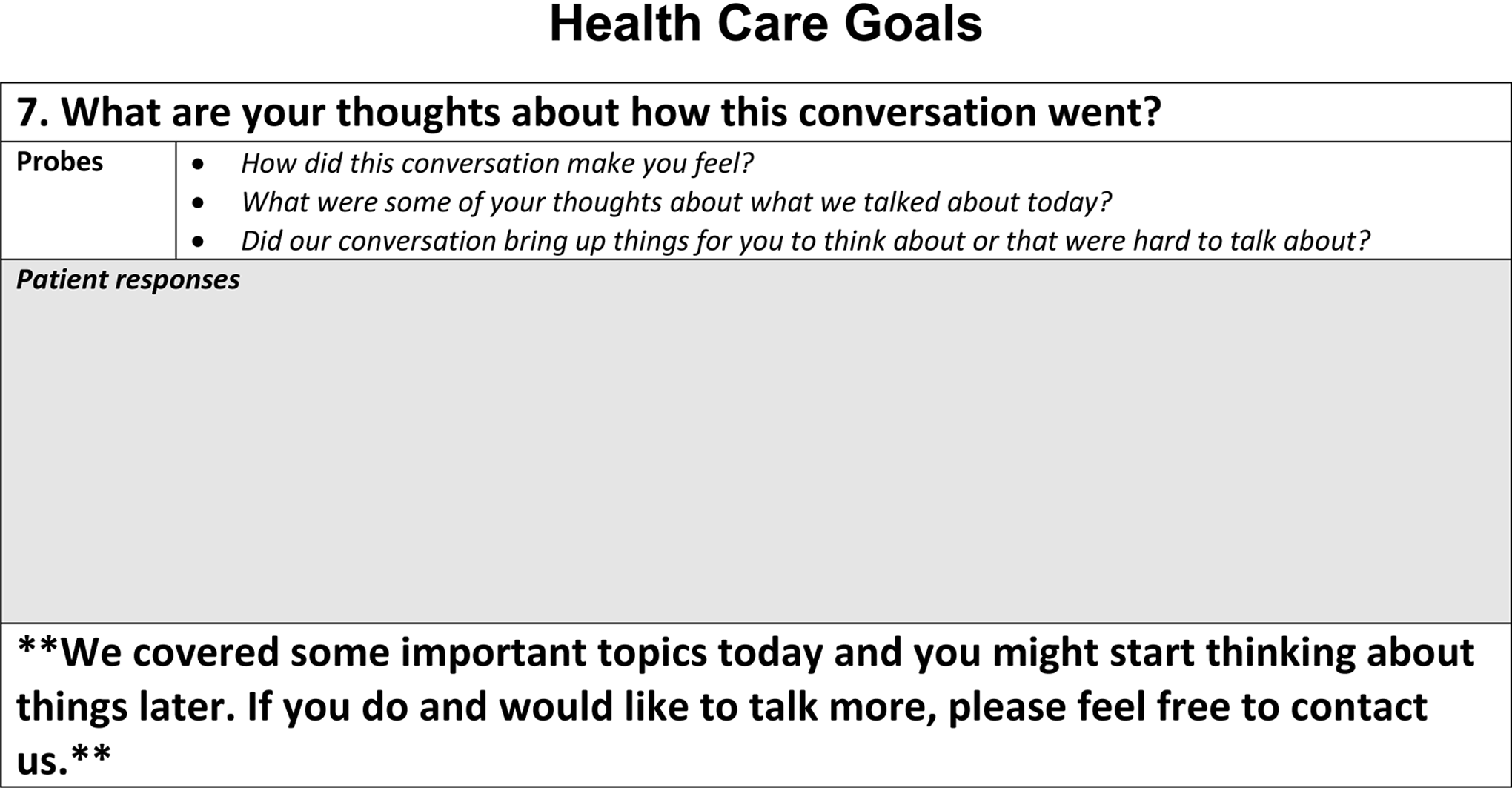
Iterative input resulted in the goals of care communication guide. The guide included questions to (1) elicit patient understanding of and attitudes toward the future of illness, (2) clarify values and goals, (3) identify positive and negative perceptions and feelings about the future, (4) identify end-of-life preferences, (5) motivate patients to complete written documents and speak with family and providers about values and goals, and (6) agree on a follow-up plan.
Multidisciplinary providers recommended changes to increase brevity, improve the clarity of certain questions, and include questions pertaining to documentation of healthcare goals. For example, the initial question was changed from “What is your understanding now of where you are with your illness” to “What has your doctor told you about your illness?” At this stage of development, the communication guide included multiple prompts, anticipated reactions from patients alongside suggested responses, and ways to customize each question.
Pilot testing
During pilot testing, 15 patients and 5 of their informal caregivers participated (17 patients were approached, 2 refused and 1 agreed but ultimately did not participate). Every patient said this was an important topic; none said the goals of care communication should not be conducted. For example, one patient said, “It is necessary. It takes the guesswork out of what other people should be doing for you. I am thinking about my daughter; she doesn't have to anguish over what I do want and don't want. It clears everything up.”
The communication guide prompts, anticipated reactions, and ways to customize each question were removed and placed into a user manual because they distracted from the main communication guide questions, were uncommonly used, and cluttered the guide. Removing this text also allowed for greater spontaneity and flexibility.
Major substantive revisions (all of which were made during piloting among the first 10 patients) are listed in Table 1. The communication guide wording was changed for each question. Patients and informal caregivers found the length acceptable (∼30 minutes), felt it flowed well, and was clear. The final communication guide is presented in Figure 1. No changes were made during piloting in the final five patients or with review by the VA-based clinical team.

Goals of Care Communication Guide.


MOLST, medical orders for scope of treatment; POLST, physician orders for life-sustaining treatment.
Discussion
We developed and revised a structured goals of care communication guide based on providers' feedback and pilot testing among patients with heart failure and COPD. The communication guide was designed for social workers and nurses to initiate and facilitate further discussions and actions among patients, family members, and healthcare providers. In this small study, the goals of care communication guide was feasible based on administration time and acceptability by patients and providers.
Weiner et al. 22 advocated for the need to formally develop communication interventions through a series of steps, based on a similar process used in the development of psychotherapeutic interventions such as interpersonal psychotherapy. 23 Our study represents such an effort. Key strengths of our approach include the grounding in prior literature and the iterative development and refinement of the communication guide using patients and a diverse sample of providers. Challenges included how to balance the need for communication guide structure with flexibility for the providers based on patient questions or responses, how to balance the need for brevity with comprehensiveness, and how much detail to place in the communication guide versus a user manual.
Although this intervention builds on substantial work in goals of care communication and advance care planning, this is a developmental and feasibility study and should be interpreted in that context. Based on our results, and given the significant time constraints of physicians, it is possible that nurses and social workers can use this guide during stand-alone visits to prepare patients and family members for further conversations and treatment decisions. Depending on the experience and expertise of the practitioner, different levels of training and supervision would likely be helpful in using the guide. The intervention was pilot tested in a mostly white and male VA population with serious lung and heart diseases. Further testing is needed in other illnesses, patient populations, and over time to explore how it works in coordination with other members of the medical team; how training and supervision can be tailored based on provider and patient needs and context; and how to adapt it for longitudinal use. Future studies could also explore whether the communication guide is useful in the context of speaking with a surrogate decision maker or for others besides nurses and social workers who are involved in caring for those with serious illness.
In summary, a structured goals of care communication guide developed for nurses and social workers was iteratively developed with multidisciplinary providers and patients and was acceptable to patients during pilot testing. Further testing of this intervention is planned in a VA-funded clinical trial. 20
Footnotes
Acknowledgments
The authors thank Alexandra Tillman for her help with data collection. The contents of this article do not represent the views of the United States Department of Veterans Affairs or the United States Government. This work was supported, in part, by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development grant HSR&D IIR 14-346. This work was supported by VA Career Development Award 08-022 from the United States Department of Veterans Affairs Health Services Research and Development Program. Dr. Bekelman was supported by NIH grant R01-NR014.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.