
Abstract
Abstract
Background:
Methadone (ME) is commonly used in pain and palliative care (PPC) patients with refractory pain or intolerable opioid adverse effects (AEs). A unique ME AE is its corrected QT (QTc) interval prolongation risk, but most evidence exists in methadone maintenance therapy patients.
Objective:
Our goal was to identify QTc interval prolongation risk factors in PPC patients receiving ME and other medications known to prolong the QTc interval and develop a risk stratification tool.
Design:
We performed a case–control study of adult inpatients receiving ME for pain management.
Settings/Subjects:
Adult inpatients receiving ME with a QTc >470 msec (males) and >480 msec (females) were matched 1:2 according to age, history of QTc prolongation, and gender with ME patients who did not have a prolonged QTc interval. QTc prolongation risk factors were collected for both groups. Covariates were analyzed using conditional logistic regression. Classification and regression tree analysis was used to identify the ME dose associated with QTc prolongation.
Results:
Predictors of QTc prolongation included congestive heart failure (CHF) (OR: 11.9; 95% CI: 3.7–38.2; p < 0.00), peptic ulcer disease (PUD) (odds ratio [OR]: 8.3; 95% confidence interval [95% CI]: 2.4–28.9; p < 0.00), hypokalemia (OR: 6.5; 95% CI: 1.5–28.2; p < 0.01), rheumatologic diseases (OR: 4.7; 95% CI: 1.6–13.9; p < 0.00), taking medications with a known torsades de pointes (TdP) risk (OR: 4.4; 95% CI: 1.8–10.7; p < 0.01), malignancy (OR: 3.3; 95% CI: 1.2–9.3; p < 0.03), hypocalcemia (OR: 2.1; 95% CI: 0.9–4.8; p < 0.07), and ME doses >45 mg per day (OR: 1.9; 95% CI: 0.8–4.8; p < 0.16). Mild liver disease was protective against QTc prolongation (OR: 0.05; 95% CI: 0.0–0.46; p < 0.01).
Conclusions:
Predictors of QTc prolongation in our multivariate conditional logistic regression model included CHF, PUD, hypokalemia, rheumatologic disorders, use of medications with a known TdP risk, malignancy, hypocalcemia, and ME doses >45 mg per day.
Introduction
M
Methods
Patients
This was a case–control study. Potential subjects were identified through pharmacy records at the University of Rochester Medical Center's (URMC) Strong Memorial and Highland Hospitals between March 14, 2011, and March 14, 2014. Adult inpatients who received methadone for at least one week before hospitalization and had an electrocardiogram (ECG or EKG) obtained within two weeks before admission or during the first 24 hours after hospital admission were included. Patients receiving MMT for substance abuse, admitted as a hospice encounter, age <18 years, or had incomplete medical records were excluded. ECGs included within the patient's electronic medical record were used to determine the presence or absence of QTc interval prolongation. All ECGs were previously reviewed by an attending cardiologist for accuracy. QTc is calculated at URMC using Bazett's correction formula. 10 QTc interval prolongation was defined as QTc interval >470 msec (males) and >480 msec (females) or a QTc interval increase >60 msec from baseline following the definitions from the American Heart Association/American College of Cardiology Foundation (AHA/ACCF) and FDA.11,12 The AHA/ACCF definition was selected because it differentiates between genders. The FDA definition of a >60 msec increase was chosen since it represents a more clinically significant change than >30 msec.
Patients with a prolonged QTc interval were designated as cases, whereas those without QTc interval prolongation were classified as controls. Cases and controls were matched 1:2 according to age range by decade, gender, and history of QTc prolongation.
Procedures
The following data were obtained from each patient's medical records: age, sex, comorbidities, history of QTc interval prolongation, baseline QTc interval and uncorrected QT interval, heart rate at time of baseline QT/QTc interval, history of structural heart disease (e.g., myocardial infarction, heart failure, valvular disease, or cardiomyopathy), history of bradycardia, history of conduction disorders (e.g., bundle branch block, heart block, arrhythmias, syncope, or long Q-T syndrome), and electrolyte abnormalities at the time of initial inpatient laboratories (e.g., hypokalemia, hypomagnesemia, or hypocalcemia). 7 Hypokalemia was defined as K+ <3.3 mEq/L, hypomagnesemia as Mg2+ <1.3 mEq/L, and hypocalcemia delineated as a corrected Ca2+ <8.8 mg/dL based on our health system's laboratory reference range. The Charlson comorbidity index was used to calculate comorbidity scores. 13 Concurrent use of other QTc-prolonging medications as classified by CredibleMeds.org was collected. 14 This website categorizes medications into four classes based on TdP risk (e.g., medications with a known risk of TdP, possible risk of TdP, conditional risk of TdP, and drugs to avoid in congenital long QT). Use of medications that increase serum methadone concentrations such as but not limited to fluconazole, fluoxetine, paroxetine, sertraline, ciprofloxacin, amitriptyline, desipramine, and voriconazole was included.15,16 Methadone indication, scheduled dose, route, frequency, and duration of use at the time of inpatient admission were obtained. Breakthrough methadone doses were not included in the methadone daily dose calculations. One investigator evaluated all the electronic medical records and collected patient data. This study was approved by the URMC Institutional Review Board, and the requirement for informed consent was waived.
Statistical analyses
Assuming a prior methadone exposure of 40% in controls, we calculated a sample size of 90 case patients and 180 controls (ratio 1:2) for this study to have an 80% chance of detecting a clinically meaningful odds ratio (OR) of 2.5 between the two groups at the 5% significance level. This was deemed to be clinically significant and to necessitate a medication regimen adjustment. We compared the odds of case patients and controls through conditional logistic regression to account for the matching design. Demographic and baseline clinical characteristics between case patients and matched controls were compared using paired t tests for continuous variables and McNemar's chi-square tests for categorical variables. Variables with a p value <0.2 identified in the bivariate analysis were considered as potential confounders in a multivariable conditional logistic regression, using backward and forward stepping. We obtained an adjusted estimate of QTc prolongation by adjusting for covariables that significantly improved the likelihood of the model. Classification and regression tree analysis was used to identify the methadone dose associated with QTc prolongation. All reported p values and 95% confidence intervals (95% CIs) were two sided. A p value of <0.05 was considered to indicate statistical significance. STATA, version 13.1 (College Station, TX) was used for analyses.
Results
A total of 908 patients were screened for this study (Fig. 1). Two hundred ninety-nine patients were immediately excluded for the following reasons: 190 patients on MMT, 84 patients did not have a documented ECG, and 25 patients were <18 years. Three hundred ninety-one did not have a prolonged QTc interval, of which 180 patients were included as controls, and 211 patients were excluded for reasons outlined in Figure 1. Two hundred eighteen patients had a prolonged QTc interval. Ninety patients were classified as controls, 103 patients were identified with a prolonged QTc interval while matching case–controls, and 25 patients did not meet inclusion criteria as detailed in Figure 1.
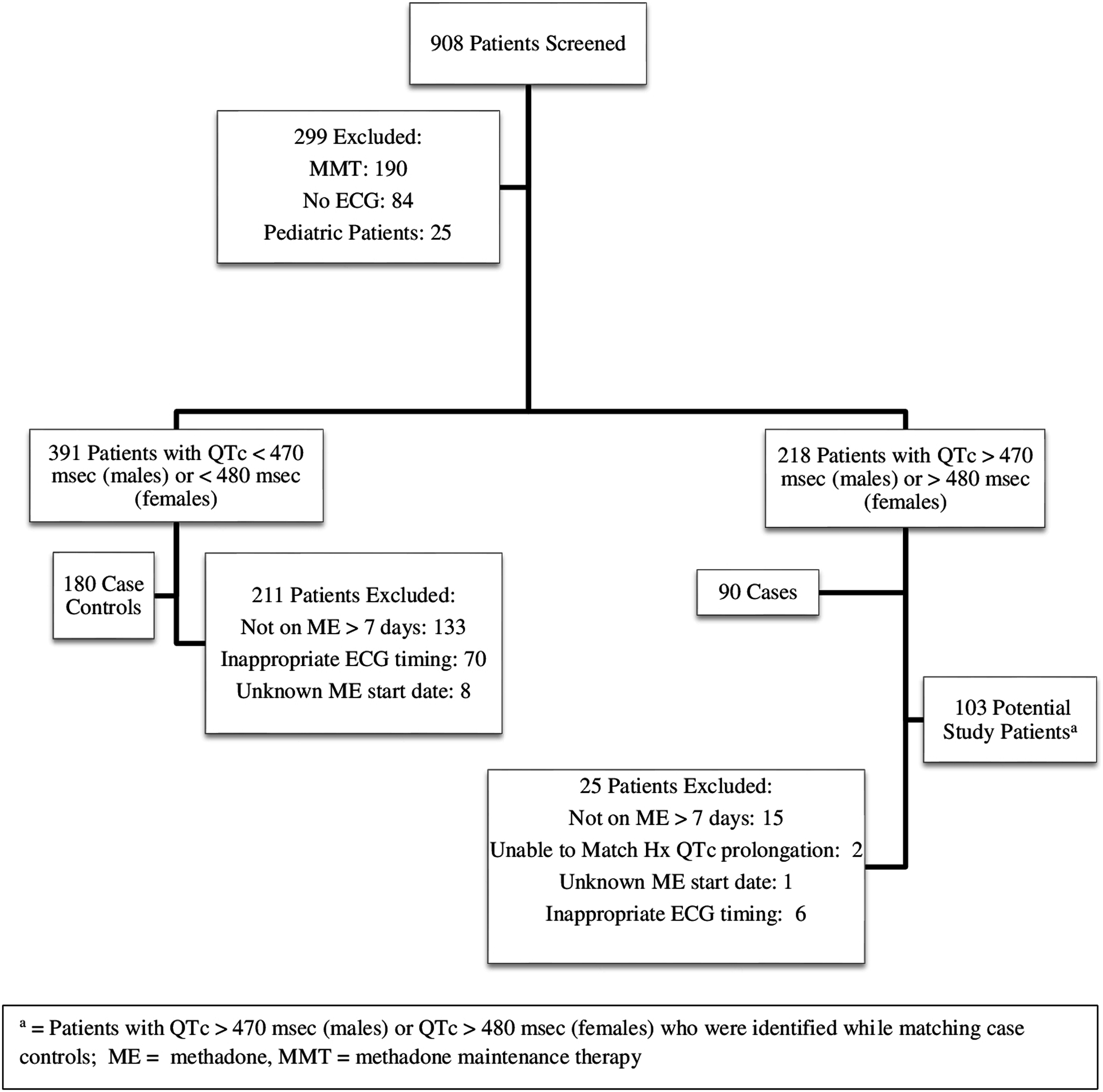
Patient screening. ECG, electrocardiogram; QTc, corrected QT.
Table 1 outlines patient demographics. Case patients had a median age of 55 years compared to controls whose median age was 57 years. No case or controls had a history of QTc prolongation. Among case and control patients, 56.7% were female and 43.3% were male. The mean total Charlson comorbidity score was 4.9 (standard deviation [SD]: 3.2) for cases and 4 (SD: 3.1) in controls. Among cases, methadone was indicated for chronic pain in 69 patients (76.7%), cancer pain in 19 patients (21.1%), and chronic and cancer pain in 2 patients (2.2%). One hundred fifteen control patients (63.9%) received methadone for chronic pain compared to 52 patients (28.9%) for cancer pain, and chronic and cancer pain in 13 patients (7.2%). The median ME dose was 36.3 mg (SD: 27.7 mg) in cases (range: 5 mg–120 mg/day) and 34.6 mg (SD: 29.9 mg) among controls (range: 5–240 mg/day). Cases used ME for a median of 199 days (SD: 302.9 days) before study entry and 197 days (SD: 318.3 days) for controls.
PEG, percutaneous endoscopic gastrostomy; SD, standard deviation.
Table 2 lists the variables from the univariate analysis included in the conditional multivariate logistic regression model. The final model was tested for collinearity, statistical interactions, and confounding variables. The results of our conditional multivariate logistic regression analysis are included in Table 3. The most significant variables to predict QTc prolongation in our multivariate conditional logistic regression model were congestive heart failure (CHF) (OR: 11.9; 95% CI: 3.7–38.2; p < 0.00), peptic ulcer disease (PUD) (OR: 8.3; 95% CI: 2.4–28.9; p < 0.00), hypokalemia (OR: 6.5; 95% CI: 1.5–28.2; p < 0.01), rheumatologic diseases (OR: 4.7, 95%: 1.6–13.9; p < 0.00), concurrent use of medications with known TdP risk (OR: 4.4; 95% CI: 1.8–10.7; p < 0.01), malignancy (OR: 3.3; 95% CI: 1.2–9.3; p < 0.03), hypocalcemia (OR: 2.1; 95% CI: 0.9–4.8; p < 0.07), and ME doses >45 mg/day (OR: 1.9; 95% CI: 0.8–4.8; p < 0.16). Mild liver disease decreased patient's QTc prolongation risk (OR: 0.05; 95% CI: 0.0–0.46; p < 0.01).
95% CI, 95% confidence interval; CART, classification and regression tree analysis; CHF, congestive heart failure; CVD, cerebrovascular disease; DM, diabetes mellitus; ECG, electrocardiogram; OR, odds ratio; QTc, corrected QT; TdP, torsades de pointes.
Discussion
We identified six studies in the literature that evaluated methadone's effect on QTc prolongation in PPC patients.17–22 Three studies identified other risk factors that contributed to ME-induced QTc prolongation.17,18,20 Price et al. identified increased risk of cardiac events (composite endpoint: QTc >500 msec, cardiac death, or hospitalization/emergency department visit for a cardiac etiology) in 1246 primary care chronic pain patients with oral ME doses ≥100 mg per day (OR: 6.18; 95% CI: 1.08–35.45) and increasing age (OR: 1.06; 95% CI: 1.03–1.09). 17 Female gender (p = 0.0061) and antidepressant use (p = 0.0397) were identified as risk factors for a prolonged QTc interval (>450 msec) in 90 chronic pain outpatients taking ME compared to controls without ME exposure. 18 Concurrent use of medications associated with QTc prolongation risk, structural heart disease, electrolyte abnormalities, and female gender was found to increase QTc prolongation risk (QTc interval increase >25% from baseline or ≥500 msec) in 100 palliative care patients receiving ME for cancer pain. 20 These studies utilized different definitions of QTc interval prolongation, so clinical judgment should be utilized when interpreting findings.
Our final multivariate logistic regression model identified CHF, PUD, hypokalemia, rheumatologic diseases, medications with a known TdP risk, malignancy, hypocalcemia, and ME doses >45 mg per day as potential risk factors, and mild liver disease had a protective effect against QTc prolongation in our chronic PPC patients. Methadone is most commonly prescribed by a limited number of specialists within our health system who care for PPC patients. Our findings may be influenced by local prescribing patterns, and the risk factors we identified in this study may slightly vary when compared to those identified for PPC patients in other geographic areas. The URMC palliative care service frequently collaborates with our institution's advanced heart failure and oncology programs. The large heart failure and oncology programs in our health system may account for the large number of patients with these risk factors in our model. Thirty-two case patients had heart failure compared to 19 control patients, and malignancy occurred in 22 case patients versus 18 control patients. Heart failure and hypokalemia are closely related risk factors given the frequent use of loop diuretics in this patient population and were also identified along with hypocalcemia as risk factors by Reddy et al. 20 Rheumatologic diseases were likely a risk factor because lupus nephritis is a common systemic lupus erythematosus complication and methadone is a preferred opioid in renal insufficiency. 23 PUD was an unexpected risk factor. Multiple variables may have contributed to this finding, including the potential for increased use of opioids versus nonsteroidal anti-inflammatory drugs (NSAIDs) for pain management with this comorbidity or through increased exposure to methadone via inhibition of CYP2C19 with concurrent use of proton pump inhibitors (PPIs). 24
It was expected that concomitant use of medications with a known TdP risk would have an additive effect on QTc prolongation risk given the frequent use of antipsychotics, antiemetics, and antidepressants for mental health comorbidities and symptom management in PPC patients. This was consistent with the findings of Reddy et al. 20 We did not assess the impact of dose, actual as-needed (e.g., prn) medication utilization, or route of administration in our risk assessment of other QTc prolonging medications. Differences in these risk variables may pose a higher QTc prolongation risk when comparing medication doses or selected routes of administration. For example, 6 mg of intravenous haloperidol has a higher QTc prolongation risk than 2 mg of oral haloperidol. Our model did not account for concurrent use of multiple QTc prolonging medications within the same risk class. A patient taking three medications with a known risk of TdP in addition to methadone likely has a higher risk of QTc prolongation than a subject taking methadone and one medication with a known risk of TdP. Methadone doses >45 mg per day were identified to increase QTc prolongation risk in our model. This dose is lower than the ≥100 mg per day dose that was identified by Price et al. 17 to increase cardiac event risk. It is unclear why mild liver disease decreased QTc prolongation risk in this study cohort. Hypokalemia, hypocalcemia, concurrent use of medications with known TdP risk, and ME doses >45 mg per day are potentially modifiable risk factors. Providers caring for PPC patients should correct or minimize these modifiable risk factors when clinically feasible. Heart failure, PUD, and rheumatologic diseases are less modifiable risk factors in PPC patients given the frequency of advanced stages of chronic illnesses and limited life expectancy in this population.
This study has several additional limitations that may have impacted our findings. Despite having one investigator collect and code all the data, there is still a potential for incomplete or miscoded data. Since many study patients were on ME before our health system's electronic medical record implementation or were initiated on methadone by a provider outside of our health system, we did not consistently have baseline ECGs or methadone start dates available for all patients. Bazett's correction formula is not as accurate as the Fridericia's correction formula for tachycardic and bradycardic patients. 12 We utilized the Bazett's correction formula for all study patients, which likely resulted in an overcorrected QTc interval in tachycardic patients and an undercorrected QTc interval in bradycardic patients. The small sample size made it difficult to compare various risk factors such as valvular heart disease due to low frequency of occurrence. Cardiac arrest and use of cardioversion were not included in our data collection since many of our palliative care patients had do-not-resuscitate orders.
One variable that we did not assess was the impact of pharmacogenomics. Findings from the MEMORIES trial demonstrated that MMT patients with a CYP2C19*2 gene variant had higher plasma concentrations of methadone's primary metabolite, ethylidene-1, 5-dimethyl-3,3-diphenylpyrrolidene (EDDP), than subjects with the wild-type gene (p < 0.004). 25 Elevated EDDP levels produced a nonstatistically significant increase in the QTc interval from baseline (p = 0.1). This pilot study draws attention to the potential influence of CYP2C19 variants on methadone-induced QTc interval lengthening.
This study included a heterogeneous patient cohort of chronic PPC patients. There are advantages and disadvantages of combining these two patient populations. Palliative care patients often have a shorter life expectancy and more severe symptoms making providers more accepting of a longer QTc interval or less likely to aggressively correct modifiable risk factors because the benefit of methadone for treating refractory pain outweighs the risk of developing TdP. Chronic pain patients have a longer life expectancy, so there is a lower threshold to modify risk factors that increase the QTc interval. However chronic PPC patient populations are more similar than those in studies that included both chronic pain and MMT patients. This improves the external validity of our findings when assessing which QTc prolongation risk factors are most clinically significant to chronic PPC patients.
Conclusions
Predictors of QTc prolongation in our multivariate conditional logistic regression model of this PPC patient cohort included CHF, PUD, hypokalemia, rheumatologic disorders, concurrent use of medications with a known TdP risk, malignancy, hypocalcemia, and ME doses >45 mg per day. PPC patients with these risk factors are at increased risk of developing a prolonged QTc interval while taking methadone. Clinicians caring for these patients should minimize exposure to the identified risk factors and correct modifiable risk factors when clinically feasible. Additional population-based studies are needed in larger, more diverse PPC patient cohorts to support these findings.
Footnotes
Acknowledgments
The authors thank Elizabeth Dodds-Ashley, PharmD, Angelo Pedulla, MD, and Nicholas Venci, MD for their assistance with this study.
Author Disclosure Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors declare no competing financial interests exist. This article was presented as part of The Great Eight-Best Paper Presentations at the ACCP 2015 Global Conference on Clinical Pharmacy in San Francisco, CA on October 19, 2015.