
Abstract
Background
P
Definition
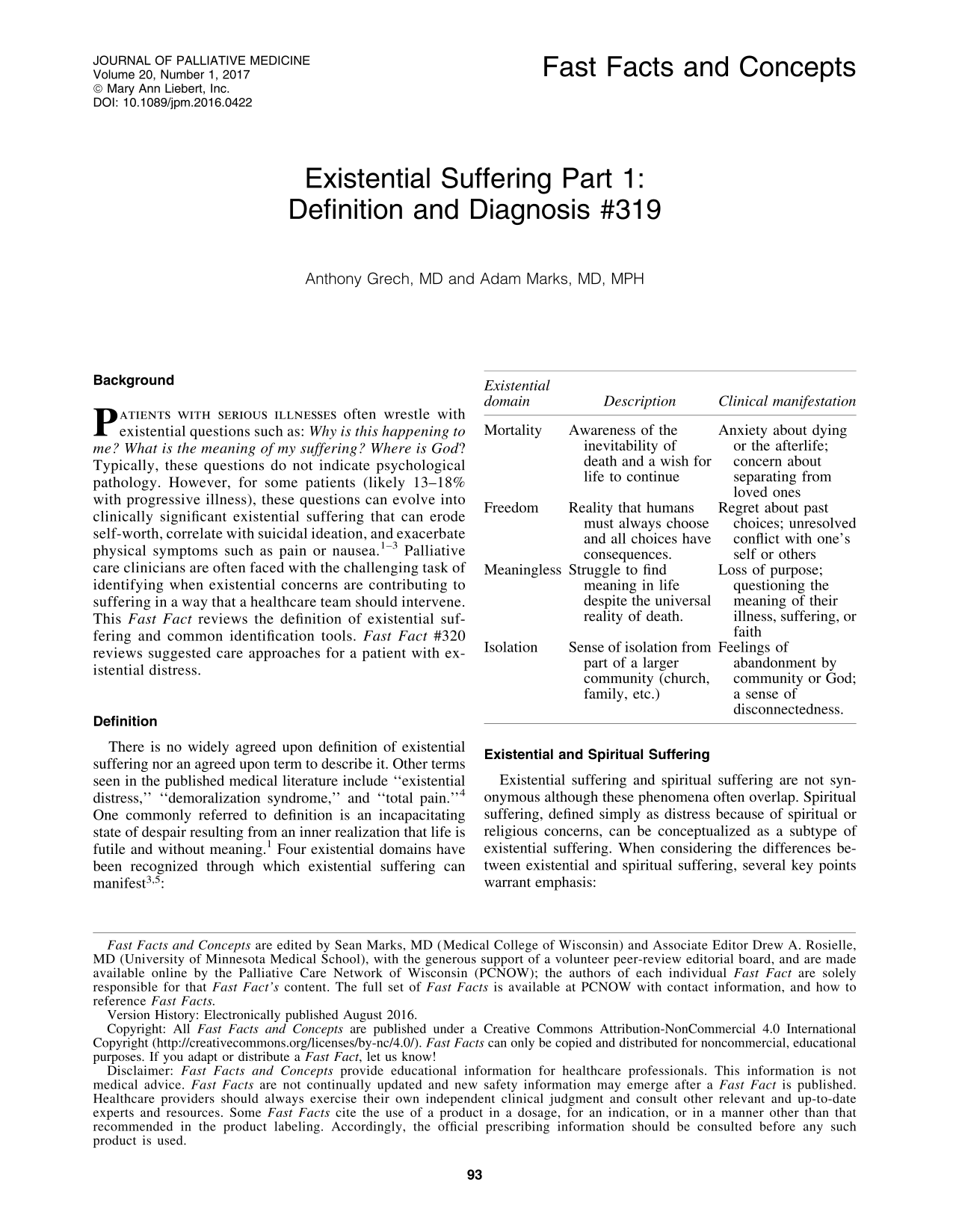
There is no widely agreed upon definition of existential suffering nor an agreed upon term to describe it. Other terms seen in the published medical literature include “existential distress,” “demoralization syndrome,” and “total pain.” 4 One commonly referred to definition is an incapacitating state of despair resulting from an inner realization that life is futile and without meaning. 1 Four existential domains have been recognized through which existential suffering can manifest3,5:
Existential and Spiritual Suffering
Existential suffering and spiritual suffering are not synonymous although these phenomena often overlap. Spiritual suffering, defined simply as distress because of spiritual or religious concerns, can be conceptualized as a subtype of existential suffering. When considering the differences between existential and spiritual suffering, several key points warrant emphasis:
• Some patients with existential suffering may not consider themselves to be spiritual and may become upset if a clinician reflexively consults a chaplain. • Spirituality has vastly different meanings for different individuals. See Fast Facts #19 and 274. In its broadest definition, spirituality can include involvement in a secular club or organization.
6
• Spirituality is part of each existential domain; however, it does not encompass all facets of each existential domain. Therefore, all spiritual suffering is existential suffering, but not all existential suffering is spiritual suffering. • “Spiritual” and “existential suffering” are not terms patients/families are typically familiar or comfortable with. At the bedside, it is best to name the distress explicitly or reflect the patient's language characterizing the suffering. For example, It sounds like you are trying to make sense of how this could happen. Or you said you've felt very apart from your family and faith community since this began. Can you tell me more about that?
Clinical Assessment Tools
Clinicians should listen for existential “cues” in all patients with serious illness, especially when symptoms seem out of proportion to their disease. Such cues can be expressions of doubt about life's meaning or one's faith or expressed feelings of isolation—for example, no one understands what I'm going through. Although there are multiple validated assessment tools available to aid healthcare providers in the diagnosis of existential suffering, many of these tools focus on one specific existential domain and others may be too cumbersome to implement into clinical practice. Instead one particularly useful tool involves simply asking the patient: Are you at peace? 7 A no answer should prompt further exploration of signs of distress, physical or otherwise, with follow-up questions such as What's keeping you from being at peace? or What worries you the most about your illness?
Risk Factors
No associations were found with existential suffering and time since diagnosis, stage of disease, or type of treatment.
1
One systematic review identified the following risk factors
8
:
• Poor social support: single patients (including divorced, separated, and widowed) or unemployed. • Poorly controlled physical or psychological symptoms. • Self-blame coping factors for illness and low sense of controllability of the illness. • Low level of physical activity.
Diagnostic Challenges
A lack of a universally accepted definition, clinician knowledge deficit, and concomitant psychological, spiritual, or social concerns make existential suffering difficult to diagnose. Furthermore, patients may have difficulty articulating their distress or may not be willing to disclose it if they feel their clinicians are too busy or guarded from discussing existential concerns. 4 Not all patients with existential suffering develop clinical anxiety or depression. In general, clinical depression can be defined by a loss of interest or pleasure in the present moment, whereas existential suffering is typically defined by a loss of hope, meaning, and anticipatory pleasure.9,10 Despite these challenges, it is important for clinicians who care for seriously ill patients to elicit existential concerns, as doing so can open opportunities for empathetic connection and clarify treatment options. Collaborating with social workers, chaplains, or psychologists is vital to better understand a patient's suffering.