
Abstract
Abstract
Background:
Dyspnea is highly prevalent in patients with idiopathic interstitial pneumonias (IIPs).
Objective:
The objective of this study is to examine the effectiveness and safety of continuous subcutaneous morphine for dyspnea in terminally ill IIP patients.
Setting/Subjects:
We retrospectively reviewed cases of terminally ill IIP patients who received continuous subcutaneous morphine for dyspnea.
Measurements:
We reviewed dyspnea severity measured using numerical rating scale (NRS) and respiratory rate (RR) before and two and four hours after morphine initiation. We conducted subgroup analyses of patients with and without noninvasive positive pressure ventilation (NPPV).
Results:
Twenty-five patients were included in this study. Median morphine dose at morphine initiation and two and four hours after treatment was 0.25, 0.25, and 0.5 mg/hour, respectively. Dyspnea NRS decreased significantly four hours after (mean ± standard deviation: 5.32 ± 2.58, p = 0.04) but not two hours (5.52 ± 2.43, p = 0.11) after morphine initiation compared with baseline (7.08 ± 2.33). RR did not change significantly either two or four hours after treatment compared with baseline. The median survival after morphine initiation was 47 hours. Patients who were not using NPPV showed significantly improved dyspnea both two and four hours after treatment compared with baseline, although patients who used NPPV showed no significant improvement with morphine. RR did not significantly change in either subgroup.
Conclusions:
Morphine might improve dyspnea in terminally ill IIP patients without decrease in RR.
Introduction
I
There are few studies examining the effectiveness and safety of morphine for dyspnea in terminally ill IIP patients.16–18 The aim of this study is to examine the effectiveness and safety of continuous subcutaneous morphine for dyspnea in terminally ill IIP patients.
Methods
Subjects
This retrospective study included terminally ill IIP patients who received continuous subcutaneous morphine for dyspnea between September 2010 and March 2013 in the National Hospital Organization (NHO), Kinki-Chuo Chest Medical Center, Japan. Patients were eligible if they had IIPs diagnosed based on IIP criteria, 1 had a dyspnea intensity ≥3 on a numerical rating scale (NRS) (before treatment, 0 = no dyspnea to 10 = worst possible dyspnea), were referred to a palliative care team, and received a continuous subcutaneous morphine for dyspnea. Patients were not eligible if they could not rate dyspnea on the NRS before treatment, if they could not rate dyspnea NRS at two and four hours after morphine initiation, or were treated with invasive positive pressure ventilation. Two respiratory specialists (Y.M. and Y.I.) and one radiologist (M.A.) who specializes in interstitial lung diseases rereviewed and classified the IIP patients as IPF or non-IPF using the criteria of the official guidelines of IPF. 3
Outcome measures
Medical records were retrospectively examined to gather demographic and clinical data. We reviewed dyspnea severity measured using NRS and respiratory rate (RR) before and two and four hours after morphine initiation to minimize the effect of disease progression or other intervention. There is a consensus that NRS is an appropriate measure of chronic breathlessness intensity. 19 The starting dose of morphine and the doses at two and four hours after morphine initiation were also reviewed. We examined survival after morphine initiation. We also analyzed patient subgroups with and without noninvasive positive pressure ventilation (NPPV) at morphine initiation and patients with and without acute exacerbation to determine changes in dyspnea NRS and RR.
Statistical analysis
We used data for two hours after treatment initiation to replace any missing NRS data at four hours using the last observation carried forward method if the patient was still alive but could not report dyspnea NRS (caused by sleep or decreased consciousness). We also conducted a complete case analysis as a sensitivity analysis. Changes in dyspnea NRS were tested using a repeated measure analysis of variance with post hoc test (Tukey honestly significant difference). Changes in RR were compared in a similar manner. Significance was assumed at p < 0.05.
This study was approved by the Institutional Review Board of the NHO, Kinki-Chuo Chest Medical Center (approval number 423).
Results
Patient characteristics
We identified 40 terminally ill IIP patients who had received continuous subcutaneous morphine for dyspnea. Fifteen patients were excluded (see Fig. 1). Almost 70% of patients had IPF. Sixty percent of patients had acute exacerbation based on the criteria for acute exacerbation of IPF in Japan. 20 No patients received anxiolytics and only two patients received hypnotics (see Table 1).

Study flow chart. IIPs, idiopathic interstitial pneumonias; NRS, numerical rating scale; RR, respiratory rate.
Data are presented as median (interquartile range) or n (%).
Measured within six months before morphine initiation.
Measured within 18 months before morphine initiation.
Measured within three months before morphine initiation.
Prescribed within six months before morphine initiation.
Prescribed within six hours before and after morphine initiation.
BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; IIPs, idiopathic interstitial pneumonia; IPF, idiopathic pulmonary fibrosis; KL-6, Krebs von den Lungen-6; LDH, lactate dehydrogenase; NPPV, noninvasive positive pressure ventilation; NSIP, nonspecific interstitial pneumonia; PaCO2, partial pressure of carbon dioxide in arterial blood; VC, vital capacity.
Oxygen delivery devices or mechanical ventilation
Forty percent of patients used NPPV. More patients with acute exacerbation used NPPV than patients without acute exacerbation (see Table 1). All patients used same oxygen delivery devices or mechanical ventilation within four hours after morphine initiation. In only two patients, oxygen flow rate was increased at two or four hours after morphine initiation compared with baseline. In the remaining 23 patients, oxygen flow rate or fraction of inspired oxygen was not changed or decreased.
Dose of morphine
The median doses of morphine at initiation and two and four hours after treatment were 0.25 mg/hour (interquartile range [IQR]: 0.25–0.25), 0.25 mg/hour (0.25–0.5), and 0.5 mg/hour (0.25–0.75), respectively.
Survival
The median survival after morphine initiation was 47 hours (IQR: 26–133 hours). Four patients died within 24 hours of beginning treatment.
Dyspnea NRS change
Changes in dyspnea NRS were available in all patients at two hours but were not available in four patients at four hours after morphine initiation because of sleep (n = 2) and no assessment (n = 2). Compared with baseline (mean ± standard deviation [SD]: 7.08 ± 2.33), NRS for intensity of dyspnea significantly decreased after four hours (5.32 ± 2.58, p = 0.04), but not after two hours of treatment (5.52 ± 2.43, p = 0.11) (see Fig. 2). In addition, the decrease of dyspnea NRS was more than 1, which is a clinically important difference in the intensity of dyspnea. 19 The complete case analysis also showed that dyspnea NRS decreased significantly after four hours of treatment compared with baseline (data not shown).
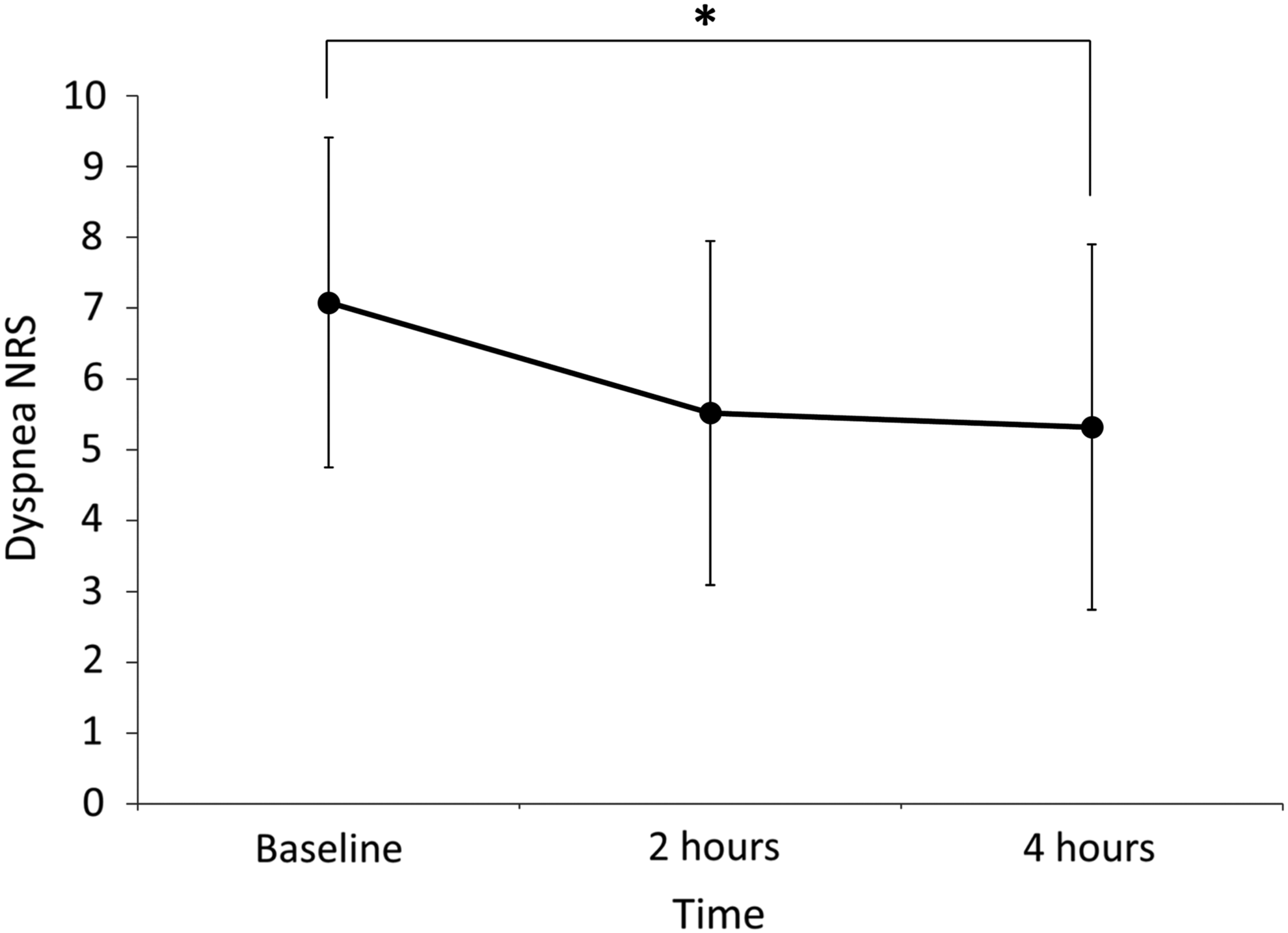
Dyspnea NRS at baseline and two and four hours after morphine initiation. *p = 0.04.
RR change
RR did not change significantly throughout the study (baseline 34.16 ± 7.08; two hours 32.72 ± 7.39, p = 0.35; four hours 33.64 ± 6.93, p = 0.69).
Subgroup analysis of patients with and without NPPV
We observed no significant improvement of dyspnea in the subgroup of patients on NPPV at either two or four hours after treatment compared with baseline (data not shown). In contrast, patients in the subgroup who were not on NPPV showed significantly decreased dyspnea NRS at both two hours (mean ± SD: 4.87 ± 2.62, p = 0.034) and four hours (4.93 ± 2.69, p = 0.042) after treatment compared with baseline (6.80 ± 2.60). RR did not change significantly in either subgroup (data not shown).
Subgroup analysis of patients with and without acute exacerbation
We observed no significant improvement in dyspnea in patients with acute exacerbation either at two or four hours after treatment compared with baseline (see Fig 3A). In contrast, patients in the subgroup without acute exacerbation showed significant improvement of dyspnea at both two hours (mean ± SD: 4.70 ± 2.31, p = 0.007) and four hours (4.10 ± 2.73, p = 0.002) after treatment compared with baseline (7.40 ± 3.03) (see Fig. 3B). RR did not change significantly in either subgroup (data not shown).
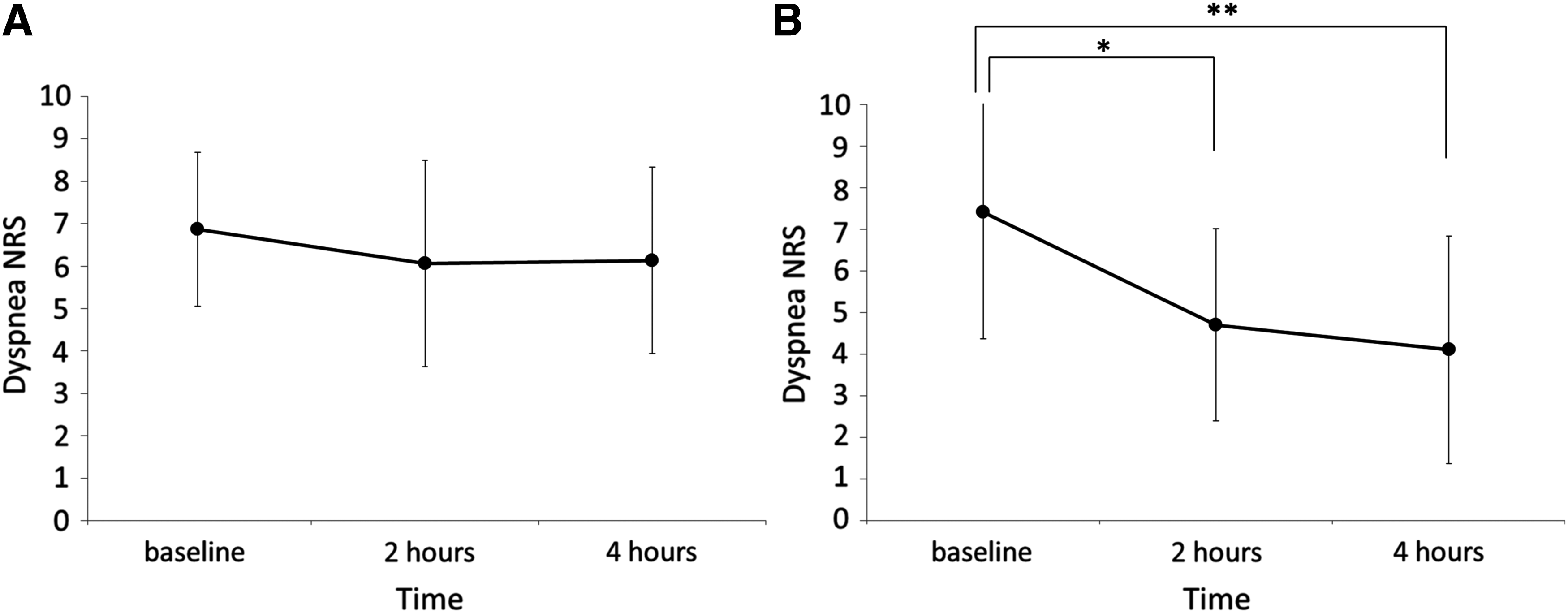
Subgroup analysis of dyspnea NRS change in patients with and without acute exacerbation.
Discussion
We have shown that continuous subcutaneous injection of morphine significantly decreased NRS for dyspnea after four hours of treatment compared with baseline in terminally ill IIP patients without decrease in RR.
Allen et al. reported that diamorphone was effective for relieving dyspnea in 11 terminally ill inpatients with IPF. 16 In their study, mean survival after starting morphine was five weeks. Although our patients were much more vulnerable (median survival was 47 hours), a continuous subcutaneous infusion of morphine was safe and effective in relieving dyspnea.
Recently, Takeyasu et al. reported that continuous morphine infusion was effective for improving dyspnea in 22 terminally ill interstitial pneumonia patients with acute exacerbation. 17 In their retrospective study, they used the operational definition of dyspnea relief within 24 hours based on chart descriptions of patients’ expression and/or physicians’ or nursing records with observations. Therefore, dyspnea severity before and after treatment was not shown. We used dyspnea NRS, a standard measurement tool for dyspnea, to assess dyspnea at specific time points (two and four hours after treatment and at baseline). Our present study indicates the short-term effect of continuous subcutaneous morphine on dyspnea in terminally ill IIP patients.
Even low-dose morphine significantly decreased dyspnea NRS remained in the moderate range in our study, suggesting that higher but appropriate dose of morphine could alleviate dyspnea NRS into the mild range.
Morphine did not decrease dyspnea NRS in patients using NPPV, although dyspnea decreased in patients who were not using NPPV. According to Nava et al., NPPV is effective in reducing dyspnea in cancer patients, 21 the dyspnea-modifying effects of morphine may partially compete with that of NPPV.
Morphine decreased dyspnea NRS in patients without acute exacerbation. Takeyasu et al. reported that morphine was effective in interstitial pneumonia patients with acute exacerbation. 17 In this study, morphine was also effective in patients without acute exacerbation. However, contrary to the results of Takeyasu's study, 17 morphine did not decrease dyspnea NRS in patients with acute exacerbation in our study. More patients used NPPV in the acute exacerbation subgroup (53.3%) than in the nonacute exacerbation subgroup (20%), which may have influenced our results.
In this study, morphine did not decrease RR at two and four hours after treatment compared with baseline. The results were same even in patients who did not use NPPV. Therefore, morphine is likely to be safe within the dose we used in this study.
This study has some limitations. First, the study was retrospective. Second, interventions other than morphine were conducted simultaneously, such as oxygen therapy, NPPV, and pharmacotherapy. Third, we did not obtain certain information about IIPs at the onset of morphine initiation, including PaO2, PaCO2, and lung function. Vital capacity was measured within 18 months before morphine initiation, thus actual vital capacity would have been worse at the time of morphine treatment. Fourth, the patients in this study had acute change in dyspnea, which was assessed by NRS identified as a valid tool for chronic dyspnea. Finally, we cannot generalize our findings to all IIP patients with dyspnea because our patients were terminally ill IIP patients with severe dyspnea and high RR.
In conclusion, morphine might improve dyspnea in terminally ill IIP patients without a decrease in RR. A prospective study is warranted in the future.
Footnotes
Acknowledgments
We are grateful for the cooperation of members of the palliative care team in the National Hospital Organization, Kinki-Chuo Chest Medical Center.
Author Disclosure Statement
No conflicting financial interests exist.