
Abstract
Abstract
Objectives:
Prognostic challenges hinder the identification of patients with advanced chronic obstructive pulmonary disease (COPD) for timely palliative interventions. We postulate that a two-minute derivative (two-minute walking distance [2MWD]) of a standard six-minute walk test (6MWT) can identify frail subjects with poorer survival for early palliative intervention. The primary outcome of interest is mortality at 18 months. Secondary objectives include evaluation of the relationship between the 2MWD and ability to self-care, dyspnea-related disabilities, nutrition, forced expiratory volume in first second (FEV1), quality of life (QoL), and comorbidity burden.
Design and Setting:
One hundred twenty-four subjects with stage 3 and 4 COPD were recruited and followed up. Ability to self-care, dyspnea-related disabilities, airflow limitation, nutrition, and QoL were measured by using modified Barthel index (MBI), Modified Medical Research Council (MMRC) dyspnea scale, FEV1 (% predicted), BODE [BMI(B), FEV1(O), MMRC(D), 6MWT(E)] index, updated ADO [Age(A), MMRC(D), FEV1(O)] index, Subjective Global Assessment (SGA), and St. George's Respiratory Questionnaire (SGRQ), respectively. Survival data were prospectively collected and analyzed.
Results:
The 2MWD correlates highly with BODE and predicts updated ADO independent of age, co-morbidities, long-term oxygen therapy (LTOT), body mass index, and FEV1. Log-rank test performed with Kaplan–Meier plots demonstrates that 2MWD ≤80 m significantly predicts survival time (p < 0.05). Cox proportional hazard regression shows a 3.6-time greater probability of 18-month mortality (hazard ratio [HR] 3.57; 95% confidence interval [CI] 1.26–10.13; p < 0.05). In addition, 2MWD strongly predicted MBI and MMRC, independent of age, co-morbidities, LTOT, body mass index, and FEV1. Subjects with 2MWD ≤80 m have a poorer ability to self-care (median MBI 90 vs. 100), lower FEV1 (32.9% ± 9.8% vs. 38.1% ± 9.4%), poorer QoL (mean SGRQ 46.6 ± 16.2 vs. 36.6 ± 13.3), and greater dyspnea-related disability (mean MMRC 1.7 ± 0.7 vs. 0.9 ± 0.6), and they are more malnourished (40.4% vs. 9.7%; RR 1.51) (all p < 0.001).
Conclusion:
2MWD ≤80 m identifies subjects with higher mortality, greater functional dependence, poorer in nutrition, greater dyspnea, and lower QoL. Incorporation of 2MWD into composite prognostic indices can enhance predictive accuracy and identify patients requiring early proactive palliative interventions.
Background
P
The six-minute walk test (6MWT) is a widely validated and reliable tool that is frequently performed in respiratory clinics to assess functional exercise capacity.7,8 It is designed as a sub-maximal, self-paced physical performance measure, and it was previously demonstrated to predict medium-to-long-term mortality in COPD.9,10 A recent study evaluating one-year mortality in 1218 subjects with stable COPD reported that the earliest and strongest predictors of death were an interval decline in 6MWT distance, lending support to its utility as a prognostic indicator for short-term mortality. 11
However, clinical observations suggest that a subpopulation of patients with advanced COPD exhibits poorer exercise tolerance shortly after test initiation. Between 40% and 70% of subjects with advanced COPD would experience exercise-induced desaturation (EID) beyond 88% within shortly after test initiation.12–14 We postulate that walking distances within the first few minutes of a 6MWT better reflects submaximal exercise capacity in advanced COPD. We hypothesize that a two-minute derivative of a standard 6MWT—two-minute walking distance (2MWD) can predict short-term survival in patients with advanced COPD. To the best of our knowledge, this is the only study that reports the prognostic utility of the 2MWD. The primary outcome of interest is mortality at 6, 12, and 18 months. Secondary objectives include evaluating the association of 2MWD with cross-sectional measurements of the ability to self-care, dyspnea, nutrition, airflow limitation, QoL, and comorbidity burden at the point of recruitment.
Methods
We report the results of an observational study with prospective collection of survival data. The study was approved by the institutional research ethics committee.
Patient population
Clinically stable subjects attending respiratory outpatient clinics and satisfying the following criteria were recruited: (1) ≥21 years old; (2) diagnosis of COPD; (3) ratio of forced expiratory volume in first second (FEV1) to forced vital capacity of <70%; and (4) Global initiative for Chronic Obstructive Lung Disease (GOLD) classification for stage 3 and 4 COPD. 15 Exclusion criteria were (1) coexisting active pulmonary tuberculosis, pulmonary fibrosis, pneumothorax, or lung cancer; (2) diagnosis of asthma; (3) too physically ill or mentally incapacitated to participate; (4) active microbial infections; and (5) hospitalization for acute COPD exacerbations within the recent two weeks. Witnessed and informed consent was obtained.
Measurements
Cross-sectional data were collected at the point of subject recruitment and include sociodemographic data, smoking status, exacerbation frequency, and long-term oxygen therapy (LTOT). Airflow obstruction was measured as the percentage-predicted FEV1 by using a portable spirometer. The Modified Medical Research Council (MMRC) scale was used to quantify breathlessness-induced disability.
Prognostic severity was scored by using the BODE [BMI(B), FEV1(O), MMRC(D), 6MWT(E)] index16,17 and the updated-ADO [Age(A), MMRC(D), FEV1(O)] index.18,19 Both are multicomponent prognostic indices that were validated in COPD to predict survival, and which also predict other patient-related outcomes, including health status and functional capacity. The BODE index incorporates the body mass index (B), airflow obstruction as FEV1(O), MMRC(D), and the 6MWT(E). 20 It has four prognostic categories corresponding to increasing four-year mortality: 0–2 points (80%), 3–4 points (67%), 5–6 points (57%), and ≥7 points (18%). The ADO index combines age(A), MMRC(D), and the FEV1(O). It was recently updated and validated in 1350 subjects with COPD and was found to better predict three-year mortality over FEV1 alone.
Physical co-morbidity was measured by using the age-adjusted Charlson comorbidity index (CCI). 21 Ability to self-care was assessed with the modified Barthel index (MBI), which evaluates 10 activities of daily living (ADLs), each with 5 levels of dependency. 22 Its maximum score is 100 points, representing full independence in all ADLs. Subjects were rated on their nutritional status by using the Subjective Global Assessment (SGA) tool. 23 The St. George's Respiratory Questionnaire (SGRQ) measured disease-specific QoL across three domains (symptoms, activity, impact), with higher scores denoting poorer QoL.24,25
The walking tests were conducted by referencing the American Thoracic Society (ATS) guidelines published in 2002. 26 Subjects were instructed to walk along a level corridor at their own pace while attempting to cover as much distance as possible during the allocated time. The time elapsed was called out every two minutes, and standard encouragement was provided at 30-second intervals. Pulse oximeter readings and the distance traveled were recorded at the start, second, fourth, and sixth minute. The 2MWD was recorded as the total distance traversed by the end of the second minute of walking. It is a direct derivative of the standard 6MWT. The test would be stopped if the subject presents with symptoms necessitating termination as per ATS protocol, if they verbalize overt fatigue or dyspnea and cannot continue despite verbal persuasions, or if they develop EID to ≤90%. Supplemental oxygen was not augmented in event of desaturation. Subjects were prospectively followed up for all-cause mortality. Survival time was measured in days from enrolment until death or censoring at the end of the follow-up period.
Statistical analysis
Data analyses were performed by using IBM SPSS Statistics v21. Receiver operator characteristics (ROC) curves were constructed for 2MWD, BODE, and the updated-ADO index. Area under curves (AUC) for these indices were derived and compared. Using ROC analyses, an optimal cut-off for 2MWD was identified and used as a reference point to maximize the percentage of patients correctly classified for 18-month mortality. Kaplan–Meier survival plots were then used to compare survival probabilities between the two groups. Statistical significance was determined by the log-rank test. Univariate and multivariate Cox proportional-hazards analyses were then applied to all three indices, as well as a range of other single-item prognostic variables to evaluate their capacity to predict 18-month mortality.
Pearson's correlation was used to examine the relationship between 2MWD and variables, including the BODE, updated-ADO, MBI, MMRC, SGA, and SGRQ. Standard multiple linear regression analyses were performed to determine predictors of these variables. Clinically important and predetermined covariates were entered as independent variables. These included age, age-adjusted CCI, use of domiciliary oxygen, FEV1, and BMI. Using the 2MWD cut-off established through ROC analysis, an independent-samples t-test was applied to test each group for their associations with parametric continuous and ordinal measures. Nonparametric associations were assessed by using Mann–Whitney U tests. The chi-squared test was applied to categorical variables. For all analyses, two-sided p-values of less than 0.05 were taken to indicate statistical significance.
Results
One hundred twenty-four subjects who were recruited had a mean ± SD age of 71.7 ± 7.6 years. The majority were Chinese men. Eighty-five (68.5%) subjects had stage 3 and 39 (31.5%) subjects had stage 4 COPD. Mean FEV1 was 35.9% ± 9.8%. Twenty-four (19.4%) subjects required home oxygen. Sixty-nine (55.6%) subjects had recurrent hospitalizations for exacerbations in the preceding year, whereas 11 (8.9%) had previous ICU admissions. The mean 2MWD was 81.9 ± 27.3 m, whereas the mean 6MWT was 167.2 ± 109.6 m.
Using ROC analysis based on 18-month mortality, a 2MWD of 80 m was identified as the ideal prognostic reference point (AUC = 0.70, p < 0.01). Incidentally, this approximates the 40th percentile of the study population. The study cohort was stratified at a 2MWD of 80 m. Baseline characteristics of the two groups are compared and presented in Table 1. Acronyms are referenced in the legend of Table 1.
FEV1, forced expiratory volume in first second; LTOT, long-term oxygen therapy; CPR, cardiopulmonary resuscitation; BMI, body mass index; SGA, Subjective Global Assessment (grade A: no or mild undernourishment; grade B: moderate undernourishment; grade C: severe undernourishment); 6MWT, six-minute walk test distance; 2MWD, two-minute walking distance derived from the 6MWT; MMRC, Modified Medical Research Council; BODE index, BMI(B), FEV1(O), MMRC(D), 6MWT(E); updated-ADO Index, Age(A), MMRC(D), FEV1(O); MBI, modified Barthel index; CCI, Charlson comorbidity index; SGRQ, St. George's Respiratory Questionnaire.
Fifty-six (45.2%) subjects were incapable of completing the full six minutes of walking owing to dyspnea or fatigue, despite verbal encouragement and/or significant EID ≤90%. Forty-eight (38.7%) experienced desaturations to ≤90% by the end of two minutes. Mean SpO2 levels fell from 95.9% at the start, to 88.8% at the end of two minutes. As oximeter readings were monitored at stipulated intervals, the SpO2 level fell to as low as 76% before termination. Our findings are consistent with clinical observations that a subpopulation of patients exhibits very poor tolerance shortly after test initiation.
Patients were prospectively followed from enrolment for a median (range) of 819 days (43–1124). All subjects were followed up for at least 18 months. Overall, 17 out of 124 (13.7%) patients died within 18 months from the time of the recruitment, whereas 34 out of 124 (27.4%) died over the entire follow-up period at an average (range) of 543 days (43–1100) from enrolment.
We compared the 2MWD with two well-validated composite prognostic indices: 2MWD strongly correlated with BODE (r = −0.631, p < 0.001), and it has moderate correlation with the updated ADO (r = −0.521, p < 0.001). Standard multiple regression analysis demonstrated that the 2MWD strongly predicted ADO scores independent of FEV1, age, age-adjusted CCI, BMI, and LTOT (R2 = 0.892; β = −0.175, p < 0.005). In addition, 2MWD ≤80 m was inversely related to the four prognostic sub-categories of the BODE index (p < 0.001). Subjects with 2MWD ≤80 m were 2.4 times more likely to score ≥7 points on the BODE index (73.1.1% vs. 36.1%; RR 2.37; p < 0.001), corresponding to 18% survival at four years.
ROC analysis was performed for all three variables to assess their predictive capacity for 18-month mortality. The AUC for the 2MWD (AUC 0.70; 95% confidence interval [CI] 0.55–0.85; p < 0.01), updated ADO (AUC 0.685; 95% CI 0.55–0.82; p < 0.05), and BODE index (AUC 0.719; 95% CI 0.58–0.86; p < 0.005) were very similar. Subjects with 2MWD ≤80 m had poorer mean survival time. Log-rank test performed with the Kaplan–Meier plots confirms a significant difference in survival probabilities (p < 0.005) (Fig. 1).
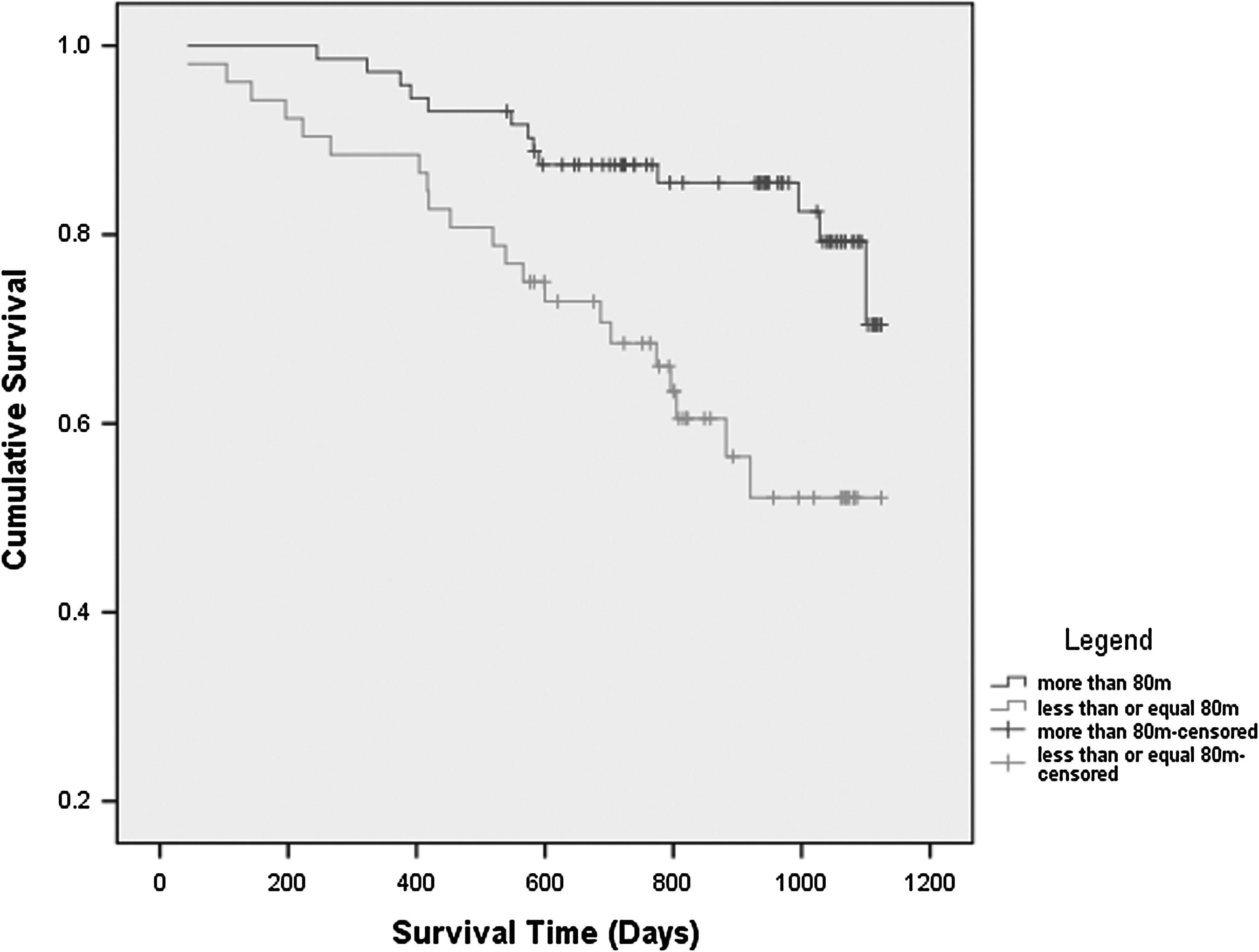
Kaplan–Meier survival analysis showing cumulative survival.
Univariate Cox proportional hazard regression demonstrates that the 2MWD ≤80 m carries a high probability of death at 18 months (hazard ratio [HR] 3.57; 95% CI 1.26–10.13; p < 0.05). This closely approximates the poorest quartile of the updated-ADO index (score ≥9: HR 3.70; 95% CI 1.43–9.6; p < 0.01). In comparison, other disease-specific prognostic markers, including the worst prognostic category of BODE (score ≥7: HR 2.21; 95% CI 1.09–4.50; p < 0.05), LTOT (HR 2.21; 95% CI 1.07–5.57; p < 0.05), and MMRC (HR 1.74; 95% CI 1.10–2.74; p < 0.05), were associated with lower probabilities of death (Table 2). After adjusting for age, gender, smoking status, and LTOT, 2MWD ≤80 m remains an independent predictor of mortality (HR 3.21; 95% CI 1.05–9.85; p < 0.05).
ADO ≥9 points denotes the poorest quartiles of the study population corresponding to ≥14.5% risk of three-year mortality.
BODE score ≥7 points denotes the worse prognostic subcategory corresponding to 18% survival at four years.
6MWT <150 m carries the worse score under the 6MWT category of the BODE index.
In addition, 2MWD strongly correlated with the MMRC, and moderately with MBI, FEV1, and SGRQ. Compared with the 6MWT from which it is derived, the 2MWD had a far stronger correlation with the MBI (r = 0.581 vs. 0.362; p < 0.001). The strengths of its other correlations were comparable, if not, slightly exceeding those of the 6MWT (Table 3). Standard multiple regression analyses demonstrate that the 2MWD is an independent predictor of both the MBI (R2 = 0.450; β = 0.313; p < 0.01) and the MMRC (R2 = 0.508; β = −0.384; p < 0.001), after adjusting for age, age-adjusted CCI, use of domiciliary oxygen, BMI, and FEV1. The 2MWD made the strongest unique contribution to both models. In comparison, the 6MWT was not predictive of MBI scores. Using similar co-variates, 2MWD and 6MWT distances could not predict SGRQ and CCI.
Subjects with a 2MWD ≤80 m were also found to have (1) poorer ability to self-care (median MBI 90, IQR 81–95 vs. 100, IQR 95–100), (2) greater airflow limitation (mean FEV1 32.9% ± 9.8% vs. 38.1% ± 9.4%), (3) greater dyspnea-related disability (mean MMRC 1.7 ± 0.7 vs. 0.9 ± 0.6), and (4) poorer QoL (mean SGRQ 46.6 ± 16.2 vs. 36.6 ± 13.3). These comparisons were all statistically significant at p < 0.001. A difference in median MBI scores by 10 points between the two groups translates to at least a 25% greater level of physical dependency for 4 out of 10 ADLs. Further analyses show that subjects with 2MWD ≤80 m were 2.3 times more likely to score ≥3 points on the MMRC (63.5% vs. 16.7%; RR 2.28; p < 0.001), corresponding to severe dyspnea within 100 yards of a leisurely walk. In addition, these subjects were 1.5 times more likely to be rated SGA grade B or C, corresponding to moderate or severe undernourishment, respectively (40.4% vs. 9.7%; RR 1.51; p < 0.001).
Discussion
Both the ATS recommendations and the GOLD statement have called for increased provision of palliative care to patients living with COPD. But there is little guidance regarding their identification.27,28 This is likely due to the paucity of evidence informing accurate prognostication for short-term survival. Studies have examined one to two year post-discharge mortality in hospitalized patients and found age, COPD severity, ICU admissions, and the use of maintenance glucocorticosteroids as predictors of poor outcome.29–32 However, the identification of patients for early palliative care should begin when patients are clinically stable, rather than during episodes of life-threatening exacerbations. An ideal assessment tool to serve this purpose would be one that can be safely and conveniently performed in ambulatory clinics, provide reliable prognostic information, and discern frailer patients with greater multidimensional care needs.
The 2MWD is safe, rapid, and inexpensive. It strongly predicts short-term survival in patients with advanced COPD. Using a cut-off at 80 m, subjects were found to have a 3.6-time greater probability of dying within 18 months (p < 0.05). This risk remains significant even after adjusting for age, gender, smoking status, and LTOT.
Moreover, the 2MWD effectively stratifies patients beyond traditional single-item and multidimensional models of risk. Composite prognostic indices such as BODE, ADO, and DOSE have been shown to significantly predict three to five year mortality.16,18,33 More recently, an updated 15-point ADO index with good discriminant ability was validated in 10 European and American populations and predicts three-year mortality. 19 In our study, not only did the 2MWD correlate strongly with BODE, but it also predicts the updated ADO independent of age, comorbidities, FEV1, BMI, and LTOT. Contrary to previous studies that consistently reported that composite measures outperform their component variables, including the FEV1, our study finds that the ROC curve areas for the 2MWD are noninferior when compared against that of BODE and the updated ADO. Furthermore, we demonstrated that a single measurement of 2MWD (with a cut-off equivalent to the 40th percentile) carries a likelihood of early deaths comparable to the poorest quartile of the updated-ADO scores, and, in fact, exceeded that of the worst prognostic category under the BODE index.17,34 Among the single-item prognostic variables investigated in our study, only two other variables were significant in our analyses (MMRC ≥3, and the use of LTOT), both of which were associated with a lower risk of deaths. We postulate that the addition of 2MWD to composite risk models will greatly enhance model performance, and it will translate into a more accurate prediction of short-term mortality.
Prognoses should not be the sole determinant of referrals to palliative services, although it is currently heavily relied on when deliberating palliative resource allocation. Difficulties in prognostication may lead to serious neglect of the multifaceted needs of dying patients, as their terminal phase of illness goes unrecognized. 35 There is mounting evidence that COPD is an persistent inflammatory disorder with widespread systemic complications, including cardiovascular compromise, frailty, and sarcopenia.36–38 Greater emphasis will have to be placed on screening a patient's global well-being when determining his or her palliative care needs, including evaluating domains of symptom burden, functional capacity, exercise endurance, nutrition, and QoL, which can be improved through integrated palliative interventions.39,40 Such an approach will create greater access to palliative care services for people living with COPD, rather than relying on a physician's clinical estimation of survival alone.
Our findings demonstrate that the 2MWD strongly predicts both the ability to self-care (MBI) and dyspnea-limited disabilities (MMRC). In comparison, the 6MWT had far poorer correlation and could not predict MBI scores. We speculate that the 2MWD better predicts MBI, because it more accurately reflects a subject's self-determined gait speed, which is known to correlate with a person's ability to self-care.41–43 The average gait speed derived over a longer duration of walking is far more likely to be influenced by multidimensional factors, including waning motivation and progressive fatigue in patients with poor pulmonary reserves. As ADLs are performed at submaximal levels of exertion, 2MWD will better reflect functional exercise capacity for daily activities, when compared against longer walking tests in advanced COPD. It is, therefore, unsurprising that the 2MWD has only modest correlation (r = 0.67) with the 6MWT, despite it being a direct derivative.
We further explored other markers of global well-being and found that subjects with 2MWD ≤80 m fell within the lowest 40th percentile for disease-specific QoL, despite similarly severe airflow obstruction. They were also 1.5 times more likely to be undernourished. These qualities strongly support the potential utility of the 2MWD in screening for clinically frail subjects with multidimensional needs, for palliative multidisciplinary interventions.
Our study encompasses a few unique strengths. First, this is the only study specifically focusing on the prognostic utility of the 2MWD. Second, we based our analysis on predicting the odds of dying at 18 months—a reasonable time frame for palliative consultations for end-stage organ failures. In comparison, the majority of previous works were based on models prognosticating three- to five-year survival. In addition, our study recommends a useful cut-off value, whereas other predictors without specific reference values may not inform clinical decision-making. Lastly, previous studies frequently focused solely on predicting survival. Comparatively, our study comprehensively examined a wide range of patient-centered health status and established that 2MWD reflects global well-being and captures many multisystemic effects of disease severity in COPD rather than pulmonary impairment alone. This makes it an ideal tool for identifying frailer patients with similarly advanced airway obstruction, for early and proactive multidisciplinary palliative interventions.
There are limitations to this study. The modest sample size of 124 subjects meant that results need confirmation in a larger sample. Challenges in recruitment largely stem from low motivation to participate in a lengthy but very comprehensive examination of physical, social, psychological, functional, and nutritional assessment, involving patients who are physiologically frail from a progressive and incurable disorder.
A second limitation involves protocol differences between the 2002 and 2014 ATS guidelines for the 6MWT. As our study commenced in early 2013, conduct of the 6MWT adhered to the 2002 guidelines that did not state an SpO2 threshold for terminating the test. Before 2014, most studies either did not report or reported using an SpO2 of 86%–90% as their safety cut-off.44–49 We chose a more conservative cut-off at 90% in line with institutional safety policies. Physiologically, an SaO2 value exceeding 90% corresponds to the plateau phase of the oxygen-hemoglobin dissociation curve. 50 Further falls in SaO2 trigger a precipitous drop in hemoglobin carriage of oxygen, which would have compromised safety in our subjects with poor pulmonary reserves. The updated 2014 protocol sets a safety SpO2 threshold at 80%. Although this standardization promotes homogeneity in test methodology, its lower threshold will inadvertently pose significant challenges to the comparison of studies initiated before and after 2014. More work will need to be done to establish prognostic cut-offs by using this revised guidelines, especially for longer time-based walking assessments (e.g., 6MWT or 12-minute walk tests) that will be the most affected by the changes.
Third, our study population, being composed predominantly of Chinese men, will limit the external validity of our results. Further calibration studies need to be performed to accommodate differences in stride length and gait speed due to gender and ethnicity. Finally, the 2MWD is performed as a subset of a longer 6MWT. It will be interesting to examine whether two-minute walk tests performed in isolation will yield similar predictive properties.
Conclusion
The 2MWD is a safe and easily derivable assessment that can be used in routine COPD office practices, to identify patients for early palliative care. A 2MWD ≤80 m strongly predicts 18-month survival and appears noninferior to BODE and the updated ADO in its prognostic value. In addition, we established a useful cut-off at 80 m, below which subjects are more likely to suffer greater functional dependence, poorer dyspnea-related physical performance, lower QoL, and higher rates of malnutrition. Incorporation of the 2MWD as part of a composite prognostic index will substantially enhance predictive accuracy for short-term survival, and it will identify subjects with multidimensional unmet needs for proactive and multidisciplinary palliative interventions.
Footnotes
Acknowledgments
This collaborative study is undertaken by the Department of Palliative Medicine and the Department of Respiratory and Critical Care Medicine in a tertiary, teaching hospital. All named co-authors participated in the design of the study, as well as in the drafting of the final article. The authors would like to take the opportunity to thank all respiratory physicians and personnel from the spirometry laboratory who were involved in the recruitment and assessment of the research participants. This research received funding from the NHG-KTPH Small Innovative Grant (SIG) and the Lien Center of Palliative Care Extramural Research Awards.
Author Disclosure Statement
The authors declare that there is no inherent conflict of interest.