
Abstract
Abstract
Background:
Limited comparative data are available on the symptom severity and burden of dialyzed versus nondialyzed end-stage renal disease (ESRD) patients and their association with negative emotional states.
Objective:
To investigate the prevalence of symptom burden and severity of ESRD patients and correlate the findings with their psychological status.
Methods:
This was a cross-sectional study of dialyzed (N = 87) and nondialyzed (N = 100) patients. The symptom burden and severity were determined using the Dialysis Symptom Index (DSI) and the psychological assessment using Depression Anxiety Stress Scale 21 (DASS-21).
Results:
Symptom severity evaluated using the DSI was comparable in both groups with fatigue as the most common symptom (n = 141, 75.4%), followed by sleep-related, sexual dysfunction, and dry skin problems. The symptom burden for worrying, dry skin and mouth, decreased appetite, numbness, and leg swelling were significant in not dialyzed group (p < 0.05).The DASS-21 scores revealed that 11% of patients were depressed, 21.8% were stressed, and 15.6% were anxious (p < 0.030). The prevalence of psychological disturbances was associated with high symptom burden regardless of their treatment options (p < 0.005). Dialyzed patients showed a positive psychological status trend on DASS-21 assessment. The not dialyzed group consisted of 34% from comprehensive conservative group, 26% of choice-restricted conservative care, and 40% with no definitive future plan.
Conclusions:
There was no difference in the prevalence of symptom burden and severity, irrespective of the type of treatment. Psychological disturbances were associated with higher symptom burden and severity and, therefore, should be screened thoroughly to achieve optimal ESRD management.
Introduction
T
The mainstay of treatment for ESRD patients is renal replacement therapy (RRT) that consists of hemodialysis (HD), peritoneal dialysis (PD), and kidney transplant. HD is the preferred RRT choice in many parts of the world; however, treatment modalities are linked to the resource availability and economic development of the country. 8 For example, continuous ambulatory peritoneal dialysis (CAPD) is widely used in Mexico, Thailand, and Hong Kong.9,10 Despite kidney transplant being the treatment of choice for ESRD, only Singapore recorded a high number of transplants (369 p.m.p.) in 2011, with much fewer numbers performed in other Southeast Asian countries. 7
Population-based studies have reported many limiting factors associated with intensive thrice-weekly HD treatment, including major physical and psychological problems, metabolic derangements, and financial limitations.9–11 ESRD is a chronic condition, which may result in various debilitating symptoms, like fatigue, pruritus, sleep-related problems, and sexual dysfunction.12,13 These distressing symptoms may be directly due to disease-related complications, treatment-related complications, or both. These symptoms are often underrecognized by patients and their physicians as the majority of patients present with clusters of symptoms rather than single symptoms. 14 Fatigue and pruritus are the most common symptoms among both nondialysis and dialysis patients and may improve with dialysis treatment. 15 The incidence of fatigue and pruritus was reported to be up to 71–74% and 46–64% of patients with advanced renal disease, respectively.12,13 Previous research demonstrated that the prevalence of psychological disturbances, such as depression and anxiety, was higher among ESRD patients (21–28%) than among the general adult population(6–7%) worldwide.16–20 Studies on chronic kidney disease (CKD) patients showed that depression was linked to an impaired quality of life (QoL) and possibly high morbidity and mortality.21–23 Factors such as psychosocial stress, symptom burden, and systemic impairment due to disease complications may influence the level of anxiety and depression in ESRD patients. In the contrary, reduced rates of depression and, hence, improved QoL and physical and psychosocial well-being were observed following successful renal transplants. 17
Studies on the prevalence of the symptom burden and the level of severity among ESRD patients, with or without RRT are lacking in Malaysia. Little is known about the psychological well-being of ESRD patients and its relationship with symptom burden, including physical symptoms, especially in nondialysis patients. Data concerning the circumstances related to patients' decisions not to start dialysis are sparse in the region of Southeast Asia. This study examined the physical symptom burden (prevalence and severity) among dialysis and nondialysis ESRD patients, its correlation with negative emotional states (depression, stress, and anxiety), and reasons underlying patients' decisions not to undergo dialysis.
Methods
Study design and setting
This study was a cross-sectional survey of ESRD patients who were on dialysis treatment or not dialyzed for various reasons. The inclusion criteria were patients with ESRD and have regular established dialysis sessions at least one year before recruitment. For those who were not on dialysis, the patients must have attended the hospital initiated predialysis counseling sessions at least three months before study recruitment. Other criteria include the latest calculated (within a month of recruitment) patients's estimated glomerular filtration rate (eGFR) ≤15 mL/min/1.73 m3 and minimal age of 18 years or older. The exclusion criteria were pregnancy; presence of any type of acute psychiatric disorder that warrant hospitalization, acute medical illnesses, or malignancy; lack of capacity to give informed consent; inability to communicate fluently in Malay or English language; or illiteracy.
Study participants
The patients were recruited from the nephrology departments of two major tertiary hospitals in Klang Valley, Malaysia between September 2015 and September 2016. The sites were chosen to represent a standard clinical setting in the management of ESRD patients in the Malaysian healthcare system. All patients who received outpatient nephrology care or admitted to the nephrology/general medical ward were screened. All potential participants were invited to participate in the study following a brief introduction.
Data collection and instruments
The following data were acquired: demographics, weight and height, self-reported comorbidities, medications, and most recent blood investigation results, including hemoglobin, calcium, phosphate, albumin, and creatinine levels. Data were obtained from patients' medical records, electronic databases, and laboratory reports. eGFR was calculated using the chronic kidney disease epidemiology collaboration equation recommended by the 2012 Kidney Disease Improving Global Outcomes guideline. 24 The Charlson Comorbidity Index (CCI) was used to assess and quantify patients' morbidities. 25
Each patient completed the questionnaires. A face-to-face interview at the time of recruitment was conducted for patients who opted not for dialysis to ascertain the reasons behind such decision at a designated site. They were asked about the reasons for their decision and to list down possible influential factors for their decision.
The 30-item Dialysis Symptom Index (DSI) was used to assess the presence and severity of physical and emotional symptoms.26,27 This questionnaire explores the presence of 30 individual symptoms over the previous seven days. Severity of symptoms was rated by a 5-point Likert scale, ranging from “not at all bothersome” (0) to “very bothersome” (5). An average overall symptom burden score ranging from 0 to 30 was generated by summing the number of symptoms reported as being present. Test-retest reliability and content validity of the DSI questionnaire in advanced CKD patients with or without dialysis have been established in previous studies.26–28 A back-to-back translation of the DSI from English to Malay and vice versa was performed to enhance understanding and to minimize bias.
Negative emotional states (i.e., depression, anxiety, or stress) were assessed using a modified 21-item version of the original 42-item version. The Depression Anxiety Stress Scale (DASS-21), a validated and reliable instrument, was used to quantify distress along the three symptoms of stress, anxiety, and depression.29,30 The DASS-21 was chosen for this study to assist in the assessment of psychological disturbances within an individual which are intrinsically dimensional and varied in severity. It has a set of cutoff scores that characterize degree of severity (mild/moderate/severe) of each negative emotional state relative to the population. The validated Malay language translated version was readily available for general use and had good Cronbach's alpha values of 0.84, 0.74, and 0.79 for depression, anxiety, and stress, respectively. 31 The DASS is relatively independent of culture, religion, or level of spirituality and is easy and simple to administer to the general population in any clinical or nonclinical setting without any special training.
Statistical analysis
Statistical analysis was performed using the IBM Statistical Package for Social Sciences Processor (SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp). Categorical demographic and clinical characteristics were described as frequencies (%), with 95% confidence intervals, or as mean and standard deviation (SD). As the data were not normally distributed, between-group differences(demographic characteristics, clinical variables, prevalence and severity of individual symptoms, overall symptom burden, overall symptom severity, and depression) were assessed using nonparametric t tests or Mann-Whitney tests for continuous variables. The chi-square test, Fisher's exact test, and Kruskal–Wallis test were used for categorical variables. In each patient group, correlations among the overall symptom burden, overall symptom severity, and depression were analyzed using Spearman's correlation coefficient. A Bonferroni correction was applied for analyses of differences in the prevalence and severity of individual symptoms, with a two-sided p-value of <0.002 considered statistically significant. In all other analyses, a two-sided p-value of <0.05 represented statistical significance.
Ethical approval
This study received ethical approval from Universiti Kebangsaan Malaysia Research Committee (FF-2016-023) and Medical Research Ethics Committee (NMRR-15-1682-27993).
Results
Patients' demographic data
In total, 187 patients were screened and eligible for the study with a response rate of 100%. Table 1 shows almost comparable demographic data of the patients in both groups except for the education level. The ethnicities of the study group were as follows: Malay (58%), Chinese (34.2%), Indian (7%), and other ethnic minority (1.1%). The cause of ESRD in this study was consistent with the findings of other ESRD studies.6,8,9 One-third of the not dialyzed group have low education level compared to the dialyzed patients (p < 0.002). Only 28.8% had a total household income of RM 5OOO (approximately USD 1200) or more per month. The majority of patients (81.28%) had not been admitted to the hospital in the previous six months, and more than two-third (89.30%) reported to be independent and self-caring.
p < 0.05.
CCI, Charlson Comorbidity index; CKD, chronic kidney disease; SD, standard deviation.
Symptom burden and severity
Tables 2 and 3 illustrate the symptom burden and symptom severity experienced by the participants. The patients in both groups reported comparable symptom burden, with the five most common reported symptoms being tiredness, trouble staying asleep, sexual difficulty, dry skin, and trouble falling asleep. Some symptoms were more pronounced in the not dialyzed group such as worrying, dry skin and mouth, decreased appetite, numbness, and leg swelling (p < 0.05). The detail analysis of the symptom burden revealed that majority of participants in both groups experienced either no symptoms or mild-to-moderate symptom on the severity scores (Table 3). Slightly more than 10% of the patients from the not dialyzed group complained of severe level of tiredness and trouble staying asleep compared to the dialyzed patients; however, these were not statically significant symptoms (p > 0.05).
p < 0.05.
DSI = The 30-item Dialysis Symptom Index.
p < 0.005, Fisher's exact test and Pearson Chi-Squarea.
Bold indicates more intense in not dialyzed group but not significant (p > 0.05).
DSI = The 30-item Dialysis Symptom Index.
RRT, renal replacement therapy.
Assessment of negative emotional states
The DASS assessment revealed that up to 84% of patients in the not dialyzed group and 94.3% patients in the dialyzed group were with normal psychological status. Further analysis of both groups showed that 21 participants were depressed (11.2%), 21.8% were stressed, and 15.6% were anxious, and the incidence of these factors was significant in both groups (p = 0.030) (refer Fig. 1). The ESRD patients with depression, anxiety, and stress were found to have median score of 14 (interquartile range [IQR]: 18.0–10.0), 14 (IQR 17.5–12.0), and 12 (IQR 13.5–10.0) on total symptoms and score of 32 (IQR: 42.0–20.0), 28 (IQR 35.5–22.5), and 25 (IQR 29.5–20) for severity of symptoms on DSI (p < 0.005), respectively (refer Figs. 2 and 3). Out of 16 patients of the not dialyzed group with depression, 1%, 5%, and 10% of these patients scored severe, moderate, and mild level of depress axe on DASS-21 assessment accordingly. Patients in the dialyzed group showed more positive psychological well-being trend overall on DASS-21 assessment compared to patients in the not dialyzed group; however, this is not statically significant (p < 0.146).
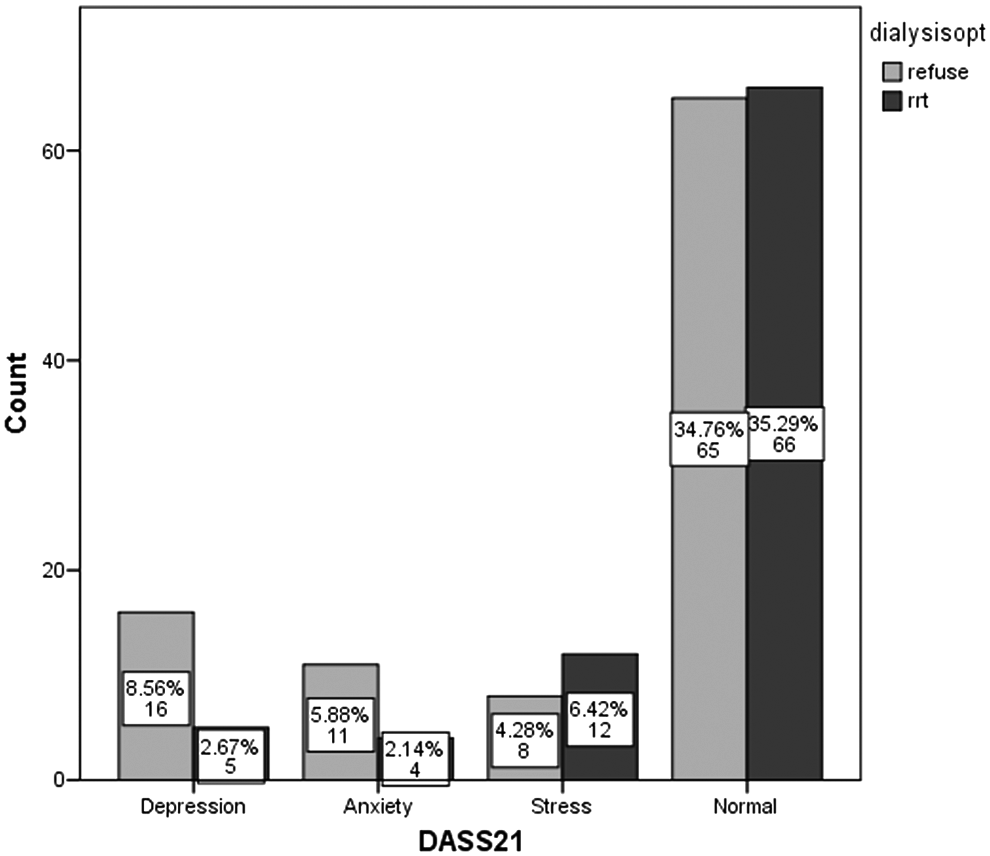
Prevalence of Psychiatric disorder among ESRD patients, n = 187 (100%). ESRD, end-stage renal disease; RRT, renal replacement therapy.
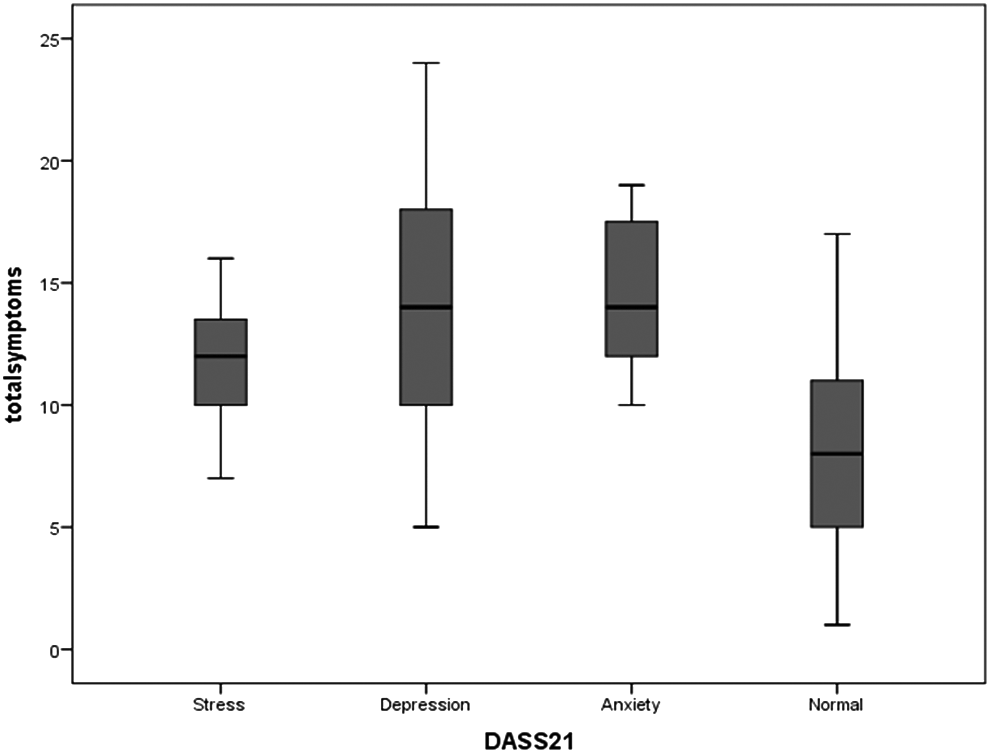
Median and IQR of total symptoms in ESRD patients who had psychological burden. IQR, interquartile range.

Median and IQR of severity of symptoms in ESRD patients who had psychological burden.
A Spearman's rank-order correlation analysis showed a positive correlation with total symptom and severity of symptoms of the participants regardless of whether they were dialyzed or not dialyzed. On bivariate analysis, the overall participants' total symptoms, rs(310) = +0.50, p < 0.05, and the severity of the symptoms, rs(310) = +0.54 p < 0.05, were positively correlated to their states of negative emotional instability. In general, patients with psychological disturbances were experiencing more symptoms and higher severity of symptom score compared to those who felt they were not depressed, stressed, or anxious regardless of whether they were being dialyzed or not (p < 0.005).
Patients with ESRD and not dialyzed
In total, 53.5% of the ESRD patients who participated in this study opted not for dialysis for various reasons and detail analysis represented heterogenous groups of patients. Up to 26% of patients with eGFR ≤15 mL/min/1.73 m3 at the time of study recruitment and strongly recommended for dialysis by the nephrology teams had opted not for dialysis at the time of the interview. This group of patients had not made a definitive decision about the future direction of their treatment. There were 34% of participants who were grouped as comprehensive conservative care group as suggested by Kidney Disease: Improving Global Outcomes (KDIGO) classification 2015 which defined as conservative care that is chosen or medically advised. 24 Up to 40% of the End Stage Renal Failure (ESRF) patients in this group were classified as choice-restricted conservative care. 32 None of the participants cited religious or spiritual beliefs, as the limiting factors in their decision did not receive an active form of RRT.
Discussion
The prevalence of the symptom burden in our cohort of ESRD patients was almost comparable, regardless of dialyzed versus not dialyzed treatment. However, the degree of physical symptom severity of the nondialysis patients was higher compared with the active RRT patients, but none of the symptoms showed statistical significance post Bonferroni correction. Interestingly, a higher total symptom burden and high degree of symptom severity were positively correlated with a higher prevalence of psychological disturbances. There was a trend of higher psychological disturbances among those who opted not for dialysis than among those who selected RRT; however, this was not statistically significant.
Comparative study on symptom prevalence and burden in dialyzed and nondialyzed groups was not extensive. However, the high symptom burden and severity among patients with advanced CKD and ESRD, regardless of the type of treatment, are well known.12,13,31 Murtagh et al. reported the symptoms experienced by patients who opted for no dialysis as 11.58% per-patient and these symptoms included lack of energy, fatigue, pruritus, dyspnea, pain, dry mouth, muscle cramp, sleep disturbances, poor concentration, constipation, and nausea. 33 The nondialysis patients may experience more complex symptoms that are difficult to treat like dyspnea secondary to fluid overload and extreme lethargy as the disease progressed. 34
The types of symptoms commonly experienced by the participants of this study were almost consistent with those reported in previous similar studies on symptom burden and severity among ESRD patients.12,13 Similar biochemical findings in our ESRD patients regardless of their treatment could be the most possible reason to explain such experience; however, this factor was not found to be statically significant on further analysis. In a clinical audit of ESRD patients who had been treated without dialysis, the symptom prevalence was reported to be high; however, this study group of patients experienced a different type of symptoms, with the most prevalent symptoms being weakness (75%), poor mobility (75%), poor appetite (58%), pain (56%), pruritus (56%), and dyspnea (49%). 35 The symptom burden and severity found in this audit were not correlated to factors such as disease severity (eGFR), the number of symptoms, and the total of mean symptom scores. 35 A previous study observed a higher symptom burden among patients with advanced CKD and ESRD and found that factors such as dialysis, older age, and female sex independently predicted the severity of symptoms. 31 Various studies demonstrated a relationship between total symptom burden and low hemoglobin, ethnicity, and a longer duration of dialysis.36,37 However, in the present study none of these epidemiological factors predicted increased symptom burden or severity.
The prevalence of depression over time among ESRD patients was reported as 19–24% in a large prospective study conducted in the United States. 38 In a study of predialysis patients with stage 3–5 CKD, they found that the depression and anxiety of patients increased as their diseases progressed. 39 Depression and up to some extent anxiety have been studied in great detail among those with ESRD; however, data on comparative quantitative measure of emotional syndromes associated with dialyzed and not dialyzed ESRD patients are very minimal. In this study, the DASS-21 score may represent an assessment of psychological disturbance and needs to be interpreted in conjunction of other clinical information in this case, the symptom burden and its severity. The present study showed that negative emotional states were correlated significantly with higher total symptom burden and symptom severity scores. In addition, we found that the nondialysis patients were more depressed and anxious, but less stressed than the patients in the active treatment group. Overall, the ESRD participants' median scores of DASS-21 in all domains were found to be higher than the cutoff value for the extremely severe level of psychological abnormalities regardless of their dialysis status. In a study of hope therapy among patients undergoing hemodialysis in Iran, the emotional disturbances were recorded as above the cutoff for severe score for depression and anxiety and mild to moderate score for stress before the intervention in comparison to placebo. 40
Studies of ESRD have demonstrated a link among depression, impaired QoL, and mortality.12,13,21,22,27,38 In addition, Boulware et al. reported that depressive symptoms among ESRD patients were strongly associated with greater risks for all-cause deaths and cardiovascular disease events. 38 Overall, they concluded that persistent and current depressive symptoms were associated with poor medical outcomes. 38 Thus awareness among renal medical providers at all levels of the high burden of symptoms and depression in many patients with advanced CKD/ESRD is necessary to ensure the implementation of appropriate symptom-alleviating and antidepressive therapies.
The other aspect in this study is the importance of socioeconomic status as a determinant in the care of ESRD patients. In the present study, 75% of patients who fall into the category of choice-restrictive conservative care had household incomes of less than RM 5000 (USD 1120) per family/month. The additional financial burden that dialysis treatment would place on the total family expenditure was consistently cited as a reason for refusing dialysis. A study of the costs of HD and CAPD in Ministry of Health hospitals in Malaysia showed that the cost per treatment of each session ranged from RM 80 (USD 18) to RM 475.79 (USD 113), with a mean cost of RM 169 (USD 40) per HD, which was equivalent to USD 23,549.42 annually.39,40 The cost of CAPD treatment ranged from RM 1400 to RM 3200 per patient/month, with a mean of RM 2186, equivalent to USD 23, 431.51 annually.39,40 The per-annual total cost for HD and PD in Malaysia is lower than that in other countries (e.g., Nigeria). However, it still represents a significant cost overall to the total medical health system, taking into account the current economy and currency instability and increased incidence of ESRD.6,7,39,40 Given the cost burden, it is not surprising that 61% of those who opted not for dialysis at the time of the interview remained undecided about dialysis in the future, although they were willing to have dialysis in the event of an acute crisis.
Limitations
This study has several limitations. A relatively small number of ESRD patients in this study have reduced the generalization of the results for a larger geographical area and, therefore, limit the power to study various associations between participants' symptom burden and severity to QoL and life expectancy. We used the validated and reliability proven English version of the 30-item DSI in this study, and measures were taken to maximize participants' understanding; however, the application of this tool among patients from various ethnic backgrounds of the Malaysian population may have influenced the outcome of the study. Therefore, modifications of the validated DSI (English version), translated to Malay or Chinese languages with cross-culture adaptation, are needed for future studies. In addition, this study should be done in a more controlled setting, where all the advanced CKD/ESRD patients are given a standard counseling and information to improve their understanding of RRT before recruitment in the study. By doing this, perhaps we will be able to obtain more robust understanding of the patients' reasons for refusing the RRT.
Conclusions
The symptom burden of ESRD patients receiving active dialysis treatment was similar to that of not dialyzed patients. A higher symptom burden and the presence of severe symptoms seemed to be predictive of future psychological disturbances. Disease-related symptoms should be identified and care plans put in place to reduce the potential development of psychological disorders among ESRD patients. More research on ESRD patients who opt for conservative treatment is necessary to understand the biopsychosocial elements underlying their decisions and indecisiveness during this critical period of life. The inclusion of clinical team members, such as experts in palliative medicine, may assist in the management of ESRD patients earlier in their disease trajectory.
Footnotes
Acknowledgments
This study was part of a thesis dissertation to fulfil the requirement for the Master of Internal Medicine at Department of Medicine, Universiti Kebangsaan Malaysia. The authors thank the Director General of Health of Malaysia Ministry of Health and Serdang Hospital for their support.
Author Disclosure Statement
No competing financial interests exist.