
Abstract
Abstract
Background:
Older Latinos with serious medical conditions such as cancer and other chronic diseases lack information about advance care planning (ACP). ACP Intervention (ACP-I Plan) was designed for informational and communication needs of older Latinos to improve communication and advance directives (ADs).
Objective:
To determine the feasibility of implementing ACP-I Plan among seriously ill, older Latinos (≥50 years) in Southern New Mexico with one or more chronic diseases (e.g., cancer, heart disease, renal/liver failure, stroke, hypertension, diabetes, chronic obstructive pulmonary disease, and HIV/AIDS).
Design:
We conducted a prospective, pretest/post-test, two-group, randomized, community-based pilot trial by using mixed data collection methods.
Setting/Subjects:
Older Latino/Hispanic participants were recruited from community-based settings in Southern New Mexico.
Methods:
All participants received ACP education, whereas the intervention group added: (1) emotional support addressing psychological distress; and (2) systems navigation for resource access, all of which included interactive ACP treatment decisional support and involved motivational interview (MI) methods. Purposive sampling was guided by a sociocultural framework to recruit Latino participants from community-based settings in Southern New Mexico. Feasibility of sample recruitment, implementation, and retention was assessed by examining the following: recruitment strategies, trial enrollment, retention rates, duration of MI counseling, type of visit (home vs. telephone), and satisfaction with the program.
Results:
We contacted 104 patients, enrolled 74 randomized to usual care 39 (UC) and treatment 35 (TX) groups. Six dropped out before the post-test survey, three from TX before the post-test survey because of sickness (n = 1) or could not be located (n = 2), and the same happened for UC. Completion rates were 91.4% UC and 92.3% TX groups. All participants were Latino/Hispanic, born in the United States (48%) or Mexico (51.4%) on average in the United States for 25 years; majority were female, 76.5%; 48.6% preferred Spanish; and 31.4% had less than sixth-grade education. Qualitative data indicate satisfaction with the ACP-I Plan intervention.
Conclusions:
Based on enrollment and intervention completion rates, time to completion tests, and feedback from qualitative post-study, follow-up interviews, the ACP-I Plan was demonstrated to be feasible and perceived as extremely helpful.
Introduction
I
Underserved patients with low socioeconomic status and limited English proficiency lack information about ACP and experience significant disparities (e.g., education, economic, social, linguistic, and cultural), limiting optimal decision making and EOL care communication.10–12 For example, individuals who do not speak English may also lack access to translation services, which hinder interactions with healthcare providers,13,14 making it difficult to communicate about ACP. 11 Careful consideration about ACP education is especially important for racially and ethnically diverse patients (i.e., African Americans and Latinos). 8 Along with a growing prevalence of multiple chronic conditions, U.S. Hispanics experience gaps in communication 15 and significant barriers to management of their conditions. 16 Older Latinos, living with serious illnesses, are especially vulnerable to misinformation because of disparities, limiting information provision and contributing to differential treatment, which plays an important role in medical decision making. 17
Cultural beliefs and values also influence communication. Sociocultural factors influence ACP education and healthcare decision making stemming from patients' cultural beliefs and experiences for receiving such information.10,18 Latinos may not ask their healthcare providers direct questions or follow treatment plans, creating confusion between patients, family members, and providers. 19 Lack of knowledge and ACP information create problems for EOL decision making. 11 Factors such as low health literacy10,12,20 contribute to communication barriers and disadvantages for Latinos, 21 which impact poor health outcomes.17,22,23 Although Latinos may prefer less-aggressive EOL treatment, they often have not documented or communicated their preferences to anyone. 24 Although Latinos tend to accept more aggressive medical treatment compared with non-Hispanic whites,25,26 they often die in the hospital instead of at home without hospice care.27,28 Out of respect for healthcare providers, Latinos are known to follow physicians' treatment recommendations, often without asking questions because they may perceive that physicians have more education and knowledge in medicine, placing them in positions of authority. 29 This indicates that when Latinos do not speak up about their preferences they could be accepting unwanted treatment without understanding or being aware of the implications of these actions. Cultural beliefs and values also influence preferences, suggesting that faith and family drive patient preferences. 19 For example, Latinos can prefer to die at home, 27 indicating that they prioritize the needs of the family over his or her own 18 and have a desire to be close to extended-family networks; however, we have limited understanding about preferences for ACP communication or EOL care preferences for home, hospital, or other places of death. In addition, we lack understanding about family involvement in this process.
ACP education and decision-making discussions should happen early and often to inform everyone involved before the need for decision making. An early approach includes culturally adapted information 10 and individualized care 30 to improve EOL decision making to identify personal preferences. Initiation of early EOL conversations can lower distress among seriously ill individuals, improving quality of life.31,32 As suggested by the IOM Health Literacy and Palliative Care Workshop, 20 community settings present a place where ACP education can openly occur, meeting the community needs, thereby reducing disparities. 33 Instead of relying on healthcare providers to begin ACP conversations, education can happen, for example, in church settings and senior centers. Some individuals are open and prefer to receive ACP education in community-based settings34–36 ; however, very little research has been conducted with older, chronically ill Latinos, which is especially sparse among those living in rural settings. There is a growing need to educate older Latinos.
There are relatively few population-based research studies that pilot test the feasibility of conducting interventions with participants of similar sociodemographic characteristics (e.g., age, race, socioeconomic status, and education) 37 and none that focus on a Hispanic population from a particular region with these characteristics and need for ACP information. Very few interventions are designed and tested to address ACP with this specific population, and none, to the best of our knowledge, have been conducted within community-based settings with older Latinos. This study addresses a key problem in ACP education among seriously ill older Latinos living in Southern New Mexico that examines feasibility and satisfaction of an ACP Intervention (ACP-I Plan) that is designed to meet informational and communication needs for ACP.
Methods
Design and participants
We conducted a prospective, pretest/post-test, two-group, randomized, community-based pilot trial by using mixed data collection methods. This study is a smaller part of a larger research project. In this study, we evaluate the feasibility of implementation and satisfaction with the ACP-I Plan. This feasibility study stems from pilot research wherein older Latinos were randomly assigned by flipping a coin to the ACP-I Plan treatment intervention group (TX) or usual care (UC).
Sampling methods considered a sociocultural framework (Fig. 1) to purposively recruit Latino participants from community-based settings in Southern New Mexico and to maximize outreach efforts to the community. Using this framework, recruitment criteria included individuals, organizations, and communities to reach Hispanics/Latinos, age >50, living in Southern New Mexico, and having one or more chronic diseases (e.g., cancer, heart disease, renal/liver failure, stroke, hypertension, diabetes, chronic obstructive pulmonary disease, and HIV/AIDS). Recruitment data identified language preference, English/Spanish, or both.
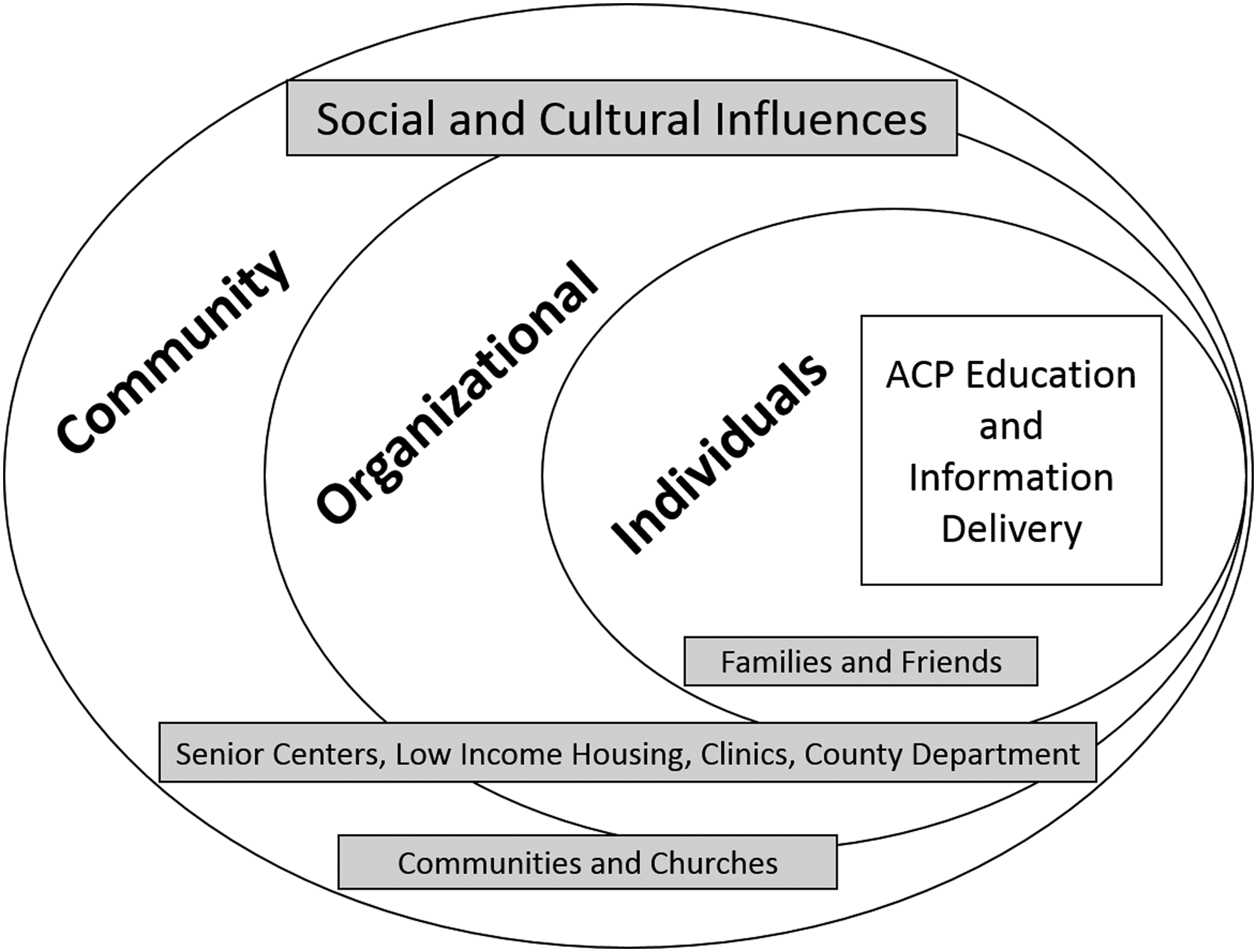
Sociocultural context for recruitment strategies. ACP, advance care planning.
Screening assessed for conditions that could influence understanding of the intervention, excluding individuals if they answered yes to: “Has a doctor ever told you that you have: schizophrenia, schizoaffective disorder, or manic/depressive disorder?” Exclusion criteria included the possibility of limited cognitive functioning that could impact decision making and research participation that asked, “Has a doctor ever told you that you have Alzheimer's disease?” Recruitment targeted populated urban and semirural areas in Southern New Mexico and surrounding colonies that are areas largely unregulated near the United States–Mexico border with minimal resources, high poverty, substandard housing, limited water sources, and inadequate roads. 38
Procedures
The New Mexico State University Institutional Review Board reviewed and approved the protocol and materials for this project. Patients provided written consent and received incentives for their participation: $5 for a screening interview to determine eligibility, $20 for a baseline survey, and $20 for completing a post-test survey. Written materials were available in English and Spanish. Per protocol, eligible participants were expected to complete a pretest survey soon after they screened as eligible, agreed to participate, and consented to the study. After the pretest survey, participants in the intervention group were scheduled and expected to complete one motivational interview (MI) counseling session after the educational session and within 30 days. Participants in both groups were expected to complete a post-test survey on or soon after 30 days from the pretest survey. 39
A masters of social work (MSW) trained social worker provided participants with ACP education and counseling. Two study MSWs were trained on the intervention model, with approximately five hours of in-depth training to learn and practice ACP educational delivery, counseling, supportive communication techniques, and manage barriers. The intervention also addressed cultural elements that were shown to reduce barriers to ACP acknowledging individuals attitudes, beliefs, and knowledge about ACP. 40 Additional training was provided to MSWs, with weekly team supervision meetings over the course of eight months, led by principal investigator (PI) to guide delivery of the intervention and improve recruitment strategies. MSWs administered all pretest/post-test surveys and conducted in-depth interviews.
Usual care group
General AD education was provided to all participants and included verbal and written information about ACP and ADs. During recruitment, AD information was introduced to all participants through a brief educational session before entering the study. We discussed specific information about the importance of appointing someone as power of attorney for healthcare decision making. We also discussed the application and limitation of medical decision making when an AD is needed, when an individual becomes unable to communicate their wishes for medical treatment. Education discussed decision making about medical treatment preferences to document on AD forms for specifying EOL care preferences. During ACP educational sessions, individuals asked questions about the forms to clarify any confusion on the process of documenting an AD. They were also encouraged to return to their healthcare providers with any medical questions that could influence decision making and AD documentation.
Treatment intervention group
The ACP-I Plan treatment intervention added one counseling session to general education about ACP to improve communication and AD documentation, combining interactive ACP treatment decisional support, counseling/emotional support, and barrier navigation. The intervention includes MI counseling39,41 and client-centered supportive care42,43 to encourage early ACP communication with healthcare providers and family members, addresses psychological distress through supportive counseling, and connects individuals to resources through patient navigation if needed.10,19,40,44 MI counseling uses a manualized protocol that is designed to help individuals explore their individual attitudes, beliefs, and knowledge about ACP. The MI session included supportive counseling for dealing with illness and talking to doctors, families, and friends about ACP, and it also explored “what is most important to you?” while considering attitudes and beliefs for talking about and/or planning EOL care. The TX group received a one-time MI session for 30–40 minutes; however, the amount of time spent with participants was individualized and based on request for more or less time. Per protocol, to individualize care, an additional follow-up session was offered as needed. Three participants requested and received an additional brief follow-up counseling discussion, which lasted no more than 15 minutes.
Feasibility measures
Before implementation, proposed benchmarks for feasibility were defined for indicators described in this section (Table 3). Feasibility is indicated by sample recruitment and study implementation examining the following: recruitment strategies to indicate a broad range of various methods and descriptive data on the demographics to show information about the target population. Screening measures in recruitment were used to report age, race, type of chronic medical conditions, number of emergency room (ER) or urgent care visits, and number of hospitalizations in the past six months to indicate the severity of illness on recruitment. We tracked language preference (English/Spanish) and type of preferred visit (face to face vs. telephone). Feasibility was also measured by number of participants screened, number enrolled, retention rate, attrition rate, duration of MI counseling, and satisfaction with the program. 42 We also tracked38,40 the time it took between screening to pretest survey and to post-test survey, as well as the examining of the duration and type of visit (phone or in-person).
Data analysis
Mixed qualitative and quantitative methods were used to examine the feasibility of recruitment and satisfaction with the program, including data from screening, pretest/post-test surveys, and qualitative interviews. Baseline data were used to examine the feasibility of recruitment and qualitative semistructured, open-ended interviews 45 were used to examine satisfaction as acceptance with the intervention. Tests for significance and change scores from pretest to post-test were not done as this study focused on feasibility. Measures of feasibility were calculated. Satisfaction was assessed as a proxy for acceptance with and retention in the program. Qualitative interviews were conducted after participants completed the post-test survey. A semistructured interview guide included questions on: satisfaction with ACP education, ACP communication with family and healthcare providers, social and cultural factors that influence discussions, emotions such as fear or denial that influence ACP communication, and suggestions for improvement of ACP information (Table 1).
ACP, advance care planning.
Data from all sources, including audio recordings, transcribed interviews, team meeting memos, notes, and case summaries, were used for descriptive analysis that were analyzed in Atlas.ti, an analytical software 46 using a constant comparative method and thematic analysis.47,48 Analysis involved a team approach and iterative methods to identify salient themes regarding recruitment strategies in community-based settings and to explore satisfaction. First, to ensure trustworthiness of the findings, 49 two team members (coauthors, K.J.G. and A.Q.) reviewed and coded the data independently, creating categories, subcategories, and themes inductively from the codes. Then, a third person (F.N.H.) reviewed the coding schema and refined the concepts. Team meetings and multiple discussions were used to resolve discrepancies and to reach a coding consensus. Once key findings were identified, a fourth team member, who did not participate in data collection, reviewed the coding strategy to summarize the identified concepts, themes, and subthemes that emerged.
Results
Feasibility outcomes
Recruitment strategies
Using the sociocultural framework, we maximized recruitment with outreach methods to reach a maximum number of participants for the study. Outreach was conducted by reaching individuals, families, and friends, and at the organizational and community levels. As a research team, two MSW trained social workers who were fluent in Spanish entered the community weekly for a six-month period, posting information about the study as well as talking with people who were interested in this study. The process of recruitment included posting and handing out flyers, sending e-mails to community members, holding meeting with stakeholders in governmental agencies, and providing AD educational sessions with older adults in senior community centers, social service agencies, low-income housing projects, food banks, grocery stores, local community churches, and assisted living facilities. In terms of the number of people approached before recruiting the target population, ∼225 flyers were given out during the recruitment period.
Sociodemographic characteristics
Demographic information about the sample indicates the likelihood of actually recruiting the target population, which is especially important for Latinos/Hispanic individuals who historically have neither participated in research 37 nor received ACP education in English or Spanish. Table 2 summarizes the background characteristics of the participants. The mean age of participants was 65.79 (standard deviation [SD] = 8.71; range 50–87). The majority were women, 76.5%. All participants identified as Latino/Hispanic, born in the United States (48%) or born in Mexico (51.4%) on average living in the United States for 25 years, 52.9% preferred Spanish, and 31.4% had less than sixth-grade education. For illness severity, participants had at least one chronic condition (10.3%); however, most had 2 (51.5%) or 3 (32.4%) conditions, with urgent care needs (38.2%, ER, urgent care, or hospitalization).
COPD, chronic obstructive pulmonary disease; ER, emergency room; SD, standard deviation; UC, usual care.
Participation
We contacted 104 patients (Fig. 2); 74 agreed to participate and were randomized 39 to UC versus 35 to TX. Three dropped out before the post-test survey because they were too sick (n = 1) or could not be located (n = 2), and 3 patients from UC dropped out before the post-test survey. The overall completion rate was 92%, with 91.4% for UC and 92.3% for TX groups.
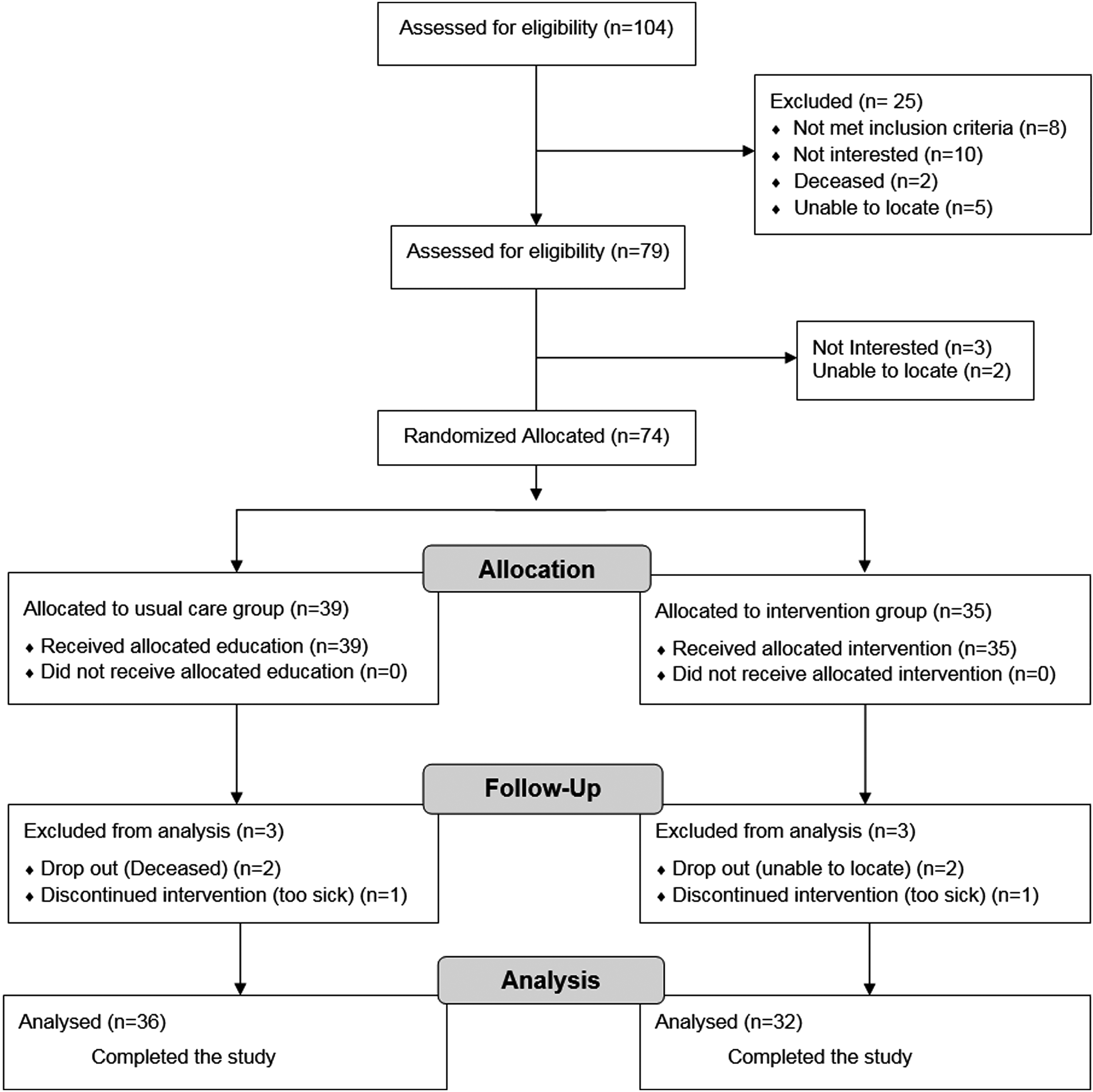
Study enrollment.
Time
See Table 3 for actual measures of feasibility. On average, pretest surveys were completed nine days after eligibility screening (median = three days, SD = 15.32), MI counseling was conducted 18 days after screening (median = 14, SD = 13.90), and post-test surveys were completed 14 days after the pretest survey (median = six days, SD = 19.42). For the duration of MI counseling to encourage ACP communication and AD documentation, participants were expected to participate in a 30- to 40-minute session. On average, this one-time session took ∼30 minutes (mean = 33 minutes, SD = 10.11 minutes). For the MI session delivery format, 22% of the sessions were conducted over the telephone and 78% were conducted face to face.
Variation for proposed sampling and recruitment strategy.
MI, motivational interview.
Satisfaction
All participants reported having a positive experience with ACP-I Plan (Table 4). Many said that ACP information was useful and fulfilled a gap in knowledge or information that brought attention to ACP and ADs. For some, it was the first time they had learned about ACP. Others said that the program added information that helped them to think and/or to talk with family members and doctors about ACP. One participant said,
TX, treatment; UC, usual care.
I'm real happy with it. You kind of asked me questions that I never even thought about…like, questions I didn't want to think about and showed me a lot about the will. Now, I can deal with it. So that's helped me a lot. (74 UC)
Participants were satisfied because the program fulfilled a need to be prepared for the future when entering the hospital or when their family members are called to make decisions. Although most participants talked about satisfaction, some (16%) indicated being simply satisfied without providing more information about their satisfaction. Among these individuals, they either spoke Spanish only with having less than a sixth-grade education or were English speaking with only a high school degree. Limited expressions of satisfaction appear to indicate gaps in health literacy and ability to articulate ideas about ACP.
Participants provided positive feedback and suggestions to improve the ACP-I Plan intervention (Table 4); comments suggest increasing the number of educational sessions in various community settings where older adults can talk about the process of ACP. Some participants emphasized that older adults need vital ACP information repeated multiple times so that they have concrete examples and suggestions about documenting an AD. Although the information was clear and straightforward, participants would like MSWs to encourage them to ask more questions, especially because they may have difficulty understanding the information. Another consideration for improvement included aspects of faith and religiosity in the discourse on ACP to allow people to express how they feel about the process and their faith. Some participants suggested engaging chaplains or their church pastors so that there could be an ACP discussion that incorporated aspects of their faith in communication. Talking about ACP can raise emotions such as anxiety or fear about dying. Since these discussions take time, participants suggested that providers allow for more time so that feelings can emerge to be expressed in the process.
Discussion
This study highlights findings of a randomized, community-based pilot trial ACP-I Plan and explores the feasibility of implementation and satisfaction with the program, providing suggestions for improvement. Findings indicate that the ACP-I Plan is feasible to implement in Southern New Mexico with older Latinos and that participants were satisfied with the program. Although previous research finds low participation rates among Hispanics/Latinos in research, this study successfully enrolled and completed the trial with 68 participants enrolled from Southern New Mexico.
The ACP-I Plan intervention development was guided by a conceptual model of MI that intended to improve ACP communication and AD documentation for Hispanic/Latinos with chronic medical conditions. Recruitment methods implemented in Southern New Mexico to enroll the study population resulted in 74 participants who were randomly assigned to UC and intervention groups; there was an overall participation rate of 93.7%. Based on enrollment and intervention completion rates, time to completion, and feedback from a qualitative post-study, follow-up interviews, the ACP-I Plan was demonstrated to be feasible and perceived as extremely helpful. This is important because no study to date has been conducted with this population and implemented in a community-based setting.
When older Latinos experience chronic illness, they may become more vulnerable when entering the medical system. Without previous decision-making discussions and lack of AD documentation, they may rely on family members 50 ; however, surrogate preferences can differ from patients' goals, leading to family conflict regarding treatment options.51,52 This study indicates that older Latinos are receptive to ACP communication and appreciate an opportunity to begin early discussions to prevent family conflict and confusion for everyone.
Disparities and added vulnerabilities for Latinos indicate the importance of early ACP education. Although vulnerability is a human condition that influences healthcare delivery, certain populations experience disparate circumstances that negatively impact information delivery and lead to misinformation and gaps in care. 53 Some individuals encounter hardships and are more vulnerable than others, living with poverty, homelessness, or disability influencing differential treatment in EOL care. 54 Our study addresses this gap by targeting the specific population with a culturally adapted approach to ACP information, providing individualized attention to their educational and linguistic needs.
Limitations
Several considerations and limitations should be considered. The ACP-I Plan was designed as a multifaceted intervention to provide ACP education and counseling to chronically ill, older Latinos to explore the possibility of recruitment and implementation of ACP. Purposive, convenient sampling was used to expand recruitment strategies that could influence a selection bias toward recruiting participants for this study. Therefore, data should not be generalized to all older Latinos. Future research will consider methods to control for selection bias. In addition, since healthcare providers should routinely integrate ACP information into daily practices, especially with seriously ill patients, it is unclear how much ACP information was received or understood before beginning the study. In future research, it is essential to assess knowledge of ACP on screening.
Conclusion
Based on enrollment and intervention completion rates, time to completion, and feedback from qualitative post-study, follow-up interviews, the ACP-I Plan was demonstrated to be feasible and perceived as extremely helpful in understanding and navigating ACP.
Footnotes
Acknowledgments
The authors thank the participants who were the reason for developing and pilot testing the Advance Care Planning Intervention (ACP-I Plan) intervention, with a special appreciation for the Southern New Mexico community members who supported this research program. The ACP-I Plan pilot study was supported by the Mountain West, Clinical Translation Research Infrastructure Network (5U54GM104944 pilot grant).
Author Disclosure Statement
No competing financial interests exist.