
Abstract
Abstract
Background:
There are few published comfort care order sets for end-of-life symptom management, contributing to variability in treatment of common symptoms. At our academic medical centers, we have observed that rapid titration of opioid infusions using our original comfort care order set's titration algorithm causes increased discomfort from opioid toxicity.
Objective:
The aim of this study was to describe the process and outcomes of a multiyear revision of a standardized comfort care order set for clinicians to treat end-of-life symptoms in hospitalized patients.
Design:
Our revision process included interdisciplinary group meetings, literature review and expert consultation, beta testing protocols with end users, and soliciting feedback from key committees at our institutions. We focused on opioid dosing and embedding treatment algorithms and guidelines within the order set for clinicians.
Setting:
The study was conducted at two large academic medical centers.
Results:
We developed and implemented a comfort care order set with opioid dosing that reflects current pharmacologic principles and expert recommendations. Educational tools and reference materials are embedded within the order set in the electronic medical record. There are prompts for improved collaboration between ordering clinicians, nurses, and palliative care.
Conclusions:
We successfully developed a new comfort care order set at our institutions that can serve as a resource for others. Further evaluation of this order set is needed.
Introduction
P
One demonstrated gap at the end of life in inpatient settings has been in the adequate and appropriate provision of opioids in the context of comfort-focused care. 14 Standardizing orders has been proposed as a way to manage patients' symptoms in a more timely manner.15–17 In 2001, our institution published guidelines for end-of-life care in the intensive care unit, including a comfort care order set for withdrawing life-sustaining treatment. 18 This order set was based on historical practices of sedation and analgesia in critical care settings that included frequent use of continuous opioid and benzodiazepine infusions to manage acute symptoms.18,19 Evaluation of this comfort care order set showed increased use of opioids and benzodiazepines without evidence of hastening death and the order set was associated with high levels of physician and nurse satisfaction.20,21 The comfort care order set for withdrawing life-sustaining treatment was then adapted for use on our acute care floors. These order sets will be referred to from hereon as the original comfort care order set. Since implementation of our original comfort care order set, practice for sedation and analgesia has changed, with reduced use of continuous infusions.19,22
As practices for sedation and analgesia changed, some comfort care protocols or order sets have come under scrutiny due to safety concerns and lack of evidence. 23 In particular, concerns have recently been raised about the use of the Liverpool Care Pathway in vulnerable populations and concerns that death was hastened. 24 Additionally, comfort care order sets that emphasize high-dose opioids (especially morphine and hydromorphone) and rapid opioid infusion titration put patients at risk for opioid-induced hyperalgesia (OIH), which can increase discomfort. 25 We had anecdotally observed patients with signs of increased discomfort from opioid toxicity when treated with high-dose intravenous (IV) opioids. Rapid opioid infusion titration may also hasten death. In 2016, with only one very low-quality, randomized control trial of a comfort care protocol available, a Cochrane Review reported a lack of strong evidence supporting end-of-life pathways, but concluded that the principles underlying these pathways are still relevant. 23
For these reasons, we sought to revise the comfort care order set utilized at two large academic hospitals with a goal to provide better symptom management for patients receiving comfort-focused care at the end of life and to provide more guidance and support for clinicians, nurses, and other staff involved in caring for patients at the end of life. We believe that our process and results may be useful to other institutions interested in developing or revising comfort care order sets that better align with current sedation, analgesia, and pharmacologic principles.
Methods
Step 1: Identifying problems with the original comfort care order set
An interdisciplinary group of physicians, nurses, and pharmacists from the two large academic hospitals (authors Bender MA, Hurd C, Solvang N, Colagrossi K, and Matsuwaka D) was formed to evaluate our original comfort care order set. We started by identifying problems with this comfort care order set through our own clinical experience and feedback from colleagues in palliative care and other specialties, medical trainees, nurses, pharmacists, respiratory therapists, and others. We also reviewed patient safety reports related to end-of-life care from the previous two years.
Through this process, we identified three key addressable problems with our original comfort care order set: (1) little guidance to clinicians and nurses for providing basic management of pain and other symptoms with opioids; (2) the algorithms allowed nurses to rapidly titrate opioid infusions, which sometimes resulted in OIH; and (3) insufficient collaboration between nurses, ordering clinicians, and the Palliative Care Service (Table 1).
Step 2: Development of a new comfort care order set
To address the key problems with our prior order set identified above, we developed a new order set over a three-year period. Our interdisciplinary group met approximately every other month during the development process. We then met roughly quarterly to obtain feedback from a larger group, including administrative faculty and staff, the pain services at our institutions, representatives from critical care and acute care units, pharmacists specializing in informatics, pain, medication safety, and pharmacy operations, electronic medical record experts, and clinicians and nurses who regularly use the comfort care order set.
To address concerns about rapid opioid infusion titration, we reviewed literature on opioid pharmacology and consulted national physician and pharmacist experts both within and outside of our institutions. Based on this, we incorporated four key pharmacologic principles into our titration algorithms:15,26,27
(1) Infusion titration, when needed, should occur close to the steady state (4–5 half-lives, or for morphine 8–20 hours) of a drug, (2) As needed (PRN), IV opioid boluses should be used to manage acute symptoms while waiting for the infusion to reach steady state, (3) If a PRN IV opioid bolus is ineffective, another bolus can be given after the first bolus reached peak effect (5–20 minutes), (4) If a PRN IV opioid bolus remains ineffective after 2–4 doses, the dose can be safely increased.
We also reviewed literature on comfort care protocols. There are few published comfort care protocols, and guidance within the protocols on opioid choice and dosing varies (Table 2). The end-of-life symptom management order (ESMO) protocol, like our original comfort care order set, allows for rapid titration of opioid infusions.28,29
BEACON, Best Practices for End-of-Life Care for our Nation's Veterans; ESMO, end-of-life symptom management order; LCP, Liverpool Care Pathway; PCAD, Palliative Care for Advanced Disease; PRN, as needed; RCT, randomized control trial.
Last, we beta-tested revised versions of the order set with nurses and ordering clinicians and presented our work to relevant institutional committees, for example, medication safety, critical care steering, and medical staff advisory committees, to solicit feedback.
Through this comprehensive process, we developed a comfort care order set that better reflects the pharmacology of opioids and current practice in intensive care settings for sedation and pain management.
Step 3: Implementation of the new comfort care order set
There were several steps necessary to implement the new comfort care order set at our hospitals (Table 3). These include approval by the hospital administrations and relevant committees, changing the ordering system in the electronic medical record, and informing and educating faculty and staff on the changes. This has been a significant change for our institutions, and ongoing training to shift the culture around opioid use for patients receiving comfort-focused care will be needed. We developed an interactive online learning tool for inpatient nurses and incorporated the comfort care order set into orientation and continuing education courses. We trained nurse champions to provide 1:1 teaching at the bedside and completed in-services for our Palliative Care Services who are available 24/7 and review a daily census of patients on comfort care to offer assistance to primary teams and nurses if needed.
Results
Results are summarized in Table 1. The new comfort care order set proposes several solutions to the problems we identified: (1) little guidance on managing pain and other symptoms with opioids, (2) rapid titration of opioid infusions resulting in OIH, and (3) insufficient collaboration between nurses, ordering clinicians, and the Palliative Care Service.
Solution 1: Guidance on managing symptoms with opioids
We included more guidance within the new comfort care order set for nurses and clinicians using opioids for symptom management. We developed the opioid decision tree to assist in choosing a pathway and ordering an opioid within the electronic medical record, including whether to start a continuous opioid infusion (Fig. 1). The opioid decision tree is designed to teach clinicians appropriate opioid use in a complex and changing clinical environment that spans a number of different types of patients, units, and clinicians. It also provides guidance for managing patients whose symptoms remain uncontrolled, including consideration of a palliative care consultation.

Opioid decision tree for comfort care.
Within the order pathways, there is guidance on opioid choice, dosing, and route of administration. This includes an example calculation to determine the starting dose for an opioid continuous infusion. The Comfort Care Clinical Guide (Appendix 1; Supplementary Data are available online at www.liebertpub.com/jpm) contains more detailed information on opioids and other relevant topics for patients receiving comfort-focused care.
Solution 2: Titration algorithm
Our new comfort care titration algorithm emphasizes frequent IV opioid bolus dosing rather than rapid titration of opioid infusions to achieve adequate relief of uncontrolled pain and dyspnea (Fig. 2). The new algorithm allows IV opioid bolus doses to be given as needed every 15 minutes. If a few attempts at a bolus dose are inadequate, the bolus dose can be safely increased. Nurses may increase the opioid infusion rate every eight hours as needed using the new algorithm, which is much closer to steady state than the 30 minutes allowed in the original order set. More time in between titrations allows for more careful observation for opioid toxicity. With the new algorithms, the higher the dose of opioid, the smaller the percent increase in opioid infusion and the smaller the opioid bolus dose allowed. With these measures, we hope to limit cases of opioid toxicity, which is more common at higher doses and with morphine. 25
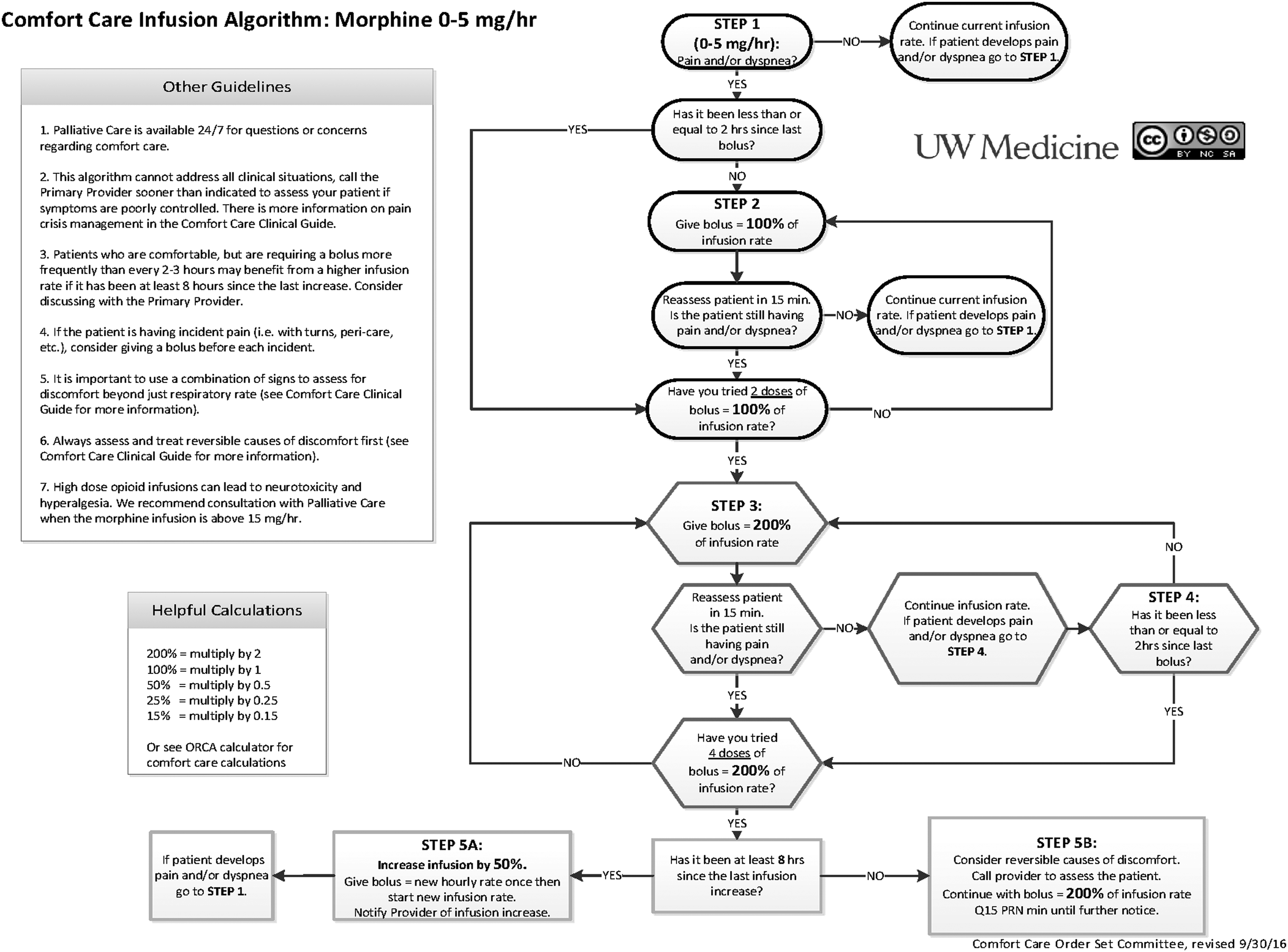
Comfort care infusion algorithm: morphine.
Solution 3: Collaboration
The opioid decision tree, comfort care opioid infusion algorithms, and order pathways within the electronic medical record include prompts for communication and palliative care consultation to improve collaboration between nurses, clinicians, and the Palliative Care Service (Figs. 1 and 2). There are also Comfort Care Provider and Nursing Checklists that encourage collaboration as well as education and resource provision to families (Appendices 2 and 3).
Discussion
There are documented gaps in the care provided at the end of life in hospitalized patients and a lack of evidence around end-of-life care pathways.3,8–10,17,23 Based on this and problems we encountered with pain and symptom management in patients receiving comfort-focused care at our hospitals, we formed an interdisciplinary group to evaluate and revise our original comfort care order set. We successfully developed and implemented a new comfort care order set at two hospitals. We based our new order set on clinical experience, opioid pharmacokinetics, feedback from colleagues, literature review, and consultation with national experts. We presented our order set nationally at the American Academy of Hospice and Palliative Medicine/Hospice and Palliative Nurses Association (AAHPM/HPNA) Annual Assembly in March 2016 and received evaluations from over 500 attendees, with much interest in this order set.
Other comfort care protocols have been published, but research on these protocols is limited.16,17,23,28–34 A 2016 Cochrane Review reported that there is a lack of strong evidence supporting the use of end-of-life care pathways. Nevertheless, the Cochrane Review concluded that the principles behind these pathways are still relevant and other sources have highlighted the importance of standardizing and streamlining orders for patients receiving comfort-focused care at the end of life.16,17,23
This report has a number of important limitations. First, we have not evaluated the impact of the new order set on drugs delivered to patients, patient comfort, or patient, family, or clinician satisfaction. Second, this development and implementation were conducted at two hospitals within a single healthcare system and in one region of the United States. Nonetheless, based on our experience presenting this process and order set at the American Academy of Hospice and Palliative Medicine, we believe our development process and resulting order set will be useful to other institutions. Further work is needed to evaluate the effectiveness and cost-effectiveness of such order sets.
With this new comfort care order set, we sought to provide more guidance to our clinicians on managing patients' symptoms with opioids, minimize instances of OIH, and improve collaboration between nurses, clinicians, and the Palliative Care Service. We offer our process and the resulting order set as an example for others to adapt and evaluate.
Footnotes
Acknowledgments
The authors would like to thank Mary Lynn McPherson, PharmD, BCPS, CPE, Janet Abrahm, MD, and Laura Mae Baldwin, MD, MPH.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.