
Abstract
Abstract
Background:
Pediatric fellows receive little palliative care (PC) education and have few opportunities to practice communication skills.
Objective:
In this pilot study, we assessed (1) the relative effectiveness of simulation-based versus didactic education, (2) communication skill retention, and (3) effect on PC consultation rates.
Design:
Thirty-five pediatric fellows in cardiology, critical care, hematology/oncology, and neonatology at two institutions enrolled: 17 in the intervention (simulation-based) group (single institution) and 18 in the control (didactic education) group (second institution). Intervention group participants participated in a two-day program over three months (three simulations and videotaped PC panel). Control group participants received written education designed to be similar in content and time.
Measurements:
(1) Self-assessment questionnaires were completed at baseline, post-intervention and three months; mean between-group differences for each outcome measure were assessed. (2) External reviewers rated simulation-group encounters on nine communication domains. Within-group changes over time were assessed. (3) The simulation-based site's PC consultations were compared in the six months pre- and post-intervention.
Results:
Compared to the control group, participants in the intervention group improved in self-efficacy (p = 0.003) and perceived adequacy of medical education (p < 0.001), but not knowledge (p = 0.20). Reviewers noted nonsustained improvement in four domains: relationship building (p = 0.01), opening discussion (p = 0.03), gathering information (p = 0.01), and communicating accurate information (p = 0.04). PC consultation rate increased 64%, an improvement when normalized to average daily census (p = 0.04).
Conclusions:
This simulation-based curriculum is an effective method for improving PC comfort, education, and consults. More frequent practice is likely needed to lead to sustained improvements in communication competence.
Introduction
O
Families, trainees, and program directors have recognized this gap.6–8,12,15,17,20–22 Yet, most pediatric fellowship programs lack formalized PC education; when education is provided, it is often lecture-based rather than experiential.17,20,21,23–26 Simulation-based training, successful in other high-stakes communication encounters,27,28 has the potential to change PC education in pediatrics.29,30 Similar to communication during resuscitation, communication around PC/end-of-life care is a discrete skill to be learned, practiced, and mastered. Prior PC simulation research has focused on adult clinicians,31–37 pediatric residents,26,38–40 and nurses of varying levels.41,42 Few studies have targeted pediatric fellows43–46 or followed longitudinally. 47
The goal of this study was to assess the relative effectiveness of simulation-based versus didactic training on pediatric fellow self-efficacy (comfort), knowledge, and satisfaction with PC medical education. For the simulation-based group, we assessed fellow communication competence including retention over time, and monitored referrals to a pediatric PC team. We hypothesized that fellows receiving simulation-based education, compared to fellows receiving didactic education, would perceive that they received better PC education, and demonstrate improved PC comfort, knowledge, and competence.
Methods
Study design
From August to November 2014, pediatric fellows enrolled at two sites: Stanford University (simulation-based site) and the University of Colorado (didactic site). Eligible fellows were first, second, or third-year fellows in Pediatric Cardiology, Critical Care, Hematology/Oncology, or Neonatal-Perinatal Medicine (Fig. 1). Recruitment occurred by e-mail invitation. Fellows signed consent for videotaping and were compensated (≤$25 gift card) for their participation. Both institutions have free-standing children's hospitals with similar patient volume and complexity, and similar size fellowships that lack a formal PC curriculum. Institutional Review Board approvals were waived at both institutions.

Fellows are first, second, or third-year fellows in Pediatric Critical Care, Cardiology, Hematology/Oncology, or Neonatal-Perinatal Medicine. aData used for analysis when full section completed (self-efficacy, adequacy of medical education, knowledge, barriers to palliative care).
Curriculum details
Fellows in the simulation group individually participated in a two-day, 4.5-hour curriculum consisting of (Fig. 2):
1. Three specialty-specific simulated scenarios with debriefing (by K.B and patient “mother”). Each involved children with life-threatening conditions, focusing on three themes of increasing complexity:
(a) introducing PC
(b) discussing goals of care including end-of-life and resuscitation preferences, and
(c) mediating disagreement between the family and medical team.
2. A 75-minute videotaped PC panel discussion delivered by PC faculty (H.C., B.S., J.G) and bereaved parents. Full curriculum and surveys available at MedEdPORTAL. 48

Study timeline for the simulation-based and didactic groups. Each simulation-based participant completed the entire schema above. Each simulation scenario was allotted 15 minutes with 30 minutes for debriefing. Didactic group fellows were able to complete education at a self-directed pace.
Two scenarios occurred on day one; the third was conducted three months later to assess retention. To ensure reproducibility, all scenarios utilized four learning goals, uniform room setup, similar family background information across specialties for each theme, one trained simulation specialist acting as the patient's mother, and a standardized debriefing guide. 48
Control group participants received didactic PC education via hyperlink and e-mail after finishing their baseline assessment, allowing curriculum completion over the study period duration. This was designed to be similar in content and time to the intervention group (one published article, four online videos, and six PowerPoint presentations) highlighting PC communication, family meetings, pain and symptom management, medical decision making, and values, benefits, and burdens of treatments.49–54 No fellows were prohibited from educational experiences that occurred throughout fellowship.
Fellow self-assessment data collection
Both groups completed self-assessments using the Pediatric Palliative Care Questionnaire (PPCQ) at baseline and day 90 (intervention group mean 90 days [standard deviation, SD 14 days], control group mean 101 days [SD 14 days]). 55 Intervention group fellows also completed the PPCQ after day one (Fig. 2).
The PPCQ has good test-retest reliability, internal consistency, and validity with subscales measuring: Self-Efficacy (comfort) with pediatric PC and communication, perceived adequacy of prior medical education in PC and symptom management, PC knowledge, and barriers to PC. 55 Self-efficacy questions were scored from 1 to 5 with five being the most comfortable (summary score range 23–115). 55 Adequacy of prior medical education questions were scored from 1 to 5 with five indicating more adequate training (summary score range 6–30). 55 Knowledge questions included seven multiple-choice and three true-false questions (score range 0–10). 55 Both groups completed post-intervention satisfaction questions (score range 1–5) with higher scores indicating greater satisfaction.
External reviewer evaluations of intervention group participants
Because physicians often self-report their competence inaccurately,56,57 external reviewers rated each subject using the Modified Kalamazoo Communication Assessment Tool (MKCAT), containing nine domains, each rated from 1 to 5 (poor–excellent). This tool has excellent reliability and validity.58,59 Scoring anchors were not previously provided, so anchors (e.g., behavior that constitutes a 3 vs. a 4) were devised and field tested with 11 multidisciplinary physicians, a PC psychologist, and two medical education experts until final approval. 48
Two reviewers experienced in performance ratings, psychosocial research and bioethics were recruited from the medical student body, and trained over four sessions, using frame-of-reference training; five videos were used, providing a range of physician-family encounters. Videos were randomly ordered, 60 and reviewers were blinded to the order. Utilizing a fully-crossed design (subset of participants rated by multiple raters), both reviewers then watched another 20% (10/51) of videos. 61 A goal inter-rater reliability, measured by the intra-class correlation coefficient (ICC), was set at ≥0.7 before dividing the remaining 70% of videos between the two reviewers (n = 18 each). 62 ICC was 0.72. Weighted kappa, assigning increased weight to values within one point (128/135 scores), was 0.70.
Palliative care consultation rate
New PC consultations, average daily census (ADC) and hospital admissions from the Divisions of Pediatric Cardiology, Critical Care, Hematology/Oncology/Stem Cell Transplant, and Neonatology at Lucile Packard Children's Hospital Stanford (simulation site) were tracked in the six months preintervention (02/2014–07/2014), study period (08/2014–11/2014), and six months post-intervention (12/2014–05/2015). Outpatient visit data were collected for the Divisions of Cardiology and Hematology/Oncology/Stem Cell Transplant.
Statistical analysis
The primary outcome was the difference in mean from baseline to three months for the Self-Efficacy Summary Score between the intervention and control groups. Secondary outcomes were the between-group difference in means over three months for the perceived Adequacy of Medical Education Summary Score and Knowledge Total score. Based on equal number of participants in the groups, power 0.8, alpha 0.05, SD 15, and true difference in means of 15, sample size estimation was 17 participants per group. 63
Descriptive statistics were used to estimate the frequencies, mean, and SD of the study variables. Between-group differences in baseline characteristics and outcome measures were assessed using Fisher's exact test for categorical variables, and two-sample t-test or Wilcoxon rank-sum test for continuous variables. The PPCQ five-point scale was converted to a binary variable with 4/5 being “comfortable” and 1/2/3 being “uncomfortable.” Multivariate logistic regression was used to determine whether the proportion of fellows moving from uncomfortable to comfortable changed over three months.
To assess within-group fellow communication competence, scores from the two blinded external reviewers were assessed for improvement and retention over time, initially with a repeated measures analysis of variance (ANOVA), and in post hoc analysis with paired t-test comparing performance in simulation #1 to simulations #2 and #3.
Difference in proportions z-score testing was used to compare the within-group proportions of PC consultations in the six months preintervention to post-intervention when normalized to ADC, hospital admissions, and outpatient visits. For all analyses, a two-tailed significance level was set at p < 0.05. Analyses were performed using SAS version 9.4, Enterprise Guide 6.1 (Cary, NC).
Results
Subject characteristics
Thirty-five eligible fellows enrolled: 17 fellows in the intervention (simulation-based) group, and 18 fellows in the control (didactic) group (Fig. 1). Demographic characteristics, prior PC education and experiences (Table 1), and baseline PPCQ Summary Scores were similar between the two groups (Table 2). Fellows had experienced similar types of education except for lecture-based education in residency (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/jpm).
One person in the didactic group did not self-report ethnicity. Percentage may not equal 100% due to rounding.
p significant at <0.05, obtained using Fisher's exact test (categorical variables) and two-sample t-test (continuous variables).
DNI, do not intubate; DNR, do not resuscitate; SD, standard deviation.
p significant at <0.05, by Wilcoxon rank-sum test.
Range 23–115 (p = 0.97 between groups at baseline).
Range 14–70 (14 a priori-designated questions which curriculum was focused upon).
Range 6–30 (p = 0.05 between groups at baseline).
Range 0–10 (p = 0.10 between groups at baseline).
Negative score reflects larger increase in didactic than simulation-based group.
Fellow self-assessment data
As assessed by the PPCQ Self-Efficacy Summary Score, over three months, the intervention group had improved self-efficacy (comfort) in pediatric PC compared to the control group (Δ between groups 10.3, p = 0.003) (Table 2, Fig. 3A, B, and Supplementary Table S2). Fellow comfort in the simulation group persisted at three months. Compared to the control group, more fellows in the intervention group rated themselves as “somewhat or very comfortable” with different PC tasks at the end of the intervention; this was notable for questions related to the simulation themes: (1) leading end-of-life discussions (increase of 53% vs. 9%, p = 0.002); (2) making a recommendation for no further cure-directed therapy (increase of 47% vs. decrease of 2%, p = 0.03), and (3) leading discussions where the family does not agree with the medical team (increase of 53% vs. 13%, p = 0.07) (Supplementary Table S3).
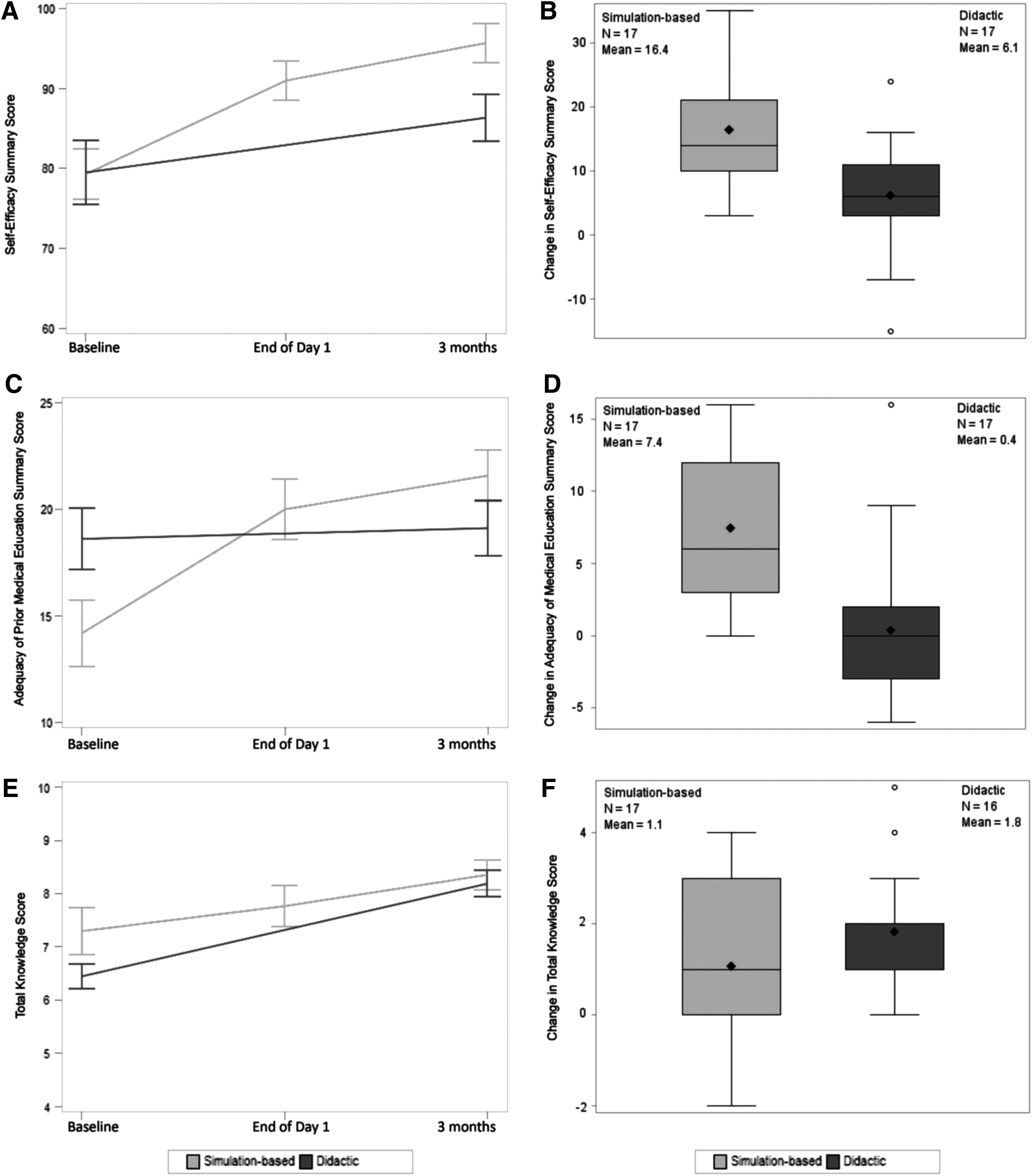
As assessed by the PPCQ Medical Education Summary Score, over three months, the intervention group felt they had received better PC training compared to the control group (Δ between groups 7.1, p < 0.001) (Table 2, Fig. 3C, D, and Supplementary Table S4).
Both groups PPCQ Knowledge test scores improved; there was no difference between groups (Δ between groups 0.7 favoring didactic group, p = 0.20) (Table 2 and Fig. 3E, F).
On a five point scale, the intervention group strongly agreed that the simulations felt realistic (4.5, SD 0.6), were similar to situations encountered in the hospital (4.8, SD 0.4), and enhanced their communication skills (4.8, SD 0.4). Despite a longer average time spent, intervention group participants more often felt that the time spent was appropriate (82% vs. 56%), valuing interactive time in simulation scenarios and debriefing. Only five control group fellows self-reported use of the educational videos and readings. Compared to controls, intervention group participants more strongly agreed that their PC education was useful (p = 0.02), would be used in clinical practice (p = 0.04), and recommended the education (p = 0.004) (Supplementary Table S5).
Palliative care communication competence
Repeated measures ANOVA (Table 3, pa) testing initially showed that fellows had improved communication competence scores over time. However, as plotting of individual results showed an initial rise in skills followed by some drop-off, post hoc analysis was undertaken assessing whether significance resulted from differences between simulation #1 and #2 (pb) or simulation #1 and #3 (pc). Intervention group fellows showed improvement over day one (pb) in four domains of the MKCAT58,59: relationship building (p = 0.01), opening the discussion (p = 0.03), gathering information (p = 0.01), and communicating accurate information (p = 0.04, paired t-test). However, these gains were not sustained over time (pc) (Table 3).
p significant at <0.05.
Repeated-measures ANOVA over three simulations (pa). Post hoc analysis using paired t-test showed significance was not a result of difference between simulation #1 and simulation #3 (pc), but rather between simulation #1 and simulation #2 (pb).
ANOVA, analysis of variance.
Palliative care consultation rates
At the simulation-based institution, PC consultations increased 64% from the divisions of Pediatric Cardiology, Critical Care, Hematology/Oncology/Stem Cell Transplant, and Neonatology in the six months post-intervention (n = 41) compared to the six months preintervention (n = 25). The post-intervention proportion of consultations was higher when normalized to the ADC (43.2% vs. 28.4%, p = 0.04) or clinic visits (0.4% vs. 0.2%, p = 0.009), but not when normalized to inpatient admissions (2.7% vs. 1.8%, p = 0.11).
Discussion
In this two-site prospective study, simulation-based training resulted in sustained improvement in fellow comfort and perceived adequacy of PC education, was more highly rated than didactic education, and may correlate with increased utilization of specialty PC services. While external reviewers saw short-term improvement in some communication skills, these were not sustained over three months.
This simulation-based PC communication study is the first prospective, longitudinal, multispecialty, multi-institution trial comparing simulation-based education to didactic education for learning PC communication skills. Previous simulation-based communication studies mostly focused on delivery of information, for example, “breaking bad news,” rather than complex goals of care discussions,39,64 and measured self-efficacy after one day, providing little data about a fellow's development. A study that assessed fellows over 6–12 months lacked a control group, 47 and thus, it remained unknown whether the improvement seen was due to usual training experiences or the educational intervention. This study builds upon prior authors' work and recommendations by utilizing a control group to monitor the baseline change in skills acquired through fellowship training, and external reviewer assessments to provide a proxy for family perception of fellow performance. 57
Excellent communication is the central tenet of providing high quality shared decision making, symptom management, and PC concordant with family values. As the complexity of pediatric care grows, quality interactions with HCPs become more important in a child's healthcare journey.4,8 Yet, many pediatricians and subspecialists are uncomfortable with incorporating PC communication skills throughout a child's disease course.12,14,15,17,20 While sub-specialty PC teams can be beneficial in this regard, there are too few teams on which to rely.2,6 Therefore, improving the quality of PC communication by all clinicians is a priority.2,6,7
Several features make this program unique. The published curriculum and questionnaire make this easily reproducible.48,55 Consistent with other studies, trainees preferred experiential learning, 39 and felt more comfortable after the intervention. However, control group data indicate that comfort also improves through usual training coupled with didactic education. Therefore, the interval improvement of the intervention group over the control group reflects the effect of the simulation-based training over a commonly used medical education training model.
This study was designed to underestimate results in several ways. Without the ability to reflect on what was learned, fellows' self-reported baseline scores may be higher than their true skill level. This response shift bias underestimates program effect, and could be reduced by using a retrospective pretest design where participants assess both their pre- and post-intervention self-efficacy at the same time, improving overall accuracy.65,66 Despite improvement, some fellows report a maximum comfort lower than “5” due to the difficulty of the content; self-reporting proficiency or competence may allow for greater score variability. In practice, simulation programs would generally have fellows participate in groups, watch other fellows' performances, and debrief as a group, which would maximize skill acquisition. 45 Lastly, increasing the complexity of the scenarios is designed to build skills incrementally, but reviewers are less likely to rate simulation #3 as being significantly better than simulation #1.
Study limitations
There are several limitations to this study. Factors limiting recruitment included the small size of pediatric fellowships and lack of protected time. Participants likely had a greater interest in PC communication than nonparticipants, leading to selection bias. Although there may be institutional confounders (PC culture, diversity of residency training, patient demographics and complexity) that limit comparability across institutions, there were minimal differences in demographic, educational variables, baseline PPCQ scores, and factors influencing participation.
Despite making didactic education readily accessible, only five control group fellows fully used the material provided during the study period, limiting analysis across groups. Didactic training is expected to improve content knowledge more than skill-based competencies; thus, it is unsurprising that there was no difference in the knowledge outcome. The low didactic group participation rate reflects the practical difficulty of relying on self-directed didactic education during busy training years. It may be more appropriate to interpret results as a comparison of simulation-based education to the current fellowship training curriculum.
External reviewers generally felt that fellows had improved over the study time. However, their scores did not confirm a sustained increase in communication competence analogous to the increase in comfort that fellows' perceived. Lack of statistical improvement could be secondary to: lack of power for this outcome, a change in the validity of the MKCAT after adding scoring anchors that often clustered scores in the 3–4 range, short simulation time limiting fellow ability to score highly on all communication domains, and the increased difficulty of simulation #3 as compared to #1. While a different scoring scale or utilizing parents of seriously ill children could yield different results, the potential for psychological distress due to the highly emotional nature of the scenarios made this unfeasible for our parent groups.
PC consultation rate was obtained only from the four departments from which fellows participated at the simulation-based site. Consultation numbers do not include complex care, gastroenterology, genetics/metabolism, nephrology, neurology, and pulmonology. The change in consultation rate could be secondary to increased recognition of the broad PC services available, and dissemination to other team members, but correlation does not imply causation. While no other institutional interventions occurred to account for this change, the direct participation of a fellow in a decision for consultation cannot be measured. PC consultation data were not available from the control site; it is unknown whether PC consultations would have changed in a similar fashion.
Future directions
As this is pilot work, further refinement is necessary in self-reported and external measurement tools targeting pediatric patients and parents. In building a curriculum, scenario complexity can be increased by modifying the disease, participants, cultural, language, psychosocial variables, and using mixed modalities (live parent and patient mannequin). Future trials could study small educational fractions provided at more frequent intervals to assess skill retention, or evaluate patient and parent-reported outcomes (perception of fellow communication skills, rates of anxiety or depression, and frequency or timing of goals of care discussions). Finding ways to make the education less costly and more efficient will be key to its continued use. Once a curriculum leads to sustained improvements by self- and external-rating, it could be more widely disseminated through online platforms or national programs.
Conclusions
Acquisition of the cognitive and communication skills necessary to competently and compassionately deliver PC has historically been thought to occur via clinical exposure. Pediatric studies indicate that this assumption is incorrect. On-the-job experience is limited and variable in quality, leading to suboptimal communication, and unnecessary physical, psychosocial, and spiritual suffering. Despite limitations of simulation education including its lack of focus on knowledge and the need for more frequent sessions to attain better retention, this simulation-based curriculum is one method for learning PC communication skills. In addition, this training is easily adapted and scaled in complexity, thereby creating challenging and valuable learning experiences for senior trainees and experienced physicians alike.
Footnotes
Acknowledgments
The authors wish to thank Nancy Contro, LCSW, and the parents from the Lucile Packard Children's Hospital Stanford Palliative Care—Family Partners group for their involvement in the education component of the video, the Center for Advanced Pediatric and Perinatal Education (CAPE) staff (Julie Arafeh, Barb Beebe, and Alba Rivera) for simulation time and expertise, Vyjeyanthi (VJ) Periyakoil, MD, for palliative care mentorship, Kiruthiga Nandagopal, PhD, and Sylvia Bereknyei, PhD for medical education mentorship, Alice Whittemore, PhD and Rita Popat, PhD for statistical mentorship, Brian Greffe MD, Joanne Hilden, MD, Thomas Parker, MD, Brian Jackson, MD, and Austine Siomos, MD at the Children's Hospital Colorado, University of Colorado for assistance with recruitment, and Jenna Braverman and Jason Batten for providing external reviews to each video, for which they were compensated. This work was supported by (1) the Child Health Research Institute, Lucile Packard Foundation for Children's Health Innovations in Patient Care Grant, Stanford CTSA (UL1 RR025744/UL1 TR001085) awarded to K. Brock, which provided salary support for authors H.C., B.S., J.G., and L.P., payment for external reviewers, simulation lab support, study subject reimbursements, RedCap utilization, and video editing; (2) the KL2 component of the Stanford Clinical and Translational Science Award to Spectrum (NIH KL2 TR 001083) that provided salary, tuition, and travel stipend support to K. Brock; (3) the Rathmann Family Foundation Educators-4-CARE (E4C) Medical Education Fellowship in Patient-Centered Care through the Stanford University School of Medicine—Office of Medical Education, in conjunction with the Stanford Center for Medical Education Research and Innovation, which provided salary, technological and travel support to K. Brock, and (4) the Endowment for the CAPE, which supports the simulation lab and personnel.
Author Disclosure Statement
The other authors have indicated they have no potential conflicts of interest to disclose and have no relevant corporate sponsors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.