
Abstract
Abstract
Background:
Investigating complaints concerning end-of-life (EoL) care is a necessary step for improving the quality of life at its final stage.
Objective:
We aimed to classify and quantify the aspects of EoL care that require improvement by analyzing caregivers' feedback on the care their relatives received before death.
Design:
A survey of primary family caregivers of deceased patients.
Setting/Subjects:
Relatives of decedents were recruited through two geriatric medical centers and from persons contacted for other studies, who reported losing a relative. Face-to-face interviews of 70 relatives of the deceased were conducted. The participants' mean age was 64, 68.6% were female, and most (57%) were born in Israel. Regarding relationship to the deceased, 74.3% were sons/daughters, 24.3% were spouses, and one (1.4%) was a cousin.
Measures:
Responses to the question “Is there something in the health system or the behavior of the doctors/nurses that you would recommend changing?” were analyzed qualitatively.
Results:
82.9% of participants had complaints about the care received. Within this, 62.9% related to provision of services, 51.4% to communication, 27.1% to system issues, 15.7% to institutional issues, and 10.0% to staffing issues. Qualitative analysis revealed potential causal relationships between these EoL issues. We therefore propose a theoretical model involving the distal factors of system, institution, and staff that impact the proximal factors of provision of services and communication.
Conclusion:
The new model has the potential to clarify directions in research, quality assessment, and intervention regarding end-of-life care.
Introduction
W
Past studies mainly focused on assessing and classifying the qualitative needs concerning professional EoL care. One review 4 stated that the needs of patients and family members concerning palliative and EoL care can be grouped into eight key domains of satisfaction with the care system, namely accessibility, coordination, competence, communication and relationships, education, emotional support, personalization of care, and support of patients' decision making.
Only a few articles have investigated EoL care needs extending beyond professional care, as for example by asking relatives about their experience of caring for a relative at EoL.3,5,6 In addition, although the qualitative aspects of EoL care have been assessed and categorized thematically, to our knowledge, there have been no studies to date that have quantified the prevalence of various EoL issues. This would therefore seem important for identifying the most pressing issues and informing effective intervention and policy change.
The objective of this study was to investigate complaints concerning EoL care, as reported by relatives of the deceased, categorize the feedback, and describe the issues encountered quantitatively. We hypothesized that we would obtain responses pertaining to the eight domains described in the review of Dy et al. 4 However, since their review included only measures of satisfaction, whereas our data pertained to complaints, we anticipated differences in the types of responses. Given the lack of previous quantitative analysis of EoL issues, it is difficult to predict which issues would be most prevalent. Yet, since a large bulk of EoL literature focused on care directives 7 and expectation setting at EoL, 1 we predicted that our quantitative analysis would reflect these among the pertinent issues in EoL care.
Methods
Participants
We interviewed 70 relatives of deceased persons (52 children, 17 spouses, and 1 cousin). Interviews were conducted from a few weeks to a few years after death (mean = 16.20 months; standard deviation = 13.07). Background information on the interviewees and their deceased relatives is shown in Table 1.
SD, standard deviation.
Procedure
The research was approved by the ethical committee of Tel Aviv University and the Helsinki committee of the Rabin medical center. Relatives of decedents who died in geriatric medical centers and persons from other studies who reported losing a relative were contacted (Fig. 1). Upon contacting the relatives, we described our research and the process of the interviews and requested their consent to participate in the research. Face-to-face interviews were conducted by trained interviewers at locations convenient to participants (e.g., home, coffee shop, and university). Interviews were structured focusing on the stages of EoL experienced by the deceased. The analysis presented in this study is based on narrative responses to the open-ended question:
Is there something in the health system or the behavior of the doctors/nurses that you would recommend changing?

Recruitment sources.
Analytic method
In the first stage of analysis, two researchers (J.C.M. and R.C.) independently categorized all qualitative responses into types of complaints. Every issue raised in an interviewee's answer was treated separately, such that each answer could represent more than one complaint response. The authors then attempted to code the responses based on eight domain classifications outlined in a 2008 EoL review article by Dy et al. 4 Due to the unsuitability of certain categories and overlap among others, the authors decided to reclassify the responses, clustering them into unifying thematic categories, each with specific dimensions and subcategories. The independent coding of each response by the two researchers was then compared and discrepancies discussed and resolved. A quantitative analysis of response frequencies within each subcategory was performed to determine prevalence of concerns relating to EoL care.
Results
Qualitative analysis: Nomenclature and model development
While attempting to develop a nomenclature that fit the data, the authors observed that there were seemingly causal relationships between some of the responses, which were not captured by existing classification systems. In analyzing the response types, we found that most complaints fell into one of two broad thematic categories: “provision of service” and “communication.” Responses within these two categories were defined as proximal in that, they were discrete complaints that directly affected the patient's or family's day-to-day lives during the EoL period. In addition, three “distal” thematic categories were identified: “system,” “institution,” and “staff.” These included ongoing and systemic issues perceived to influence the proximal categories (see Table 2).
Provision of service
“Provision of service” included all medical, nursing, and custodial interventions, subdivided into dimensions of quantity and quality. Quantity included responses that reported necessary treatments that were unavailable to the patient, services that were available, but were only partially provided to the patient, and cases of overtreatment. For example,
It is more important to pay attention to things like replacing diapers every four hours. We are talking about humans. The nurse should make another round in between. A person can have a bowel movement an hour after the nurses' round, so he has to wait three hours.
The dimension of quality included responses pertaining to treatments that were performed at an inferior level or in a manner not respectful of the patient's values or lifestyle. For example,
Hospitals A and B were not good. He got bedsores, and was sent home with a fever because they said there was nothing to do for it. So he was at home for two weeks with fever and I saw that he was really not a person anymore, he was nothing. The nurse sent him immediately to the B hospital, and they did not heal his bedsores.
Communication
The category of communication was subdivided into quality, quantity, and scope. Quantity of communication described issues relating to the frequency with which staff communicated with patients and family. For example,
I would like the staff to talk more with the family, invest time and volunteer information. Often you find yourself feeling uncertainty. I would like to know more details, what to do…
Quality of communication dealt with the manner in which staff interacted with patients and family, including showing respect and compassion for the patient. For example,
The doctors… were really impatient. Once I said to the doctor that the breathing tube that they stuck in his throat could damage him. He laughed to my face, “Do you think that your father will ever wake up?”
Scope of communication outlined the range of topics covered by staff communication and whether this matched the patient's or family's needs.
System
Responses in the “system” category included complaints regarding health coverage, governmental funding, justice (issues of unfair or illegal conduct within the health system), and navigation of healthcare. Interestingly, to date, the subcategory of justice has been absent from quality of EoL literature. The following excerpt provides an example of the justice category:
…we understand that he did not treat her [the patient] properly. He behaved arrogantly toward us and toward her. In retrospect, we realize that he wanted us to give him money on the side for him to take care of her properly. But at the time we did not know that was what he wanted.
Institution
The category of institution includes responses pertaining to the general management of medical facilities, such as ongoing complaints about poor environmental conditions or lack of coordination among the health team. For example:
The bottom line is that it is a place where it is difficult to be. You open the door and the smell and the views you see there are very difficult.
Staff
This general category includes training of staff, staff competence, and staff burnout. For example:
…There was no compassion there. They would take them, put them, like a sack. Screaming from all directions…There was no communication among the different staff members. It was completely crazy
Proximal and distal responses
We found that responses often pointed to causal relationships between complaints. These could not be accurately portrayed by previous categorizations in the literature. We therefore included the concepts of proximal or distal factors, thereby adding a level of complexity in understanding EoL care. The following excerpt provides an example of this causal relationship:
There were times of understaffing and stress on the unit. For example, when persons need their diapers changed, these people cannot say what is bothering them because they are unconscious, and I could come and find my father dirty.… I do not blame the staff, but one has to increase staffing. …Staff members seem to burnout and they too need support.
This relative is upset about insufficient or untimely toileting care, which falls into the category of quantity of service. However, she is able to identify potential underlying causes, namely understaffing and the resultant staff burnout.
Limitations in categorizing responses
In classifying relatives' narrative responses into discrete categories, we came across a number of complexities that highlight components missing from both our proposed nomenclature and the EoL care literature. First is the complex interrelationships between praises and complaints; second, the emotional valence of many of the interview answers is lost once they are broken down into discrete responses; and finally, the subjectivity of complaint data raises the potential for bias in coding the responses. These are illustrated below.
Interrelationships between complaints and praise
In X acute hospital, they did not talk with us at all. And toward the end, they talked, but did not provide us with all the options. They said, you know that he is in a grave state, so, yes, I know, but what are the options to help him? That, they did not provide. So what if he is an older person? The dialysis department did help us to reach decisions in a simple and comfortable manner…
As demonstrated, praise was sometimes included to illustrate a complaint and validate it. The quantitative categorization of complaints cannot include these complex interrelationships. We do not report the results regarding praise because we asked about complaints, and so the reports of praise likely do not represent the sample's appraisal of the positive aspects of care.
Emotional valence of responses
The classification system does not allow for the expression of the intensity and emotional quality–anguish, despair, and helplessness–of the complaints. This is an integral element in understanding the pitfalls in EoL care and is demonstrated below:
From the doctors who do not exist, to the disgusting nurses and the nurses' aides who are cruel beyond anything I have ever seen. Really cruel. I would change everything, I would replaces the doctors, all the staff!
Potential limitations with using complaint data
His family doctor did not force him to undergo an endoscopy examination which he had skipped because he did not want to do it, though he was at risk…. I did not attack her to her face but I think she is guilty.
In this situation, the complaint is highly subjective, as one could argue that the deceased had the right to refrain from undergoing a procedure. Accordingly, the authors remained cognizant of this potential for bias, not always taking such complaints at face value.
Quantitative analysis
When asked whether there was anything they would like to change in the healthcare system, 67.1% responded in the affirmative. Both these respondents, as well as those who responded in the negative, proceeded to elaborate on what they would like to change. In the verbal responses, 82.9% of the interviewees reported problems with quality of care.
Complaint responses
The issues raised involved different aspects of dissatisfaction with the healthcare system. With 62.9% of all participants reporting dissatisfaction related to provision of services, 51.4% to communication, 27.1% to system issues, 15.7% to institution, and 10.0% to staffing (see Table 2). The most commonly endorsed subcategories were as follows: not providing needed services (27.1%), lack of compassion (22.9%), staff not focusing on the patient (21.4%), staff not manifesting respect and dignity (20.0%), insufficient health insurance coverage (18.6%), health services unavailable (18.6%), lack of information regarding prognosis (12.9%), and lack of justice (11.4%). Two specific issues relating to quality of service were repeated by multiple responders, namely those pertaining to lack of cleanliness (including smells) and the development of pressure sores.
Discussion
Of the interviewees, 82.9% reported problems with quality of care. These quantitative results reveal a disturbing picture of EoL care, where patients frequently encountered a lack of services, neglect, and staff who did not treat them as a whole person and who lacked compassion and respect. By quantifying the frequencies of complaints, this study is unique in its approach to classifying EoL care. By creating a hierarchy within EoL care issues, this approach allows for the identification of not only broad categories that require change but also areas that require the most urgent attention. In this way, our results are unequivocal in that, the areas of EoL care that require the most urgent intervention are lack of services and lack or poor quality of communication. More specifically, the issues that were most pertinent included lack of needed services, staff members' lack of compassion, lack of respect to patients, insufficient health insurance coverage, and staff unavailability. These findings are corroborated by research documenting high levels of suffering at the EoL in Israel. 8
Our findings add to prior classification systems in that, within the model, healthcare concerns are divided into proximal and distal complaints. The proximal complaints represent acute problems encountered directly by the patients. The distal complaints were generally the root causes of the proximal complaints. We therefore suggest a new framework that takes these factors into consideration as represented in Figure 2. This differentiation allows for a more targeted approach, suggesting that policy change should focus more on the distal root issues, whereas interventions in care facilities would be better suited to target proximal concerns.
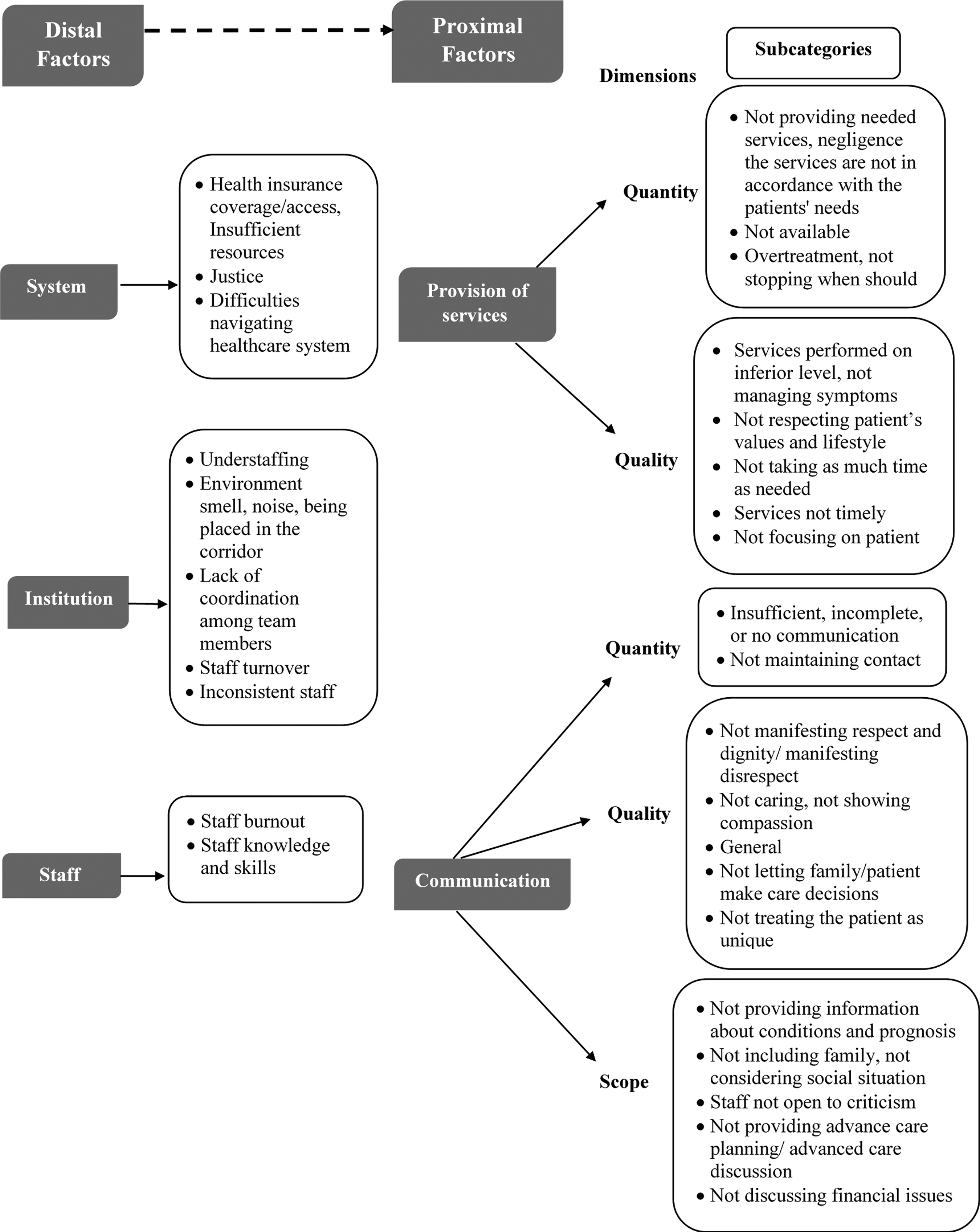
A nomenclature for classifying quality of care: distal factor impacting proximal factors and their dimensions.
The analysis revealed a domain not identified in past EoL care research, related to “justice,” which includes several types of complaints: patients receiving different quality of treatment based on connections or money, conflicts between staff and patient values, and systemic corruption (e.g., a conflict between physicians' private practice and work in a public hospital). The question arises as to why this issue surfaced in the Israeli sample and not elsewhere. We can only speculate that culture-specific attitudes, such as expectation of equality in care, might represent possible influences.
Existing literature focuses on improved advanced care planning as a central issue for improving EoL care. 7 Our results are somewhat at odds with this approach. Only 1.4% of our participants complained regarding advanced care planning, the least common category.
Our results, rather, suggest that our proposed framework for classifying quality of care at EoL better reflects the perceptions of caregivers than do prior classifications. The deficits in quality of care pertain mainly to inferior treatment and problematic attitude/communication. In reorganizing the EoL classification system in a more streamlined manner, our model draws attention to the most prominent deficits within the EoL care system, thereby allowing healthcare professionals to better identify the areas that require improvement. Similarly, we believe that framing the classification in the negative, as opposed to the positive, allows for more effective detection of the matters that most urgently require change.
Despite the outlined advantages of our proposed model, some considerations and clarifications remain. The most important is the question of cause and effect: to what extent are the distal factors actually causing the proximal ones, such as understaffing resulting in poor care? These causal relationships are crucial in terms of planning interventions to improve quality of care. A further issue that needs to be examined is the degree to which different types of facilities, such as acute hospital, long-term geriatric hospital, nursing home, or home care, are associated with different types of problems in terms of quality of care during EoL.
Use of qualitative data as the basis for our analysis elicited some complexities, such as with coding and classification of the data into discrete categories. For example, when a complaint involved the quality of care provided, it could also be coded under the distal category of staff. We tried to code the complaint based on what it primarily addressed, which itself was not always clear. Therefore, decisions regarding ambiguous responses may have affected category frequencies. We suggest adding a scale to our model, which would allow for report of emotional valence as a factor in the complaint data.
The results paint a disturbing picture of EoL care. It is acknowledged that the sample was not a random sample of the population and thus not a representative sample of all EoL experiences in Israel. This is important in that, many of the complaints were setting specific. The wording of the question analyzed requested complaint data, yet since this question was part of a larger questionnaire investigating the stages of EoL, the respondents likely did not participate in the study specifically for an opportunity to complain. A study of a more representative sample is recommended, investigating complaints as well as praise concerning EoL care, and designed in line with findings of this study.
The question of what needs to be done to improve the quality of care at EoL emerges from the study findings. Yet the results can only point to partial answers. One component of the answer appears to involve distal systemic root causes, which include institutional structure, staff management, and resources that are currently not provided by the care system. However, proximal issues of standards of care as well as attitudes and communication need to be addressed simultaneously.
Footnotes
Acknowledgments
This study was supported by the Minerva-Stuftung Foundation.
Author Disclosure Statement
No competing financial interests exist.