
Abstract
Abstract
Background:
The increasing number of children with life-threatening and life-limiting conditions requires an individualized approach and additional supportive care in hospitals. However, these patients' characteristics and their prevalence in a pediatric tertiary hospital setting have not been systematically analyzed.
Objective:
This study aimed to determine the proportion of hospitalized children who are receiving care for life-threatening diseases with feasible curative treatments and for life-limiting diseases (LLDs) with inevitable premature death as opposed to care for acute or chronic diseases; additionally, it sought to compare patient characteristics, clinical features, and symptoms within these subgroups.
Design/Setting/Subjects:
A cross-sectional survey of 208 patients was conducted at a large tertiary pediatric care center through standardized interviews with the responsible medical teams. Patient subgroups were defined as those with acute, chronic, life-threatening, or LLDs.
Results:
The comparisons of patient subgroups showed distinct differences and revealed that nearly half of all inpatients suffer from life-threatening (20%) or LLDs (27%), with a high proportion of rare diseases (82%). They experienced a high burden of symptoms in all parameters of clinical features, including high demand for medications and nursing care.
Conclusion:
A substantial proportion of pediatric inpatients suffered from life-threatening or LLDs, as well as rare diseases, indicating a high burden of symptoms and a high need for additional care. The results suggest a substantial need to implement pediatric palliative care structures in tertiary care centers for patients in critical and terminal conditions.
Introduction
I
Similarly, the number of children and adolescents (hereafter “children”) with life-threatening diseases (LTDs) and life-limiting diseases (LLDs) has also risen. 3 This increase has been attributed more to the higher survival rates of patients with LTD/LLD than to a rising incidence of LTD/LLD. 3 The estimated prevalence of LTD/LLD in children ranges from 18.54 to 32 per 10,000. 3 The prevalence of LTD/LLD in children younger than one year is even higher, at an estimated 127.3 per 10,000. 5 Children with LTD/LLD mainly suffer from congenital, oncological, or neurological disorders.5,6 The proportion of rare diseases, defined as those not affecting more than five per 10,000, is high within this group. 7 The clinical conditions of children with LTD/LLD are complex.6,8 They lead to regular hospitalizations and require an individualized approach that is often delivered by a multidisciplinary and multiprofessional team. 9 It is claimed that supportive and palliative care should be integrated early in this approach to meet patients' needs for additional care, such as special nursing techniques, pain therapy, physiotherapeutic and psychological approaches, as well as to provide support for the affected families.10,11 Detecting children in the hospital setting who are in need of additional palliative care is crucial for better quality of life and parental adjustment. 12 However, the characteristics and their actual prevalence among children with LTD/LLD in a pediatric tertiary hospital setting have not been systematically analyzed.5,13
The aim of this cross-sectional study was to quantify the group of patients with LTD/LLD who are in need of palliative care in a pediatric tertiary care university center and to gain a better understanding of their characteristics and specific care needs by evaluating their clinical features and symptoms and comparing them to other inpatients.
Methods
Study design, setting, and study population
Between March 2013 and April 2013, a cross-sectional survey was conducted in the Children's University Hospital of the Charité Universitätsmedizin Berlin, Germany, which is a public tertiary care center. With a capacity of 312 beds, this hospital is one of the largest university pediatric medical institutions in Europe, hosting nine specialized pediatric departments, including all pediatric subspecialties except for the surgical subspecialty of cardiac surgery. The hospital also provides pediatric palliative care (PPC). Data were collected over a period of eight days, in which each department was surveyed on one particular day.
On these particular days of data collection, 224 of the 312 hospital beds were occupied. Fifteen individuals were older than 18 years, and one patient died on the day the study was conducted. The remaining 208 patients were aged between 0 and 18 years and represent our study group. Patients were only counted once, regardless of their possible transfer to other wards during the survey. This study received approval from the Ethics Commission of Charité Universitätsmedizin Berlin in November 2012 (application No. EA2/054/12) and adhered to the Declaration of Helsinki (Version 1996, Somerset West).
Data source and survey process
Interviewers (n = 7) received prior interview training and gathered data by conducting standardized interviews with the physicians and nurses in charge of the respective patients. Standardized definitions for every term used in the interview were available for the interviewers and interviewees at any time. Questions were coded either as yes–no for close-ended questions or as a list of answer choices on a 4-point Likert scale. Interviewers simultaneously entered the obtained data into a web-based survey tool (SurveyMonkey™) created for this study.
Each interview consisted of two domains. The first domain was a query of clinical data. Physicians provided information concerning sedation, level of alertness, and, in patients with LLDs, life expectancy. Nurses provided information on permanent medical devices and level of nursing care. In the second domain, detailed information on ∼29 current symptoms such as the frequency, intensity, and burden of symptoms was gathered from the medical team in charge of the respective patients.
In addition, relevant data were extracted from the patients' files and entered into the survey tool. The data extracted from patient files included gender, age, length of stay in the hospital, and daily scheduled medication.
All data were then downloaded and compiled into a master database. Eight weeks after the survey, each patient's discharge diagnoses were added to the master database as International Classification of Diseases, 10th revision (ICD-10), diagnostic codes. 14 To differentiate patients' clinical conditions, subgroups were generated based on existing classification tools such as the ICD-10 and A Guide to the Development of Children's Palliative Care Services.9,15 The underlying diagnosis of every patient was assessed based on ICD-10 diagnostic codes in addition to the diagnoses that triggered the patient's original admission to the hospital. Each diagnosis was assessed to determine whether it belonged to the category of rare diseases. 16 Finally, to reflect the presence of life-limiting conditions in children, the ICD-10 diagnostic codes in this study were compared with a directory of ICD-10 codes for children suffering from LTD/LLD developed by Hain et al. (hereafter “Hain's ICD-10 Directory”).17,18
Subgroups and interview guide
Before the interviews, the attending pediatricians were asked to assess and classify the patients' underlying condition as either an acute disease (AD), CD, LTD, or LLD, thereby establishing a primary stratification tool to generate subgroups. Based on the ICD-10 and the underlying conditions, a reassessment performed by an expert in PPC led to a validated classification of the diseases. When the pediatrician and PPC expert provided different allocations, a second external expert in PPC was consulted. Consensus was established through discussion between the two PPC experts. For definitions of the subgroups, see Table 1.19–21 Because our focus was on children with palliative care needs, we combined the subgroups AD and CD and compared this merged group with children suffering from LTD or LLD.
AD, acute disease; CD, chronic disease; LLD, life-limiting disease; LTD, life-threatening disease.
Statistical analysis
Analysis was performed using IBM SPSS Statistics, version 22.0 (IBM Corp., Armonk, NY) 22 and R Core Team 2014. 23 Descriptive statistics was generated using proportions, median (MDN), and interquartile range (IQR) as appropriate. As the data did not show a normal distribution, nonparametric tests such as Fisher's exact test, Kruskal test, and pairwise Wilcoxon test were applied to compare the characteristics of the stratified subgroups. The alpha level was set at 5%, meaning differences with a p-value ≤0.05 were considered significant.
Results
The final study sample comprised 208 inpatients. The patient characteristics are shown in Tables 2 and 3. Physician data and assessments were missing for 11/208 patients. In general, there was good agreement between the assessment of the physician in charge and of the PPC expert regarding the assignment of the children to the four groups (AD, CD, LTD, and LLD) (Cohen's kappa coefficient, κ = 0.76 [0.69/0.83]). In 35/197 patients, the responsible physicians' assessment of the patient's disease differed from that of the PPC expert. For these 35 patients, allocation was applied according to the experts' agreement (Fig. 1). The highest rate of mismatch was observed for the LTD group. The final subgroup sizes of children with AD/CD and LTD/LLD were 110/208 (53%) and 98/208 (47%), respectively.
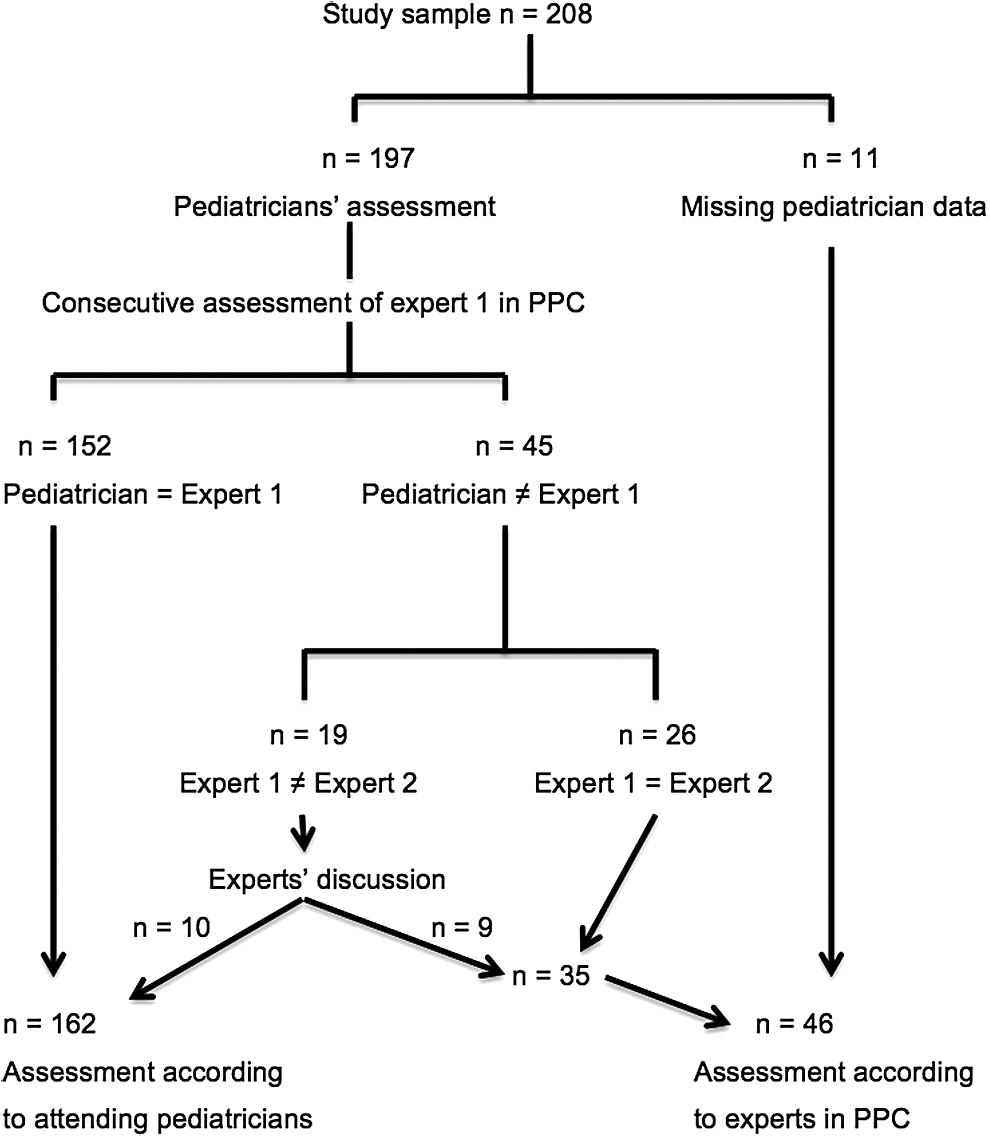
Overview of subgroup establishment. Primary stratification: Attending pediatricians' assessment of patients' conditions (AD, CD, LTD, or LLD). Validation of diseases' classification: Reassessment by an expert in PPC. When different allocations: Consultation of a second external expert in PPC and consensus through discussion between the two PPC experts. AD, acute disease; CD, chronic disease; LLD, life-limiting disease; LTD, life-threatening disease; PPC, pediatric palliative care.
Statistics: Fisher's exact test for categorical data or Kruskal test for quantitative data.
n = 1 missing.
ICD-10, International Classification of Diseases, 10th revision; IQR, interquartile range; MDN, median.
Statistics: Fisher's exact test for categorical data or Kruskal test for quantitative data.
n = 11 missing.
n = 1 missing.
n = 2 missing.
CVC, central venous lines, includes also Broviac-, Hickman-, or port catheter; PEG, percutaneous endoscopic gastrostomy.
Comparing Hain's ICD-10 Directory17,18 with ICD-10 codes for LTD/LLD revealed agreement in 71/98 patients (73%; κ = 0.63 [0.53/0.74]). The ICD-10 codes of 21 patients with LTD and 6 patients with LLD did not correspond with any of the ICD-10 codes in Hain's ICD-10 Directory (Table 2). In patients with LTD, the most common noncorresponding ICD-10 codes were anorexia nervosa, prematurity, and status after cerebral hemorrhage. The ICD-10 codes that did not correspond in children with LLD were status after liver or kidney transplantation, severe crisis of sickle cell disease, cytomegalovirus encephalitis, focal segmental glomerulosclerosis, and a severe case of a patient with Trisomy 21.
Comparison of children with LTD/LLD to those with AD/CD
In children with LTD/LLD, the most frequent underlying diseases were malignant neoplasms (19%), genetic/congenital disorders (16%), and neurological/neuromuscular disorders (15%, Fig. 2). The clinical features and symptoms of children suffering from LTD (41/208, 20%) or LLD (57/208, 27%) differed significantly from those of inpatients suffering from AD (50/208, 24%) or CD (60/208, 29%). Patients with LTD/LLD were significantly older than those with AD/CD and showed a significantly higher rate of rare diseases. Specifically, 80/98 patients with LTD/LLD suffered from rare diseases (82%; p < 0.001, Table 2). During their hospital stay, patients with LTD/LLD received significantly more daily scheduled medications (including infusions, Table 3). They required significantly more antibiotics, diuretics, antacids/PPI, anticoagulants, antihypertensive drugs, and glucocorticoids (p < 0.001). Significantly more children with LTD/LLD had permanent medical devices such as a central venous line (Table 3). Nurses reported a significantly higher level of care for patients with LTD/LLD compared to patients with AD/CD (Table 3). Children with LTD/LLD showed a significantly higher median number of symptoms (p < 0.001, Table 3), and the frequency, intensity, and burden of symptoms were almost always higher in these children (Fig. 3). Fatigue, poor appetite, depression, and concentration difficulties were significantly overrepresented in children with LTD/LLD (Fig. 3). Finally, children with LTD/LLD showed a high or very high burden from anxiety, pain, and agitation.

Patients' underlying diagnosis, comparison of the four subgroups; diagnoses were classified in 10 major categories; percentage of n in each subgroup, relative frequency, listed according to the frequency of the total sample; AD, n = 50 (24%); CD, n = 60 (29%); LTD, n = 41 (20%); LLD, n = 57 (27%).
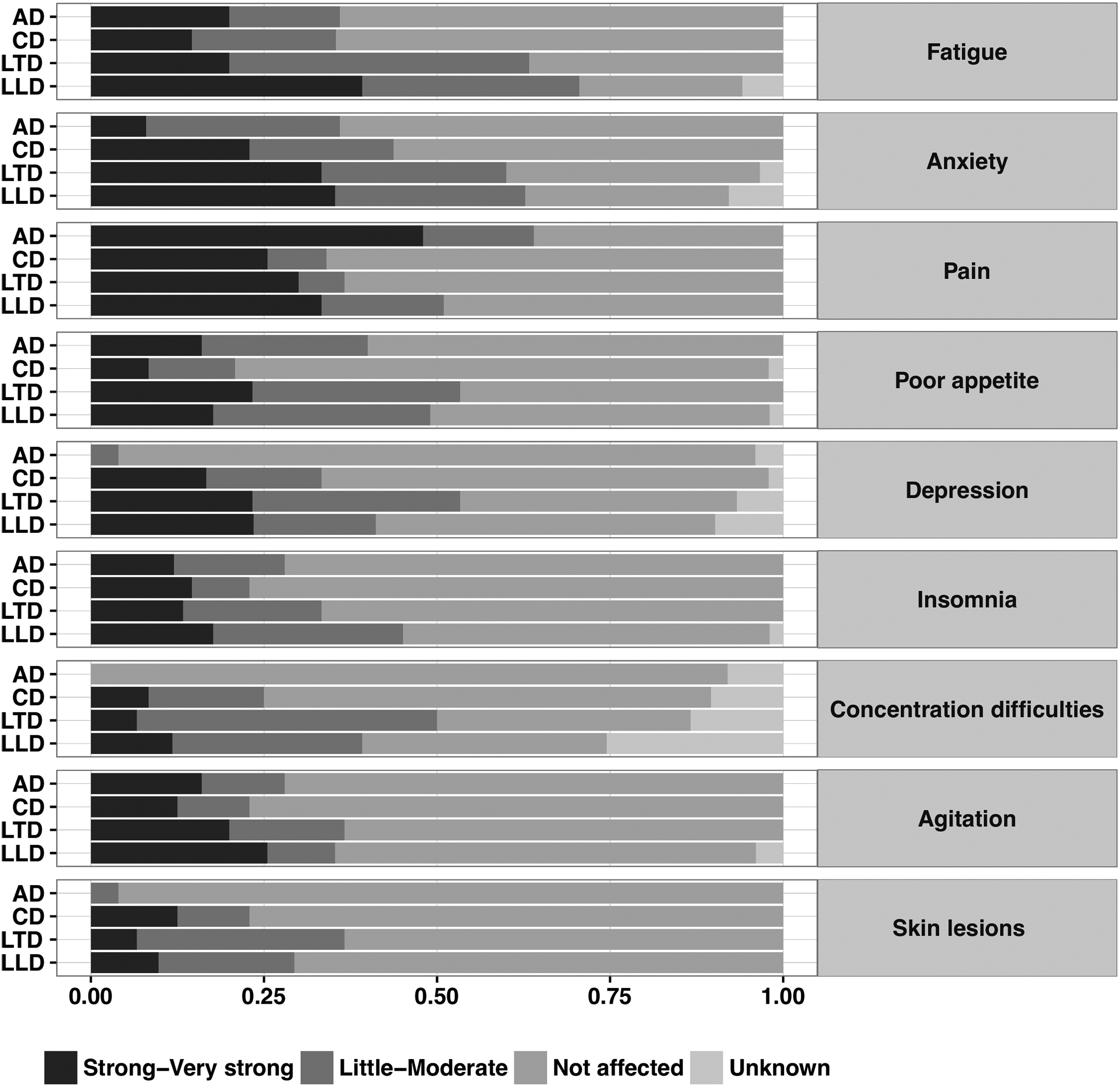
Intensity of the most frequent symptoms in the four subgroups among children older than one month; percentage of n in each subgroup, relative frequency; AD, n = 50 (24%); CD, n = 60 (29%); LTD, n = 41 (20%); LLD, n = 57 (27%).
Comparison of children with LTD to those with AD/CD
In children with LTD, malignant neoplasms formed the largest underlying disease group (29%, Fig. 2). Patients with LTD had the longest median hospital stay overall (MDN 39; IQR 7–87, Table 2). They suffered mostly from fatigue (63%), anxiety (60%), and depression and poor appetite (both 53%, Fig. 3). The frequency and burden of poor appetite were particularly high in children with LTD compared to those with AD/CD.
Comparison of children with LLD to those with AD/CD
Children with LLD suffered mostly from genetic/congenital disorders (23%, Fig. 2). The life expectancy of 52% of patients with LLD was estimated to be more than five years. In 17%, this estimation was less than one year, and in 9%, a survival of one to five years was estimated. For 22% of the patients, the interviews indicated difficulties estimating the duration of survival. Children with LLD received very intensive medical care and had significantly more comorbidities than children with AD/CD (p < 0.05, Table 2). In total, 33/57 patients (58%) with LLD required more than six medications and 18/57 patients (33%) more than 10 medications per day. Many patients with LLD received analgesics (25/57 patients, 44%). Strong opioids were used significantly more often in these children than in children with AD/CD (11/57, p < 0.001). Thirteen patients of those requiring sedatives belonged to the subgroup of children with LLD (72%; p < 0.05). Children with LLD suffered mostly from fatigue (71%), anxiety (63%) (p < 0.05 compared to patients with AD, both symptoms 36%, and those with CD, 35% and 44%, respectively), and from pain (57%) (p < 0.05 compared to those with CD, 35%; patients with AD 68%; Fig. 3).
Comparison of children with LLD to those with LTD
Despite the high concordance between the two, the group of children with LLD differed from the subgroup of children with LTD. Children with LLD were more often affected by rare diseases than those with LTD (p < 0.05). The ICD-10 codes for LLD matched significantly more often with one of Hain's ICD-10 Directory than the LTD ICD-10 codes. There was significantly more drug use in children with LLD, especially more antibiotics, antacids/PPI, non-opioids, and strong opioids (p < 0.05). In addition, sedative medications were used significantly more often in children with LLD. Sweating and urinary problems occurred significantly more frequently in these patients compared to patients with LTD.
See Supplementary Data for a detailed analysis of the four subgroups (Supplementary Data are available online at www.liebertpub.com/jpm).
Discussion
This is the first cross-sectional study to address the prevalence of pediatric patient groups with a particular emphasis on their need for palliative care and was conducted in one of the largest tertiary care pediatric centers in Europe. This survey revealed a high prevalence of patients with complex medical conditions. Remarkably, only a quarter of all patients suffered from ADs, while nearly 50% of all inpatients suffered from life-threatening or LLDs. Children with LTDs or LLDs presented with a wide variety of underlying conditions and a substantially high proportion of rare diseases. They presented with complex medical conditions with a considerably higher need for medical devices, medications, and nursing care. The symptom burden was high in both groups, and the median length of stay was considerable. Children with LTD and LLD may thus need additional specialized care that focuses on their palliative care needs.
When establishing the subgroups of children with AD, CD, and LLD, high concordance was observed between the PPC experts, whose decisions were based on the ICD-10 codes of the underlying diagnoses, and the caring physicians, whose decisions were based on personal contact with patients. However, the definitions of LTD showed the highest rate of mismatch between the PPC experts and the caring physicians. The lack of an objective identification tool might lead to disagreement between professionals. 24 This may delay or even impede the provision of appropriate additional care, including consulting palliative care services for these patients. 25 Importantly, the early identification of palliative care needs and the subsequent inclusion of a specialized team yield advantages such as improved parental adjustment, sufficient symptom control, fewer emergency admissions, and fewer unexpected deaths at hospital.12,26,27
Consistent with previous studies, the children with LTD/LLD mainly suffered from malignant neoplasms and genetic/congenital or neurological/neuromuscular disorders.5,6 The clinical course of patients with LLDs is often unpredictable, and sudden deterioration with possible subsequent death may occur at any time.28,29 The precarious conditions of these patients show a high concordance with the characteristics of those with LTDs. Therefore, there are good reasons to consider and discuss them as one group in the hospital setting with similar care needs.
Several findings of this study imply that there is a fundamental and profound need for PPC in tertiary pediatric centers. The findings of this study showed that almost 50% of the patients live with LTD/LLD, 82% of whom suffer from rare diseases. For a large number of rare diseases, the exact diagnosis and course of the disease are not known, which further increase the burden of the affected families.30,31 In describing and comparing subgroups, we found that children with LTD/LLD suffered a high burden in all clinical parameters, including a high demand for medications, medical devices, and nursing care. This underscores the need for properly resourced PPC with appropriate assessments.6,32 More than half of the patients with LLD had an estimated survival of more than five years. This corroborates the findings of other surveys and leads to the need for palliative concepts of transition to adult services. 33
This study replicates the findings of previous studies that indicate that LTDs/LLDs are associated with a high burden of symptoms, especially fatigue, anxiety, and pain.32,34–37 Fatigue and anxiety are difficult to treat. Their differential diagnosis is complex, as these symptoms cause great impairment and relate to and involve one another.38,39 A holistic approach to treatment with spiritual, emotional, and psychological support is important.28,40,41 A positive result of this study is the health professionals' acknowledgment of these psychologically vague symptoms. Pain was one of the most common symptoms experienced by inpatient children, regardless of subgroup. The high prevalence of pain during hospitalization, both in children and in adults, is very well known42,43 and highlights the urgent need for intensive pain prevention and management. 44 Pain plays a predominant role in perpetuating a vicious cycle of symptoms. Effective pain management approaches should include not only pharmaceutical techniques but also cognitive-psychological interventions.45,46
To appropriately identify children with life-threatening and life-limiting conditions, ICD-10 codes are not sufficient and need to be complemented with a multioperational approach.11,17,18 Clinical characteristics, including the number of medications, use of medical devices, and predominance of symptoms, must complement the diagnostic code. Preliminary attempts to establish a method of detecting children with palliative care needs are in process.47,48
Limitations
This is an exploratory cross-sectional study that does not reflect trends over time, but provides insight into a single typical day at a pediatric tertiary care center. Further studies over a longer time period and in more tertiary care centers are needed. A study based on interviews will always depend on the individual experiences of the interviewees. Conducting the study in a large center led to a relatively large group of interviewees. Using a standardized interview and prior interviewer training, we tried to improve the objectivity of the assessment. As information regarding symptoms was based on external assessments performed by the medical team, these results may deviate from a patient's or parent's perspective on symptoms. Useful further assessments of symptoms could include questioning of parents and children themselves, for example, with visual pain scales and incorporate objective parameters such as physiological measurements. In this study, we did not conduct patient-based need assessments to assess whether or not patients were open to receiving palliative care services.
Conclusion
The analysis of patient subgroups of those suffering from AD, CD, LTD, and LLD provides a unique picture of the diversity within a large pediatrics center and highlights the burden of disease of severely ill children. A substantial proportion of pediatric inpatients suffered from life-threatening or LLDs, as well as rare diseases. They showed complex medical conditions and a high burden of symptoms, indicating a high need for additional care. Although the data need to be confirmed in further studies, our results imply the explicit need to implement PPC structures in pediatric tertiary care centers, not only for patients at the end-of-life period but also for those whose conditions temporarily require additional supportive care. 49 Further investigations are needed to identify the unique needs of these patients under the given clinical circumstances. Therefore, health professionals and affected families must work together to clarify additional needs of patients with severe chronic and rare diseases and to develop adequate supportive care structures in hospitals. 50
Footnotes
Acknowledgments
The authors thank the study participants, the interviewers, and all of the pediatric departments at the Charité Universitätsmedizin Berlin. The authors are very thankful to Dr. Andreas Busjahn from HealthTwiSt GmbH Berlin for helping with the data analysis.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.