
Abstract
Abstract
Background:
Factors leading to inappropriate critical care, that is treatment that should not be provided because it does not offer the patient meaningful benefit, have not been rigorously characterized.
Objective:
We explored medical record documentation about patients who received inappropriate critical care and those who received appropriate critical care to examine factors associated with the provision of inappropriate treatment.
Design:
Medical records were abstracted from 123 patients who were assessed as receiving inappropriate treatment and 66 patients who were assessed as receiving appropriate treatment but died within six months of intensive care unit (ICU) admission. We used mixed methods combining qualitative analysis of medical record documentation with multivariable analysis to examine the relationship between patient and communication factors and the receipt of inappropriate treatment, and present these within a conceptual model.
Setting:
One academic health system.
Results:
Medical records revealed 21 themes pertaining to prognosis and factors influencing treatment aggressiveness. Four themes were independently associated with patients receiving inappropriate treatment according to physicians. When decision making was not guided by physicians (odds ratio [OR] 3.76, confidence interval [95% CI] 1.21–11.70) or was delayed by patient/family (OR 4.52, 95% CI 1.69–12.04), patients were more likely to receive inappropriate treatment. Documented communication about goals of care (OR 0.29, 95% CI 0.10–0.84) and patient's preferences driving decision making (OR 0.02, 95% CI 0.00–0.27) were associated with lower odds of receiving inappropriate treatment.
Conclusions:
Medical record documentation suggests that inappropriate treatment occurs in the setting of communication and decision-making patterns that may be amenable to intervention.
Introduction
W
Although clinicians agree that treatments that are contrary to their clinical and professional judgment should be avoided,8–12 there is incomplete understanding of how and why inappropriate treatment occurs. 13 Using a qualitative–quantitative mixed-methods approach, we aimed to understand the determinants of inappropriate treatment by performing an analysis of verbatim clinical documentation in the medical records of patients who were assessed as receiving inappropriate treatment.
Methods
Details of the definition of inappropriate treatment and the core data collection are described in detail elsewhere 14 and summarized here. This study was approved by the UCLA IRB (IRB No. 11-002942-CR-00004). For three months (December 15, 2011 through March 15, 2012), critical care attending physicians in five ICUs in one academic health system completed a daily questionnaire, asking whether their patients were receiving inappropriate treatment. After collapsing daily survey data, 1136 patients were categorized as patients for whom treatment was never perceived as inappropriate or as patients with at least one assessment of inappropriate treatment. Hospital mortality and six-month mortality were abstracted.
Medical record abstraction
Three nurses and one internal medicine resident abstracted the medical records of the 123 patients who were assessed as receiving inappropriate treatment and the 66 patients who were assessed as receiving appropriate treatment but died within six months of ICU admission. Statements from any member of the healthcare team regarding the aggressiveness of treatment such as descriptions of prognosis, expected outcomes, and documentation reflecting communication or decision making were abstracted verbatim.
Qualitative analysis
To perform a qualitative content analysis, ATLAS-TI 7.5.6 was used to manage and code the verbatim abstractions. Three physicians (T.H.N., D.M.T., N.S.W.) of different disciplines (critical care, family medicine, and general internal medicine) used an iterative review process15–17 to develop themes and subthemes concerning prognosis and factors that influence aggressiveness of treatment. One investigator (T.H.N.) applied codes to abstractions from all 189 patients. To assess intercoder reliability, another investigator (D.M.T.) independently coded a 15% random sample of the abstractions with a kappa of 0.78. Discrepancies were resolved by consensus.
Themes were grouped into domains: predisposing characteristics, physician–patient/surrogate communication, intermediate outcomes, and decision making. These domains were adapted from the conceptual frameworks of Torke, 18 Street, 19 and Ashton, 20 and are presented in a newly constructed conceptual model of how communication and decision making lead to appropriate or inappropriate treatment.
Statistical analysis
For each patient, we transformed the qualitative findings into quantitative data by noting the presence or absence of each theme. We performed bivariate and multivariate analyses to determine the relationship of each theme with whether the patient received inappropriate treatment. For the multivariable logistic model, we retained themes that occurred in at least five patients and appeared in both inappropriate and appropriate treatment groups. Analyses were performed using STATA 12.1.
Results
Thirty-six critical care physicians in five ICUs assessed 123 patients (11% of the 1136 evaluated patients) as having received inappropriate treatment on at least one day in the ICU. Patients who were assessed as receiving appropriate treatment had lower in-hospital mortality (4.6% vs. 68%) and six-month mortality (7.3% vs. 85%) than those receiving inappropriate critical care.
Qualitative analysis revealed 21 themes and 74 associated subthemes; their definitions with negative and positive exemplars were collected in a codebook. Table 1 presents quotations representing each theme.
ICU, intensive care unit; Pt, patient.
Conceptual model
Our conceptual model (Fig. 1) organizes the themes associated with decision making into four domains.
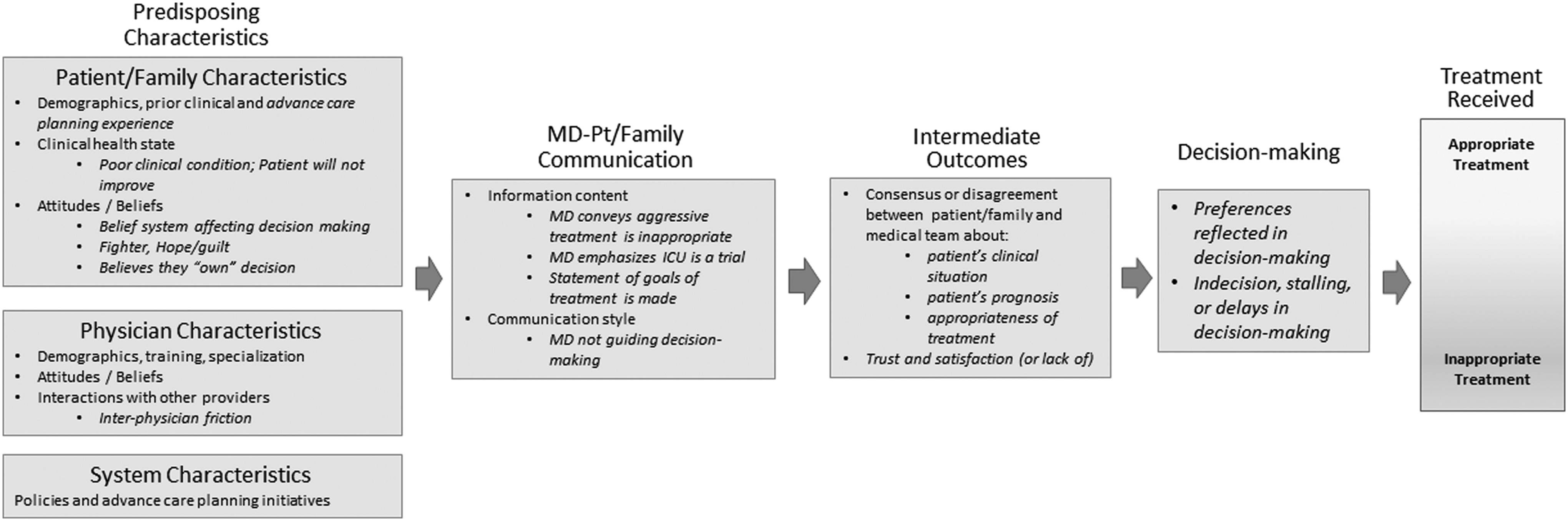
Conceptual Model of Decision Making in the ICU. This conceptual model illustrates the factors associated with decision making in the ICU once a physician establishes a patient's clinical circumstances and prognosis. Factors identified in the qualitative analysis are italicized. Predisposing patient/family, physician, and systems characteristics influence the quality and quantity of physician–patient/family communication. In turn, whether and how physicians communicate about a patient's clinical situation and guide decision making can influence intermediate outcomes, such as patient/surrogate trust and the process of sharing an understanding of the situation and making joint decisions. These intermediate outcomes influence the decision making that results in inappropriate or appropriate treatment received. ICU, intensive care unit.
Predisposing factors
We found two themes that relate to the patient's clinical condition, one focused on the condition being poor (i.e., “multiorgan failure”) and the other focused on the inability to improve (i.e., “prognosis is dismal”). Other themes reflected the patient's/surrogate's attitudes and beliefs, for instance, the patient is a “fighter” (such that the notion of forgoing aggressive treatment equates to giving up).
Physician–patient/family communication
This domain consists of the content of the information exchanged as well as the negotiations and interactions that are associated with the information exchange18,20 (i.e., whether the physician conveys that aggressive treatment is inappropriate or emphasizes it as a time-limited trial, whether the patient/family expresses preferences in terms of patient's goals, and whether the physician guides decision making). Documented goals include desires to go home, be free of disability, maintain cognitive function, and “stay alive at all cost.” Statements were marked as “Physician not guiding decision making” when there were no recommendations made, one way or the other for patients with a poor prognosis. Statements within this theme ranged from statements that simply presented options without a medical recommendation, such as “Will need to discuss trach[eostomy] and PEG [feeding tube] vs end-of-life discussion” to an acquiescence to the family's insistence on aggressive treatment despite a grave prognosis (“We placed a trach[eostomy] at the request of the family despite her terminal cancer”).
Intermediate outcomes
Physician–patient/family communication leads to intermediate outcomes, which include patient decision making, and can result in consensus or disagreement.18,19 This domain contains six themes, including themes regarding agreements/disagreements with the patient's condition, prognosis, and/or treatment (i.e., “He does not believe that his wife is suffering”), and distrust and dissatisfaction (i.e., “He felt his mother had been ignored for 6 weeks”).
Decision making
High-quality decision making is informed by clinical evidence, concordant with values, and mutually endorsed. 18 We identified two themes: when preferences were reflected in the decision and when there was indecision. The theme “patient preference reflected in decision making” was characterized by two subthemes: family acknowledging the need to focus on patient's preferences and the course of treatment being dictated by advance care planning. The theme “indecision, stalling, or delaying decision making” was found to be associated with inappropriate critical care. For some, decision making was delayed because of the desire to wait for family members to assemble. In other instances, the treatment plan was stalled by indecision or an unwillingness to specify preferences (i.e., “Patient is unwilling to communicate desires on repeated attempts”).
Statistical analysis
Bivariate analyses showed several themes being associated with inappropriate treatment (Table 2). Sixteen themes were included in multivariable analysis, and four themes were found to be significantly associated with the receipt of inappropriate treatment (Table 3). When decision making was not guided by physicians (odds ratio [OR] 3.76, confidence interval [95% CI] 1.21–11.70) or was delayed by patient/family (OR 4.52, 95% CI 1.69–12.04), patients were more likely to receive inappropriate treatment. The likelihood of receiving inappropriate treatment decreased with documentation of communication about patient's goals (even if unrealistic) (OR 0.29, 95% CI 0.10–0.84) and patient's preferences driving decision making (OR 0.02, 95% CI 0.00–0.27). Table 4 contains quotations illustrating these four themes and their subthemes.
Bold indicates p < 0.05.
Patient/family = patient and/or family.
Bold indicates p value < 0.05.
Discussion
By analyzing clinical documentation for patients perceived as receiving inappropriate critical care, our study offers a novel perspective on how communication and medical decision making contribute to inappropriate critical care. Although medical record documentation is an imperfect reflection of events, 21 it is a fundamental component of patient care, offers the perspective of the clinicians in real time, and serves to convey information to all stakeholders in the healthcare team.22–24 Although nearly all of the factors identified in this study have been previously identified as obstacles to optimal decision making, this study directly links these factors to the provision of inappropriate treatment and identifies components that are independently associated with inappropriate ICU care. Importantly, many of these care processes are under at least partial control of the healthcare team and can be improved upon.
Since predisposing factors are often immutable at admission, it is encouraging that we found that they were not independently associated with inappropriate treatment. More important was whether the decision-making process incorporated the patient's goals and whether the physician guided decision making during patient/family–physician communication. The finding that “indecision, stalling, and delays in decision making” is related to inappropriate treatment underscores the importance of prompt family meetings and early palliative care involvement. The finding that the theme “physician not guiding decision making” is associated with inappropriate treatment demonstrates that the manner in which information is communicated is crucial. Indeed, the language used to frame treatment options has been shown to influence treatment decisions. 25 This finding is also consistent with a prior study that found that a high-intensity medical center, compared with a lower intensity facility, was more likely to offer open-ended trials of life-sustaining treatments without addressing long-term goals. 26
Our study has several limitations. Although we worked from rich medical record documentation, our analysis is limited to what providers wrote in charts. The exact content of the information exchanged during family meetings is unavailable. Also, physicians provided the majority of the analyzed documentation, indicating a dearth of documentation about decision making from other providers and yielding domains built on only physician communication. The sample size is small and all patients were from a single health system. The patients who died after receiving appropriate ICU treatment may not be completely comparable with those receiving inappropriate treatment because they may have had different prognoses. Finally, patient and family viewpoints are included only as documented by providers.
Conclusions
The provision of inappropriate critical care is associated with a complex set of coexisting patient/family and physician factors, communication, and decision-making domains, some of which may be targeted by interventions to reduce inappropriate treatment.
Footnotes
Acknowledgments
This project was supported by a donation from Mary Kay Farley to RAND Health. The funder played no role in the design and conduct of the study; collection, analysis, and interpretation of the data; or preparation, review, or approval of the article. T.H.N. was supported by the UCLA CTSI KL2 UL1TR000124, the NIH-NIA 1K23AG047900-01A1, and the NIH loan repayment program.
Author Disclosure Statement
No competing financial interests exist.