
Abstract
Abstract
Background:
Although limited, the descriptions of Community-Based Palliative Care (CBPC) demonstrates variability in team structures, eligibility, and standardization across care settings.
Objective:
In 2014, Four Seasons Compassion for Life, a nonprofit hospice and palliative care (PC) organization in Western North Carolina (WNC), was awarded a Centers for Medicare and Medicaid Services Health Care Innovation (CMMI) Award to expand upon their existing innovative model to implement, evaluate, and demonstrate CBPC in the United States. The objective of this article is to describe the processes and challenges of scaling and standardizing the CBPC model.
Design:
Four Season's CBPC model serves patients in both inpatient and outpatient settings using an interdisciplinary team to address symptom management, psychosocial/spiritual care, advance care planning, and patient/family education. Medicare beneficiaries who are ≥65 years of age with a life-limiting illness were eligible for the CMMI project.
Results:
The CBPC model was scaled across numerous counties in WNC and Upstate South Carolina. Over the first two years of the project, scaling occurred into 21 counties with the addition of 2 large hospitals, 52 nursing facilities, and 2 new clinics. To improve efficiency and effectiveness, a PC screening referral guide and a risk stratification approach were developed and implemented. Care processes, including patient referral and initial visit, were mapped.
Conclusion:
This article describes an interdisciplinary CBPC model in all care settings to individuals with life-limiting illness and offers guidance for risk stratification assessments and mapping care processes that may help PC programs as they develop and work to improve efficiencies.
Background
C
In 2010, the Affordable Care Act established the Centers for Medicare and Medicaid Services Innovation (CMMI) Center to help innovate and achieve value-based healthcare. In 2014, Four Seasons received a CMMI Award titled “Increasing Patient and System Value with Community Based Palliative Care,” to test a new care delivery and payment model for PC. The CBPC program at Four Seasons was started in 2003 to meet the needs of those with serious life-limiting illness. The program serves patients in both inpatient and outpatient settings using an interdisciplinary team of physicians (MDs), physician assistants (PAs), nurse practitioners (NPs), social workers (SWs), and chaplains. The CBPC program addresses the needs of people with life-limiting illness through symptom management, prognostication, psychosocial and spiritual care, advance care planning (ACP), caregiver support, patient/family education, and coordination with community-based resources. Care is delivered via in-person visits in all care settings (hospital, home, clinic, and facility), phone-based monitoring, and follow-up with 24/7 coverage. Within a seven-year period, Four Seasons CBPC program expanded to include three community hospital systems. In the hospital inpatient setting a 1:1 ratio of physicians to Advanced Practice Professionals (APP includes PAs and NPs) is utilized while the outpatient setting involves a ratio of 1:4 physician to APP. To monitor quality data, a standardized process of data collection was developed using the Quality Data Collection Tool (QDACT) in partnership with colleagues at Duke University. In 2010, the PC Immersion Course was developed to improve clinical competencies.
This CBPC model at Four Seasons involves (1) a lead PC provider organization (Four Seasons); (2) motivated partner organizations that span settings, in which local patients receive care (hospitals, facilities, and clinics); (3) workforce development, focused on nonphysician providers; (4) clinician education conducted through the PC immersion course and continued mentoring; (5) interdisciplinary teamwork through interprofessional practice collaboration; and (6) quality assessment/quality improvement. With the Innovation Award, Four Seasons expanded upon this existing model to implement, evaluate, and demonstrate the value of CBPC in the region. This article describes the infrastructure, implementation, standardization, and scaling of the CBPC model over the first two years of this three-year award.
Materials and Methods
Target population and geographic region
To be eligible for the CMMI project, patients must have a life-limiting illness (defined as “any disease/disorder/condition that is known to be life-limiting or that has a high chance of leading to death” 4 ) and be ≥65 years of age with traditional fee-for-service Medicare coverage (excludes Medicare Advantage [MA]). With the CMMI project, Four Season's CBPC program was expanded from 4 to 24 counties in Western North Carolina (WNC) and into upstate South Carolina (SC). Four Seasons service area expanded from 4 to 13 counties in WNC and serves patients in the home, clinic, three small community hospitals, and facilities. The number of collaborating facilities (skilled, nursing, assisted living, and residential facilities) that Four Season's serves increased from 79 to 90. The initial and primary project partner, Palliative Care and Hospice of Catawba Valley (Catawba), began enrolling patients in March 2015 and serves patients in the home, one small community hospital, 2 PC clinics, and 41 facilities in 11 counties in WNC. In March 2016, Greenville Health Systems (GHS) in SC began enrolling patients in the program along with Mission Health System in NC, who joined in June 2016. Both additions represent large hospitals with bed size >700.
Integration of hospitals into the project involved the administrative level, hospital business managers, and financial analysts to determine areas of highest healthcare utilization and highest costs to establish how CBPC could assist in improving care. Needs assessment-identified gaps in service and helped the team prioritize needs. On the clinical level, ongoing education to providers and participation in conferences, team meetings, and hospitalist rounds have helped build collaborative relationships. In addition, readmission task forces have been set up at several collaborating hospitals to help identify CBPC referrals and manage patients across the continuum of care. To aid in data collection and patient tracking, a registered nurse (RN) was added at each hospital.
Measures were put in place to increase the number of facilities participating in the program. In the nursing homes; quality measures, star ratings, and readmission rates were used to identify areas that CBPC could be of service. Clinical staff were educated on the benefits of CBPC, and training sessions were conducted on topics such as ACP, pain/symptom management, and bereavement support. In the Assisted Living Facilities, CBPC was promoted and marketed as a mechanism to keep residents in the facility by helping them manage troublesome symptoms and aligning care according to treatment preferences.
Patient care
Care is delivered by an interdisciplinary team via in-person visits, and phone-based monitoring is provided to patients as needed on a 24/7 basis. RNs, a new addition to the model, allows for improved care management and coordination across the system. Further expansion of the CBPC model included patient family advisors, community educators, and increased administrative support. A Practice Manager was put in place to provide oversight, standardization of care, and track clinician dashboards. Dashboards include productivity, hospice transitions, PC deaths, and discharges, and this information is shared with providers monthly. A PC Operations Leader was hired to help improve processes and manage the grant activities. NPs will generally manage a caseload of 80–100 patients, while RNs and SWs manage around 125–150 patients depending on the care setting.
Patient recruitment and eligibility
Community educators travel to hospitals, physician offices, and facilities to educate stakeholders about the benefits of CBPC. Other outreach venues include professional meetings, direct-to-patient outreach (community groups, churches, etc.), and public education. Referrals to the CBPC program can come from any care setting and by self-referral. A screening tool was developed to help referring providers determine CBPC eligibility. The screening tool was developed by a consensus group (made up of PC team members) who reviewed the literature around PC screening questions and hospital readmissions. Social determinants and local coverage determinants of the different advanced illnesses were also identified and included in the screening guideline.
Patient referral
An interdisciplinary clinical task force at Four Seasons' has begun to map out the CBPC process from patient referral to discharge, defining what positions were responsible for each step, so that this model can be scaled and replicated. The interdisciplinary CBPC clinical task force is composed of physicians, administrators, NPs, a chaplain, and a SW. There were several discussions surrounding the informed consent process, including the responsible parties for obtaining consent. When possible, administrative teams obtain consent through an encrypted email. Other important discussions involved patient information, including the Health Insurance Portability and Accountablity Act of 1996 (HIPPA) privacy authorization form, the controlled substance agreement, the new patient handbook, and the time frame for patients to receive this information.
Risk stratification
To help align patients' needs with timing of consults, frequency of visits, and need for psychosocial or spiritual intervention, risk stratification tools were developed by the clinical task force. Based on the experiences of the various disciplines, the task force determined factors that would indicate whether a patient was high, medium, or low risk and the time frame for follow-up. Once formulated, the risk stratification tools were presented to the project Advisory Council for review (made up of national leaders in the field of PC), who gave further input. Using the advisory council's suggestions, the risk stratification tools were redefined and brought to the CBPC team for approval and implementation.
Initial visit
The interdisciplinary clinical task force mapped the initial CBPC visit by discussing current process flow, improvements to the current process, then implementation of improvements. There was a large focus on the RN initial telephone assessment, as this assessment is used to determine priority for seeing patients at home versus clinic or a facility.
Results
Target population and geographic region
A significant percentage of patients in Four Season's CBPC program are younger than 65 years old, and about 18% are enrolled in MA plans, therefore, only about half of patients meet program eligibility requirements, which required they be age-eligible and traditional Medicare beneficiaries. When the grant was written, 80% of patients in the region had traditional Medicare, however, over time, there has been an increase in referrals of younger patients and a higher number of patients with MA plans. Our partnering organizations also have <50% CBPC patients with traditional Medicare.
In the first six months of the program, new stakeholder relationships were built, data use agreement contracts were initiated, and the model was expanded into neighboring counties in WNC. Catawba joined the program during month 7, further expanding the number of counties served in WNC. During months 6–12, infrastructure to carry out CBPC was built at Four Seasons and Catawba. In the second year, patient enrollment increased significantly due to the additions of two large hospitals, GHS and Mission. Challenges of scaling into hospitals included difficulty engaging partners due to political and financial reasons, concerns around data sharing and contracting, and increased clinician burden. Once patients started enrolling in the hospitals there continued to be fragmentation issues across care settings, making patient navigation challenging. For example, electronic health records were not interoperable, and there were limited processes in place to achieve smooth patient transitions.
CBPC delivery in rural WNC has proven to be very difficult. Issues include provider burnout with long travel time through mountainous terrain, inefficient systems to manage care, and increased cost of care. A pilot telemedicine program using a telehealth software application (TapCloud) and videoconferencing has helped overcome some of these challenges in rural areas.
Patient eligibility
The screening tool developed to help referring providers determine CBPC eligibility includes serious illnesses, physical and social determinants, utilization of resources, LACE index (Length of hospitalization “L,” acuity of the admission “A,” comorbidities “C,” and emergency department use “E”), 5 and the well-validated surprise question “in your clinical opinion would you be surprised if this patient died in the next year?” 6 (Fig. 1). Physical limitations include severe functional decline, nonambulatory, debility, fall risk, and needs assistance with activities of daily living. Serious illnesses categories include multiple comorbidities and end-stage illnesses. Utilization of resources examines frequency of healthcare utilization, high-risk medications, and recent sentinel events. Depression, low income, limited access to care, transportation issues, substance issue, and lack of caregiver support are some of the at-risk social determinants for referral to CBPC (Fig. 1). Patients should also be referred to CBPC if they have a LACE score >12 or the provider answers no to the surprise question. Using the screening tool as a guide, clinicians identify and triage patients suitable for CBPC.
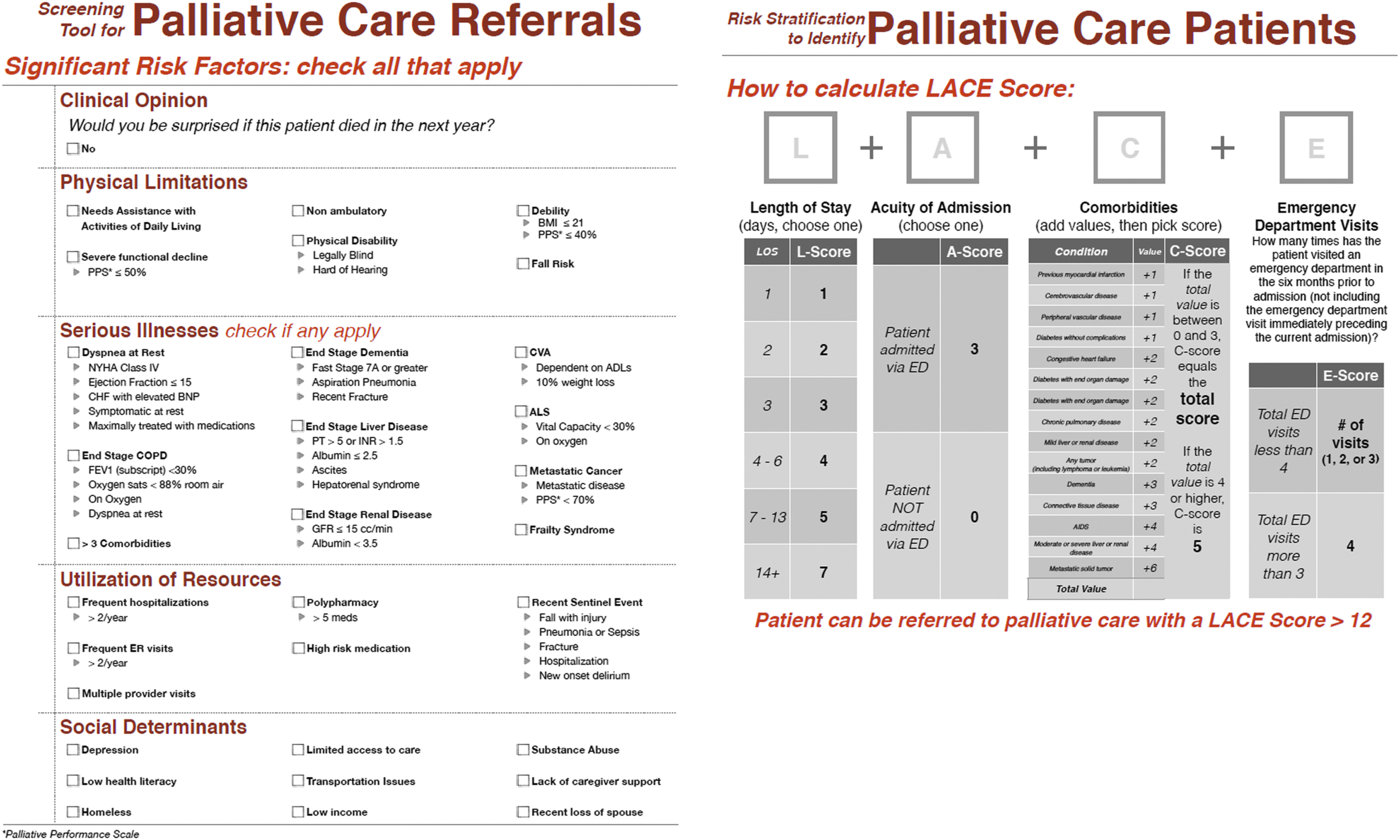
Screening Guidelines for Palliative Care Referrals. Using screening guidelines, clinicians identify and triage patients suitable for palliative care. Screening guidelines include serious illnesses, physical and social determinants, utilization of resources, LACE (Length of hospitalization “L,” acuity of the admission “A,” comorbidities “C,” and emergency department use “E”) index (inpatient only), and the well-validated surprise question “in your clinical opinion would you be surprised if this patient died in the next year?”
Patient referral
The clinical task force mapped out the patient referral process, which involves obtaining patient records, determining eligibility, completing initial clinical assessment and determining priority status, and scheduling appropriate visits (Fig. 2). Administrative personnel are responsible for reviewing patient referral information, verifying insurance, obtaining medical records, and entering patient information into the CBPC caseload. Once a patient is enrolled in the program, they are tracked by administrators, including transitions to hospice, PC deaths, discharges, and active caseloads. For routine facility patients, administrative personnel obtain verbal consent, notify the provider, and schedule a visit in less than or equal to two weeks. For home, clinic, or other facility referrals, a RN performs an initial clinical phone assessment that includes obtaining verbal consent and determining CBPC eligibility and risk. If a patient is hospice eligible, CBPC nurses collaborate with hospice to admit the patient to hospice (Fig. 2). If a patient is CBPC eligible and high risk, an RN monitors the patient, and a provider visit is scheduled at the home, clinic, or facility for ≤48 hours. If a patient is CBPC eligible and not high risk, the patient is scheduled to have a provider visit at the home in 7–10 days or at the clinic in less than or equal to two weeks.
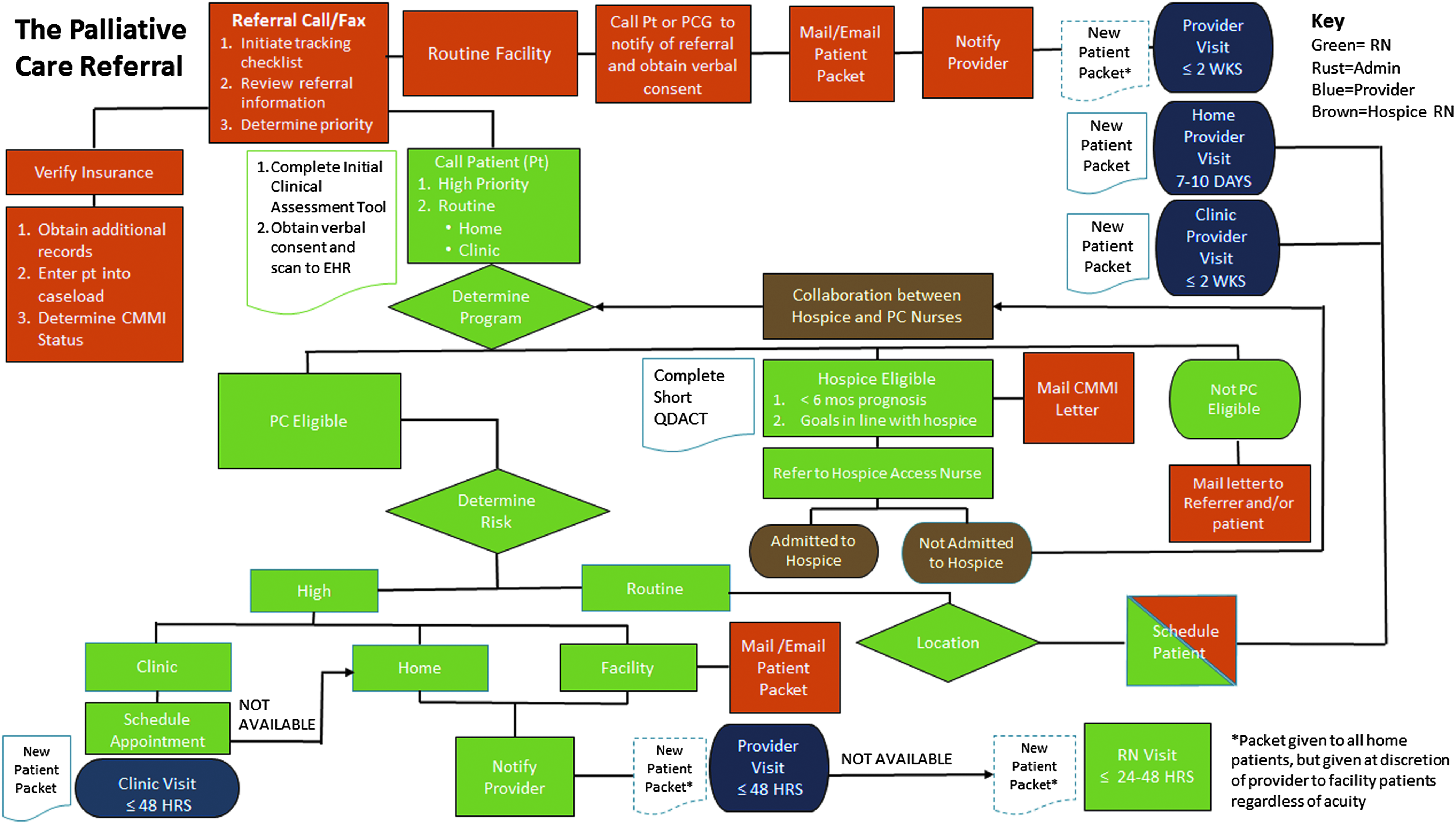
Mapping the steps of a palliative care referral. The palliative care referral process involves obtaining patient records, determining eligibility, completing initial clinical assessment and determining priority status, and scheduling appropriate visits.
Risk stratification
Risk stratification tools were developed to help determine timing of consults, frequency of visits, and needs for psychosocial or spiritual intervention (Fig. 3). On the initial visit a patient is stratified as high, medium, or low acuity in terms of clinical, psychosocial, and spiritual risk. The clinical risk areas include the following: recent care setting transitions, symptom burden, functional status, number of medications and medication changes, nutritional status, and recent infections. If a patient is stratified as a high medical risk, an RN will monitor the patient and a provider visit is scheduled to occur within 48 hours. The patient will have an additional RN follow-up call or visit within 72 hours. A medium or low-risk patient will have provider visit less than or equal to two weeks and a follow-up telephone call or visit with an RN within two weeks for medium risk and within one month for low risk. Psychosocial risks include cognitive changes, mental health issues, signs/symptoms of abuse or neglect, substance abuse, complex family dynamics, and caregiver issues. Important risks for spiritual distress include existential suffering, hopelessness, no spiritual/community support, or fear of dying. High-acuity patients on psychosocial or spiritual risk stratification will have a telephone call or visit with a SW/chaplain within 24–48 hours, medium risk within seven days, and low risk within two to three weeks. Ongoing visit frequency for high-risk patients is 7–10 days, medium risk two to three weeks, and low risk four to six weeks (Fig. 3).

Palliative care risk stratification assessments (medical, psychosocial, and spiritual). Risk stratification assessment (high, medium, or low) according to recent transitions, physical, functional, psychosocial, and spiritual needs. On the initial visit a patient is stratified and risk stratification is an ongoing process in all domains of care. Risk stratification helps to align patients' needs with timing of consults, frequency of visits, and need for psychosocial or spiritual intervention.
Initial visit
The initial CBPC visit is broken up into previsit, visit, and postvisit activities (Fig. 4). Previsit activity involves collection of patient background information. The visit involves patient education, a history and physical exam, symptom/medication review, spiritual assessment, functional status, and identification of goals and ACP (Fig. 4). Postvisit activities include the provider determining risk level and collaborating with other doctors and CBPC team members to formulate a care plan. Quality data collection is entered postvisit or real-time through QDACT, which captures symptoms, prognostication, ACP, caregiver burden, and functional status. 7 Engaging clinical providers to collect quality data is a struggle, especially if metrics are not embedded in the electronic medical record. Having monthly quality meetings to present data to clinicians and involving them in performance improvement projects have been beneficial and have increased the buy in over the importance of data collection.

Mapping the Palliative Care Initial Visit. The initial palliative visit has been broken up into previsit, visit, and postvisit activities. Previsit activity involves collection of patient background information. The visit involves patient education, a history and physical exam, symptom and medication review, spiritual assessment, functional status and safety assessment, identification of goals and advance care planning, and formulation of care plans. Postvisit activities include the provider determining risk level and collaborating with other doctors as well as palliative care team members.
Discussion
While the benefits of CBPC are starting to be realized on a national scale, there is significant variation of care among practices in different parts of the country. This article describes the process and challenges of scaling and standardizing Four Season's CBPC program in WNC and upstates SC as part of a CMMI funded project. Four Seasons has improved efficiency and effectiveness by implementing a CBPC screening referral guide and a risk stratification approach that aligns resources with patient needs in the clinical, psychosocial, and spiritual domains of care. We have begun to map out the CBPC process from patient referral to discharge so that this model can be replicated. Collecting quality data using a standardized tool (QDACT) helps us understand the needs of the population we serve. We can identify gaps of care, understand interventions used in treating symptoms, and map functional decline, symptom burden, and ACP to specific disease states and care settings. While analysis of data is under way, important themes are starting to emerge on where opportunities to improve care should be focused.
The first step in scaling our model involved identifying partners and stakeholders whose mission was similar to ours: to deliver high-quality PC across a continuum of settings. Data use agreements and contracting occurred so that deidentified information could be shared on quality metrics. Ongoing biweekly meetings with partnering organizations have been an important strategy to engage partners, address challenges, define opportunities for growth/improvement, and to share best practices.
As the demand for PC continues to grow, the workforce shortage will continue to increase and programs may be forced to hire practitioners with little experience and training. 8 Expertise in PC not only requires knowledge of all end-stage illnesses but also proficiency in communication skills and prognostication. By training providers in an experiential learning model through the PC Immersion Course, skills are practiced in a safe environment where learning is accelerated. As more individuals enter the workforce, robust training programs will be needed to enhance learning and provide ongoing mentorship.
We have identified several important limitations to our CBPC design. First, the geographic area of our program is limited to 25 counties in the southeast and represents a mostly Caucasian population. We recognize that this is not representative of the demographics of the United States as a whole, and a larger national demonstration project in a more broadly representative sample of patients would be an important next step. Second, Four Seasons CBPC is integrated within a hospice agency, which may not be typical of other programs. Moving to a value-based reimbursement system is shifting the incentives of hospital and healthcare systems who are starting to invest in care management programs and outpatient PC programs, hence, the parent organization may differ. Finally, the payor source in this program is limited to traditional Medicare as CMMI did not approve MA participants, and MA programs are limited in our service area.
Conclusion
As the United States moves to a more patient-centric healthcare system tied across the community, CBPC is well positioned to bridge across the continuum of care settings and deliver a person-centered interdisciplinary approach to people dealing with life-limiting illnesses.
Footnotes
Acknowledgments
This project is supported by Grant Number 1C1CMS331331 from the U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the U.S. Department of Health and Human Services or any of its agencies.
Author Disclosure Statement
No competing financial interests exist.