
Abstract
Abstract
Background:
Palliative care (PC) development is diverse and lacks an effective integration into European healthcare systems. This article investigates levels of integrated PC in European countries.
Methods:
A qualitative survey was undertaken for the 2013 EAPC Atlas of PC in Europe with boards of national associations, eliciting opinions on opportunities for, and barriers to, PC development.
Analysis:
Barriers and opportunities directly related to PC integration were identified and analyzed thematically according (1) to the dimensions of the World Health Organization (WHO) public health model and (2) by the degree of service provision in each country. A frequency analysis of dimensions and level of provision was also conducted.
Results:
In total, 48/53 (91%) European countries responded to the survey. A total of 43 barriers and 65 opportunities were identified as being related to PC integration. Main barriers were (1) lack of basic PC training, with a particular emphasis on the absence of teaching at the undergraduate level; (2) lack of official certification for professionals; (3) lack of coordination and continuity of care for users and providers; (4) lack of PC integration for noncancer patients; (5) absence of PC from countries' regulatory frameworks; and (6) unequal laws or regulations pertaining to PC within countries. Innovations in education and new regulatory frameworks were identified as main opportunities in some European countries, in addition to opportunities around the implementation of PC in home care, nursing home settings, and the earlier integration of PC into patients' continuum of care. With increasing provision of services, more challenges for the integration are detected (p < 0.005).
Conclusion:
A set of barriers and opportunities to PC integration has been identified across Europe, by national associations, offering a barometer against which to check the challenge of integration across countries.
Background
P
The WHO has proposed public health strategies, as they are understood as the best manner to integrate PC into health systems. This public health strategy is based on four dimensions: (1) appropriate policies; (2) adequate medicine availability; (3) education of policy makers, healthcare workers, and the public; and (4) implementation of PC services at all levels throughout the society. 9 More recently, the 67th World Health Assembly pleaded again for the integration of PC (I-PC) across all levels of the health systems with emphasis on universal coverage schemes. 10 In studies carried out in 2009 and 2010 to identify the main barriers for PC development in Europe, the results were presented separated by geographic region: Western and Eastern Europe.6,7 For Western countries, major barriers were the lack of education and training programs, and a lack of awareness and recognition; for Eastern European countries, financial constraints and poor opioid availability were the key barriers. A thematic study revealed that there are fears associated with opioids, and lack of funding allocation, affordability, and knowledge impeding access to the opioid medications. 11 Another study addressing barriers and approaches to the I-PC and oncology practice insisted in the need for increased PC education for both medical undergraduates and postgraduate physicians and mentioned key issues in the early I-PC, including relationship building, across multiple health systems and specialties. 12 European associations of oncologists and PC professionals reported that barriers to PC are predominantly financial. 13 Specific barriers to integration have been recently studied in different regions and health systems than Europe. From the United States, a review concluded that key barriers to greater I-PC are a lack of adequate education and training, the perception of PC as limited to end-of-life care, an inadequately trained workforce, and a fragmented healthcare system. 14
As PC is evolving in Europe with less frontiers, today's challenges have to be evaluated again, globally as a whole region, and not only looking at the existence of PC resources but also to the current issue of how to integrate them within health systems. In addition, a recent review focusing on approaches to overcome barriers that continue to affect the availability of PC in low- and medium-income countries (LMICs) concludes that the critical factors that will drive and implement change in those countries are leadership and health system stewardship within LMICs. 15 The inference is that specific approaches would be needed in some European countries regarding a different provision of PC and different levels of income.
This study aims to identify barriers and opportunities to the I-PC in European countries according to service provision levels. As in previous studies conducted by our group,6,7 we have chosen leaders' views from national PC associations collected in the last 2013 EAPC Atlas of Palliative Care 16 survey, as sources of information for this secondary analysis. This study is performed within the framework of the European Commission InSup-C project on patient-centered integrated PC. 17
Methodology
Population
Our study addresses the WHO European Region comprising 53 countries and a population of 879 million people.
Definition and framework
For this study, PC development is understood as a combination of processes, structures, policies, and resources that support the delivery of PC. 16 Barriers and opportunities were defined as factors that prevent or promote development and are classified following the four dimensions of the WHO public health strategy, 9 namely, policies, education, implementation of PC services, and medicine availability. In this point, it is worth to say that the WHO Model List of Essential Medicines includes a list of medicines considered essential for PC and opioid analgesics are included as a cornerstone for pain and PC. 17
In the InSup-C project, the following working definition of integration was adopted: “integrated PC involves bringing together administrative, organisational, clinical and service aspects in order to realise continuity of care between all actors involved in the care network of patients receiving PC.” 18 We will use this definition considering the active academic debate around what elements are necessary for integration.19–21
As previous works have demonstrated, integration happens after the development of general PC (G-PC). 2 For this article, we adopted this same concept, and our analysis considers a two-staged process where there is first G-PC and if there is improvement, then it leads to I-PC.
Data sources
This study draws on primary data from the WHO European Region of the EAPC Atlas of Palliative Care in Europe with its methods detailed elsewhere. 16 In summary, the EAPC Atlas used a multimethod approach to collect quantitative and qualitative information at the country level, with two different original surveys (“Facts questionnaire” and “Eurobarometer survey”), published information in the literature, and information collected by the EAPC Head Office and other institutions such as the World Bank or the Pain and Policy Studies Group. All the information collected for the country reports went through a peer review process to confirm the accuracy of the information before publication.
The qualitative survey of the EAPC Atlas, named “Eurobarometer,” was addressed to national associations. From the outset, the EAPC Atlas survey sought to work collaboratively in a manner that would bring together experience from groups and institutions working to promote PC in their own countries. The EAPC Head Office and the International Association for Hospice and Palliative Care (IAHPC) provided vital information in identifying national associations (or, where national associations were inexistent, organizations promoting PC at country level). The national PC association of each country was requested to nominate someone with extensive local knowledge to participate in that survey (e.g., a chairperson or secretary). Alternatively, associations could have dedicated board meetings eliciting the opinions requested in the survey. In this way, national associations provided valuable answers to the qualitative survey eliciting opinions and views on questions regarding PC development. As the WHO no longer uses the term “drug” to describe medical use of a substance, but rather medicine, in this text, the term medicine is used specifically referring to opioids.
For this study, we used only answers to specific qualitative questions on opportunities for, and barriers to, PC development at the country level of the Eurobarometer. Those questions were: (1) Please list in order of importance the three main barriers to the development of palliative care in your country at the present time, and (2) Please list in order of importance the three main opportunities to the development of palliative care in your country at the present time. In the same EAPC Atlas study, other data related to innovations in services, accreditation, education, policies, medicine availability, and vitality were also gathered. Those respondents are referred to as “PC national leaders” or, simply, “leaders.”
The data on the provision of PC services were obtained from the EAPC Atlas and a secondary analysis has already been published. 1 Total population data were extracted from the World Data Bank.
Analysis
All answers on barriers and opportunities underwent a double thematic content analysis. First, barriers and opportunities were categorized into two categories: those related to the G-PC and those in relation to the I-PC, as defined above. Only the barriers and opportunities to the I-PC are presented here. Second, barriers and opportunities to the I-PC were coded according to the dimensions of the WHO Public Health Model for PC 9 (policy, medicine availability, implementation of PC services, and education).
To classify barriers or opportunities as I-PC or G-PC, the criterion followed was whether or not they agreed with the definition of integration adopted for the study. In the confrontation with the definition, the two researchers (C.C. and E.G.) had to agree, and the differences were discussed until consensus was reached and the codes assigned. This process allowed to appreciate, in the answers analyzed, concrete aspects that facilitate or hinder the I-PC. The new aspects found, and the results of the classification, were subjected to constant revision during the process, maintaining a uniqueness of criteria that guided and facilitated the classification process. In addition, a third researcher (M.V.E.) reviewed the initial classification by making observations on some assignment that was reconsidered again and finally discussed with the research team until the final classification was obtained. In this process, some issues were considered inherently related to I-PC by nature (e.g., undergraduate education in PC); others related to G-PC (e.g., specialist education). In the results, literal quotations are presented to better show the rich nuances of the received answers.
Based on these codes, we have performed a quantitative analysis of the type and frequency of the barriers and opportunities to the I-PC in European countries. Countries were classified by level of PC service provision per million inhabitants. Four groups were characterized according to a frequency distribution, approximately matching the percentiles 25, 50, 75, and above, corresponding to “low provision,” “intermediate provision,” “high provision,” and “very high provision,” respectively. The rationale of the approach and national differences in provision are illustrated graphically (Fig. 1). A quantification of the resulting issues from the content analysis was used to describe the presence and frequency of specific barriers/opportunities to the I-PC within the diverse PC service provision levels. The chi-square test was used to assess the association between the level of service provision (low, intermediate, high, and very high) and the degree of development (G-PC and I-PC) by the dimensions of the WHO Public Health Model for PC (policy, medicine, implementation, and education).
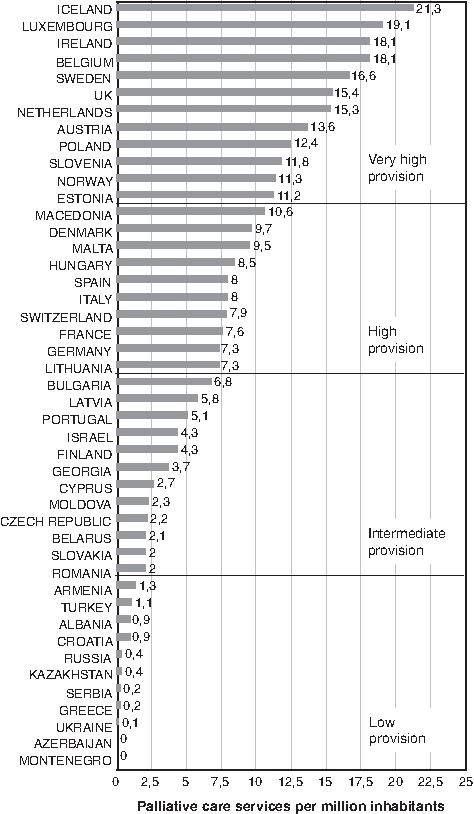
Level of provision of palliative care services in European countries by quartiles.
We use this strategy following Caracelli and Green. 22 Besides the interpretative analysis inherent to the qualitative methodology, thematic content analysis allows translating qualitative codes into numeric representation. This can be used for quantitative description of the units of analysis and/or analysis through the use of statistical routines. The quantitative translations can also be used for hypothesis testing. 23 These approaches are known in the health field.24,25
Results
In the EAPC Atlas of Palliative Care in Europe 2013, 48/53 (91%) European countries responded to the survey (five countries failed to complete the questionnaire). Initial codification concordance between the researchers was 80% for barriers and 67% for opportunities; peer review concordance reached 79%, and final consensus for the remaining was reached after discussion.
Barriers to I-PC across Europe
Categories and examples of barriers to the I-PC, classified by the WHO public health framework, are shown in Table 1. From 135 mentioned main barriers on the development of PC in 48 European countries, 43 (32%) were classified as directly related to the I-PC. From those 43 main barriers, 17 corresponded with the domain of education, 13 with the implementation of services, 11 with policy, and 2 with medicine availability.
I-PC, integration of palliative care; PC, palliative care.
Education
The barrier most often mentioned in education is the lack of basic training in PC with a particular emphasis in the absence of PC teaching at the undergraduate level:
“At the undergraduate level, training in modern principles of palliative medicine and palliative care are not available for future physicians, future nurses, and social workers. Certifications for personnel and assessment of competence in palliative medicine and palliative care are not conducted” (Russia; there are similar quotations in seven other countries)
The lack of official certification for PC was another main issue reported by six countries: Spain, Portugal, Croatia, Russia, Israel, and Sweden. Other referred to aspects included the lack of media and public advocacy and inadequate legislation with regard to PC education.
Policy
National associations from Belgium, Italy, Germany, Finland, and Sweden identified, as main policy barriers, the lack of equal regulations for the whole country (due mainly to decentralized states), and other countries also mention the lack of coordination within the health system:
“Differences in Regional Laws about the features and development of regional palliative care networks. The recent national law N.38/2010 tries to reduce these differences, but a lot of work has to be done. The Italian Constitution establishes that each region can organise autonomously its regional health service” (Italy, there are similar quotations in four more countries, Belgium, Finland, Sweden, and Switzerland).
Other frequently reported barriers were the lack of I-PC for noncancer patients, problems associated with funding and reimbursement, and the lack of the inclusion of PC into the regulatory framework. For instance, Belarus mentions that PC is not included in the Public Health Code.
Implementation of PC services
The lack of coordination and continuity of care at user and provider levels is a main barrier. The lack of coordination among providers was stated by Andorra, Azerbaijan, Germany, the Netherlands, Latvia, Lithuania, Malta, Poland, and Russia. In the continuity of care, many aspects are involved: lack of integration with primary care, lack of development of PC services in university hospitals, and absence of a clear definition of the specialist level of care:
“There is no consensus about general and specialist palliative care: what are the boundaries, how do they collaborate and build up on each other, etc.?” (Germany).
“Primary care givers are not sufficiently supported by palliative care specialists (no. 24/7 access to palliative care)” (Netherlands).
In this analysis, the lack of trained manpower has been classified as a barrier within the domain of services but could also refer to educational barriers. In any case, it is an important barrier and was mentioned in Iceland and Belarus:
“The lack of specialized and interested doctors is painful” (Iceland).
For contrast, Belgium referred the global shortness of formal caregivers, more especially in the nursing homes, as one of the three main barriers for the I-PC.
Availability of medicines
In two countries, the lack of opioid availability is identified as a barrier for the I-PC. In Albania, prescription of opioids is only available for cancer patients; and in Serbia, NGOs are not involved in the advocacy for changes in legislation. That does not mean that opioid availability is not a problem in Europe, as availability is an issue in countries such as Belarus, Kyrgyzstan, or Russia, but the analysis clarified that it must be classified as barrier for the G-PC and not as a barrier for I-PC.
Opportunities to I-PC across Europe
Categories and examples of opportunities to I-PC, classified by the WHO public health framework for PC, are shown in Table 2. Of a total of 133 opportunities mentioned by national associations from 48 countries, 65 (49%) referred specifically to issues of I-PC. Categories and subcategories with frequencies of opportunities identified are shown in Table 2. Related to education, there were 24 opportunities mentioned, 21 with policies, and 17 with the implementation of services. Three additional opportunities for the integration have been identified in the area of PC research.
WHO, World Health Organization.
Education
European PC leaders observe relevant key opportunities for future development within the field of education. They referred to the expansion of basic training and the inclusion of PC in the university, within professorships (Germany), and in the curricula:
“Introduction of academic teaching of palliative medicine (undergraduate and postgraduate) in other schools of medicine (it is already taught at Tel Aviv University)” (Israel, and see also similar quotations for Austria and France)
Training PC experts and establishing an official certification or accreditation for PC are also seen as major opportunities for the integration.
“Training opportunities for doctors and nurses are increasing (and improving in quality)” (Finland).
Policies
Opportunities are also highlighted in the field of policies. Foreseeable upcoming legislative changes, such as the passing of new laws on PC, or the inclusion of PC within the Public Health regulatory framework, were the most repeated opportunities (10 countries):
“The new norm that places an obligation on hospitals to provide hospital palliative care support teams” (Portugal)
The setting of national PC programs or strategies in Austria, Andorra, or Turkey and the integration in noncancer patients are also reported as advances. The reform of the health system is also seen as an opportunity in Ireland:
“The Government's commitment to radical reform of the health service offers an opportunity for the strategic positioning of palliative care to deliver a patient-centred, high-quality and effective service that is excellent value for money” (Ireland).
Implementation of PC services
Several countries report key opportunities concerning the implementation of services in varied situations such as home care (Netherlands, Serbia, Poland, or Italy) and nursing homes (Austria), an early integration into the disease's trajectory (The Netherlands) and in the continuity of care (the United Kingdom), implementation of guidelines and protocols (Romania, Lithuania, and Sweden), and expansion to including patients suffering from diseases other than cancer (Malta).
Research
Research was mentioned as an opportunity to develop PC in countries such as Belgium, Iceland, and the United Kingdom.
“There are more evidence-based practice in hospice and palliative care” (the United Kingdom)
The challenge of integrating PC in Europe and its relationship with levels of service provision
The quantitative analysis of the type of barriers mentioned by European PC leaders is presented in Tables 3 and 4.
The association between level of service provision and phase of development attending to the barriers is close to statistical significance (p = 0.056).
There is a statistically significant association between the level of service provision and phase of development attending to the opportunities (p = 0.001).
G-PC, development of general PC.
No statistically significant association was found between level of service provision and public health dimensions neither for barriers nor for opportunities (p = 0.119 and p = 0.061).
Table 3 shows that with greater provision of services in a country, the more frequently its difficulties and opportunities are related to integration. That is, in countries with “very high” or “high” provision of services, barriers directly related to the I-PC represent 49% and 33% of all barriers mentioned, respectively, while in countries with “intermediate” and “low” provision, only 19% and 26% were related to integrated care, respectively. This association is close to statistical significance (p = 0.056). Furthermore, the most frequent opportunities for integration are mentioned for countries with higher provision levels (“very high” 74%, “high” 57%) versus those with “intermediate” or “low” levels (36% and 28%, respectively). This association is statistically significant (p = 0.001).
Table 4 presents the frequency of different public health dimensions in the barriers to integration according to the different provision of PC services in European countries. Barriers to integration related to the dimension of education are the most frequent in countries with “intermediate” and “low” levels of service provision (57% and 44%, respectively); health policy barriers to integration are more important in countries with “intermediate” or “high” levels of service provision (29% and 50%, respectively) and much less relevant at “very high” or “low” levels (18% and 11%). In countries with the highest level of provision, the most frequent barriers are the implementation of health services (41%) and other education-related barriers (41%).
Also, Table 4 shows a similar analysis of the type of opportunities. In countries where the level of services is “low” or “intermediate,” opportunities related to education are the most frequent (56% and 69%, respectively). Opportunities for integration related to health policies are found at all levels of service provision. In countries with “very high” levels of service provision, opportunities related to the dimension of implementation are the most frequent (38%), and there appears a new dimension related to research in the field of PC. No statistical association was found between the level of service provision and the WHO dimensions, neither in barriers nor in opportunities.
Discussion
From the national PC leaders' perspectives, one in every three major barriers to PC development is related to the lack of integration within the health system. Their responses indicate that it is also time to integrate PC, as when they prioritize opportunities for PC development, half of them were specifically related to integration. Our analysis on service provision levels points out that this previous consideration is true in all stages of development: PC cannot be developed without achieving integration; for sustainable development, existing barriers must be overcome before or at the same time as first services are established. However, issues related to integration are more common in countries with high levels of service provision but are also present in other levels. This has been clear in the quantitative analysis where it is observed that 50% of the barriers and 75% of the opportunities in countries with a “very high” level of provision of PC services, such as the United Kingdom, Ireland, Belgium, Sweden, Netherlands, Austria, or Poland, are related with the integration.
The model for the development of PC, within the context of public health proposed in 2007 by the WHO, 9 remains valid many years afterward. Nearly all barriers and opportunities identified by PC national leaders in Europe can be categorized under the categories of the WHO proposal. Opportunities in research are new aspects to be considered when speaking about I-PC. In a potential revision of the WHO model, some subcategories could be included, renamed, or better specified within the current dimensions. This is the case for issues such as the regional equity in health policies regarding PC, the need for coordination among levels of care, and the inclusion of a specialization program for professionals.
Main barriers have been identified within the different dimensions of the WHO public health model. In education, the lack of basic training in PC at all levels has been identified as a core barrier. A novelty, when compared to previous analysis, is that at least eight countries mention training in PC at the undergraduate level as either a barrier or an opportunity for guaranteeing this basic education for future professionals. In other countries, it is already a reality: in a study about university education and PC in Europe, in 2013, PC was already taught as a mandatory subject in six countries' medical schools (the United Kingdom, Israel, Norway, Belgium, France, and Germany). In another seven countries, optional courses of PC were offered in each of the medical schools. 26 Another relevant issue within the education domain is that many countries express difficulties or hopes in having a specialization process for PC.
It seems that PC education would facilitate the integration at all development stages. The fact is that at any level of service provision, education-related issues are recurrent either as barriers or opportunities. Nevertheless, we observe in the frequency analysis that the critical moment for emphasizing education is when some services are already in place and the level of service provision can be considered “intermediate.” These are the educational issues highlighted by intermediate provision countries such as Finland, Portugal, Romania, or Israel, mentioning them as main barriers (57%) or as opportunities for greater integration (69%).
One-third of listed opportunities to the I-PC fall under the policiy dimension, and the analysis identifies that this is mainly about developing national plans or strategies for PC or legislative and regulatory advances for the I-PC in general health laws, or even in specific PC laws. The I-PC depends, to a great extent, on the development of adequate health policies, which means that service development is not in isolation or does not simply bypass the health system. The impression derived from our analysis is that national PC leaders interpret that health policies have been put in place, and that these policies represent a true chance for PC reaching all those in need in the future. It is possible that within the coming years, we will see greater advances in Europe as a result of efforts made by global institutions such as the WHO,10,27 or the European Parliament,5,28,29 and organizations such as EAPC. 30 Undoubtedly, some of the health policies in a country are determined by the “contagion” effect of what surrounding countries are developing in their health policies.
With regard to the development of services, and based on data gathered from the leaders, it can be deduced that the I-PC services has to do with matters of an adequate coordination of services at the diverse levels of care rather than with funding or the availability of material resources. These are the type of barriers within the domain of “implementation of services” that have been identified.
Finally, with regard to the public health dimensions, this analysis does not deny that still today barriers in the availability of medications exist. They have been reported less frequently as main barriers to integration (only two countries), and are also seldom reported as barriers to the G-PC (four countries, not presented in results). We cannot state that barriers in this sense do not exist, as other analyses have pointed it out, 13 but that the leaders' prioritization of these are less important to the development of PC in European countries than other identified issues.
For the first time, an analysis on barriers and opportunities for PC development is done considering different levels of service provision. No statistically significant association was found between levels of service provision and Public Health dimensions. Many factors could interfere with the development of services, including bureaucracy (laws may be enacted but not implemented) and lack of resources (trained personnel and places for care provision). However, according to our quantitative and qualitative analysis, for those countries with lower service provision levels, some recommendations could be taken into account. The first need is to pay attention to the education of PC, specifically training experts, and including the development of specialization programs. In the medium term, the focus should be on training future professionals at the undergraduate level. Opportunities are observed when laws and national PC plans are established and approved. For countries with higher levels of service provision, however, integration efforts must focus at the service level, promoting coordination and the establishment of strategic plans. Regarding policies, equity aspects of PC policies within the country and the expansion of PC for noncancer patients are issues on integration. Opportunities are seen in regulatory frameworks, research, and the inclusion of the PC components in the university.
Strengths and limitations
Our findings should not be interpreted as a comprehensive description of all the challenges and opportunities that characterize PC development. The open-ended survey questions favored diverse, context-specific responses, but this methodology also led to a limited number of responses for any given issue, which complicated the interpretation.
Expert surveys on PC development have limitations that have been described elsewhere. 31 The risk of bias of the informant's personal perspective has been addressed, as explained in the method, by directing the study to national associations expressly requiring that they nominate their expert or a committee to answer our questions. So, the priorities reported in our study mainly reflect the perspectives held by PC leaders, in a limited number per country, which may explain some of the emphasis placed on education and policy. Although this group constitutes the backbone of national PC development, its priorities may differ from those of patients, families, policymakers, and multidisciplinary professionals. Thus, our results constitute a sample of major priorities for PC development, but they, in no way, preclude the presence of other challenges, including, among others, opioid availability and use,32,33 the identification of patients in need of PC, 34 and the I-PC in cancer. 35
The data are from the 2013 EAPC Atlas, so the identified challenges and opportunities reflect what was true then and not necessarily what is true now. Things may or may not be different. Despite this, the 2013 EAPC Atlas dataset analyzed here is a unique European-wide and carefully built set that gives insights into important barriers and opportunities for PC integration.
Conclusion
Based on the feedback of leaders of national associations, I-PC seems achievable if professionals and students are trained in PC, and if they have access to well-established PC certification programs. The expansion of business plans, resources, and infrastructures, as well as widening the regulatory framework, would improve the I-PC into the healthcare system and must be perceived as true opportunities by policy makers.
While the diversity of country responses underlines the importance of adapting policies to the national context, many factors conditioning PC development were long term and, therefore, amenable to long-term planning that could help speed up the policy changes needed to improve access to PC in Europe.
While the challenges of improving access to PC are immense, there is a growing interest in understanding how best to implement an integrated care model. 36 A set of barriers and opportunities to PC integration has been identified across Europe, by national associations, offering a barometer against which to check the integration challenge across countries.
Footnotes
Acknowledgments
On behalf of the InSup-C project on patient-centered integrated PC. An EU Framework 7 Programme (FP7/2007–2013, Grant agreement no. 305555). 18 InSup-C aims to identify the prerequisites for best practice in integrated PC with the overall objective of improving service delivery and service user issues. InSup-C is coordinated by Dr. Jeroen Hasselaar, BSc, PhD, of Radboud University Medical Center, Nijmegen, The Netherlands. Other partners are as follows: University Hospital, Bonn, Germany; International Observatory on End-of-Life Care, Lancaster University, Lancaster, United Kingdom; University of Pecs Medical School, Pecs, Hungary; University Hospital Leuven, Leuven, Belgium; WHO, Geneva, Switzerland; European Association for Palliative Care (EAPC OnLus), Milan, Italy; Erasmus University, Rotterdam, The Netherlands; University of Navarra, Navarra, Spain; Mount Sinai Hospital, NY.
The authors thank all those associations, institutions, and professionals who have helped with the EAPC Atlas study. Without their selfless contribution and hard work, this study would not have been possible. A group of professionals have contributed either on their own behalf or on behalf of national PC institutions that can be found in: ![]()
Author Disclosure Statement
No competing financial interests exist.