
Abstract
Abstract
Objectives:
The dual aim of this study is, first, to describe preferred place of care (PPOC) and preferred place of death (PPOD) in terminally ill patients with lung and heart diseases compared with cancer patients and second, to describe differences in level of anxiety among patients with these diagnoses.
Background:
Previous research on end-of-life preferences focuses on cancer patients, most of whom identify home as their PPOC and PPOD. These preferences may, however, not mirror those of patients suffering from nonmalignant fatal diseases.
Design:
The study was designed as a cross-sectional study.
Setting:
Eligible patients from the recruiting departments filled in questionnaires regarding sociodemographics, PPOC and PPOD, and level of anxiety.
Results:
Of the 354 eligible patients, 167 patients agreed to participate in the study. Regardless of their diagnosis, most patients wished to be cared for and to die at home. Patients with cancer and heart diseases chose hospice as their second most common preference for both PPOC and PPOD, whereas patients with lung diseases chose nursing home and hospice equally frequent as their second most common preference. Regardless of their diagnosis, all patients had a higher level of anxiety than the average Danish population; patients with heart diseases had a much higher level of anxiety than patients with lung diseases and cancer.
Conclusion:
Patient preferences for PPOC and PPOD vary according to their diagnoses; tailoring palliative needs to patients' preferences is important regardless of their diagnosis.
Introduction
K
The dual aim of this study was, first, to describe PPOC and PPOD among patients who were terminally ill with lung and heart diseases and compare their preferences with those stated by cancer patients and second, to describe differences in the level of anxiety among patients with these three diagnoses.
Methods
This study is part of a larger randomized intervention study testing potential effects of advance care planning in which participating terminal ill patients with lung, heart, and cancer diseases were asked about PPOC and PPOD, anxiety, and sociodemographic factors before the intervention.
Setting
The Danish healthcare system is financed by income tax, and medical treatment is therefore available to everyone free of charge. The primary healthcare sector is available to everyone and includes treatments from general practitioners and home care nurses. The secondary sector consists of the acute wards where patients can be hospitalized at all times of the day and the specialized departments are responsible for the treatment of the patients' primary diseases. There is an ongoing registration of all healthcare utilization in central registers.
Study design
Eligible patients from the departments of oncology, respiratory medicine, and cardiology at the Aarhus University Hospital, Denmark, and the department of cardiology at Vejle Hospital, Denmark, were identified and recruited by doctors and nurses in these departments. Eligible patients with an estimated remaining lifespan of 12 months or less were assessed by the staff using a set of general and disease-specific inclusion criteria (Table 1). These criteria were based on a thorough literature review and collaboration with experts at the recruiting departments. The patients were contacted by mail and later by telephone by the first author. A baseline questionnaire, including written consent, a scale measuring anxiety, and ad hoc questions regarding sociodemographic factors, was then sent to the patient. Returning a consent form blank or not responding after two reminders was considered a decline.
Medical Research Councils scale, breathlessness scale. 30
Forced expiratory volume in one second.
Gender, age, physiology, index for idiopathic pulmonary fibrosis. 31
NYHA, New York Heart Association; GI, gastrointestinal.
The inclusion of patients began November 2013 and ended June 2015. For consenting patients, data from registers were afterward obtained.
Data collection
Data comprised questionnaire answers provided by the patient and registry data.
Questionnaire data
Previously used questions regarding PPOC and PPOD were used. 3 Patients were asked the following questions: “Have you considered, where would you prefer to spend the last months or weeks of your life”, and “Where would you prefer to die? 3 Response options were yes/no”. If yes, the response options were as follows: “home, at relatives, sheltered home, nursing home, hospital, hospice, other location, and don't know.” Questions used to assess preferences were carefully chosen and piloted in a previous study. 3 All patients filled in a questionnaire where symptoms of anxiety were measured on a subscale of the Symptom Checklist 92 item version (SCL-92), which includes eight subscales in total. The anxiety subscale contains 10 items. For each item, response options were scored on a five-point rating scale ranging from 0 (“not at all”) to 4 (“extremely”). 11
Register data
Data on diagnoses were collected through The National Patient Registry, which is administered by Statens Serum Institute. 12 This institution is responsible for several health registries used for central and local government tasks and research. Data from the questionnaires and The National Patient Registry were linked at an individual level using the unique Danish personal identification number (civil register number), a 10-digit code assigned to all Danish citizens. 13
Analysis
All variables, except levels of anxiety, were reported using percentage with a mean value and 95% confidence intervals. Categorical data were assessed using chi-square (χ2) test. Continuous variables were graphically assessed for normality and compared, except levels of anxiety, using Wilcoxon rank-sum test. The significance level was defined as p ≤ 0.05. In accordance with previous studies, the scores in the SCL-92 were summed up, and a mean score was derived for each symptom scale. 11 The SCL-92 is a rating scale and therefore belongs to the category of ordinal data. Data should therefore be reported as for example, medians and in quantiles. However, to be able to compare our data with the existing international literature and the Danish reference standards where mean values are used, we report data as means according to the Danish scoring manual.11,14 Differences in means of SCL-92 were analyzed using two-way analysis of variance (ANOVA) with department and gender as factors. Model validation was performed by inspecting residuals and fitted values. Some deviation from normality was observed due to right skewness and zero observations; however, comparing to a two-part analysis gave similar estimates and did not give cause to change any conclusions. Therefore, the ANOVA results are reported throughout. 15 Full details on the contents and the construction of the SCL-92, including its validation by item response models, have been published elsewhere.14,16 To confirm the internal consistency of the anxiety subscale of the SCL-92, a Mokken analysis was performed to investigate the scalability. The scalability is measured by Loevinger's coefficient of homogeneity ranging weak (0.30–0.39), acceptable (0.40–0.49), and strong (0.50 or higher).11,14,17 The Mokken analysis was performed using the Managing Successful Programme. 18 The other statistical analyses were carried out using Stata version 13.
Results
Of the 354 eligible patients, 167 patients agreed to participate (Fig. 1). Participants and nonparticipants were similar regarding gender (Table 2). However, nonparticipants were significantly older with an average difference of two years. The characteristics of participants regarding distribution of diagnoses are presented in Table 3.
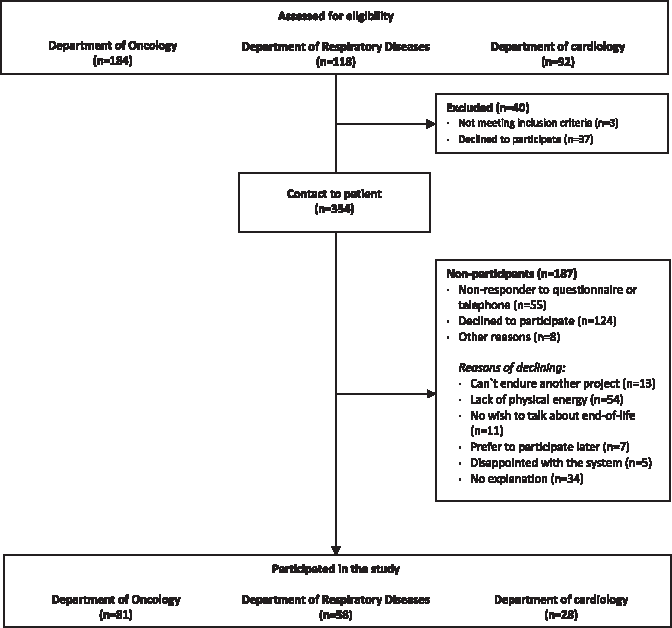
In total, 394 patients were assessed for eligibility at the three departments.
Chi-square (χ2) test.
Wilcoxon rank-sum test.
CI, confidence interval.
Sociodemographics
Participants in the three disease groups were similar on most parameters, apart from gender, age, children living at home, and status of residence (Table 4). First, with regard to gender, all three groups were significantly different from each other. The proportion of women was significantly higher among cancer patients than among patients with heart diseases. Second, cancer patients were significantly younger than patients with lung and heart diseases who had roughly the same age. Third, more cancer patients than patients with lung diseases had children living at home. Fourth, we found significantly fewer patients with lung diseases than patients with heart diseases who were living in their own homes. Although no significant difference was found, a trend was observed toward patients with lung diseases being more likely to be living alone, being single or divorced, and having a lower level of education than patients with the other diagnoses.
Chi-square (χ2) test.
Wilcoxon rank-sum test.
GCSE, General Certificate of Secondary Education.
PPOC and PPOD
Of the 167 participants, 137 patients had considerations concerning PPOC and 133 had considerations about PPOD (Table 5). Significantly more cancer patients than heart disease patients had considerations regarding PPOC. Among cancer patients, more than half favored home as their PPOC and, similar, slightly less than half of the patients preferred home as their PPOD. A significant difference was found between patients with cancer and patients with lung diseases; hence among the latter, fewer preferred hospice as their PPOC and PPOD and more favored hospital or nursing home (long stay) as their PPOC and PPOD.
Chi-square (χ2) test.
PPOD, preferred place of death; PPOC, preferred place of care.
Level of anxiety
A total of 152 patients completed the subscale of anxiety (Table 6). The Loevinger's coefficient of homogeneity is 0.48, which is acceptable. The median score was 0.5 with an interquartile range at 0.7. Five patients reported a sum score above the expected maximum sum score of 1.9 and were classified as outliers. Data were compared with the Danish reference standard, which is a mean score of the general Danish population (Table 6). The levels of anxiety were above the Danish reference standard in all disease groups showing a higher level of anxiety than a representative sample of the Danish population. Patients with heart diseases had a significantly higher level of anxiety than patients with lung diseases and cancer. This was most pronounced among female patients with heart diseases than female patients with cancer. Overall, patients with cancer had a lower sum score than patients with lung and heart diseases.
The maximum sum score was 3.2 and the minimum was 0. The 75th percentile was 0.9 and the 25th percentile was 0.2.
Rating scales for affektive lidelser, Psykiatrisk Forskningsenhed, Psykiatrisk Sygehus Hillerød Frederiksborg Amt, 2005.
Analysis of variance, two way.
Discussion
Main findings
Regardless of their diagnosis, most patients had considered both PPOC and PPOD. However, while most patients with cancer had considered their PPOC and PPOD, this was rarer among patients with heart diseases. Regardless of their diagnosis, most patients wished to be cared for and die at home. Patients with cancer and heart diseases chose hospice as their second most common preference for both PPOC and PPOD, whereas patients with lung diseases chose nursing home and hospice equally frequent as their second most common preference. Although all patients had a higher level of anxiety than the average Danish population, regardless of their diagnosis, differences among diagnoses were found; patients with heart diseases had a much higher level of anxiety than patients with lung diseases and cancer.
Strengths and weaknesses of the study
The strength of this study is the use of patients' own statements about their preferences regarding PPOC and PPOD rather than proxy statements by, for example, the bereaved relatives. We also consider it as a strength that all patients were asked the same questions, regardless of their diagnosis, and we used a validated questionnaire for measuring anxiety. However, our study also has a number of limitations, and the results must therefore be interpreted with caution. Because of the risk of selection bias, it is possible that some of the more severely symptomatic patients were not invited into the study by the recruiting staff as such an invitation could pose an unwelcome burden for those patients. Not all eligible patients accepted participation, and those who declined were on average two years older than the participants. The declining patients may therefore have higher morbidity and mortality and thus presumably have other preferences than the participants. It may therefore be argued that the study population may have had fewer symptoms from their disease and thereby better life conditions than a representative group of terminally ill patients. Finally, it should be noted that there were relatively fewer patients with heart diseases than patients with cancer and lung diseases, which also troubles the generalizability.
Comparison with existing literature
The percentage of patients who had considered PPOC and PPOD was lowest among patients with heart disease in this study. This may reflect that health professionals do not engage in discussions of end-of-life care with patients with nonmalignant diseases, who therefore receive little or no professional support to cope with symptoms and imminent death despite the fact that they are facing a similar or even worse symptom burden and deterioration of their quality of life than patients with a malignant disease.19,20 This study also reveals differences among patients' preferences for PPOC and PPOD, showing that patients with lung diseases were more likely to choose nursing home and hospital than patients with cancer and heart diseases. This can be explained by several factors. First, patients with lung diseases may be forced to prefer care outside the home as this group of patients are more likely to be living alone without relatives to support them. Second, the number of patients with lung diseases preferring hospice may be low because these patients receive little information about end-of-life care. Third, the general perception among the public may be that hospice care is earmarked for patients with cancer. Finally, it should be noted that many patients with terminal lung diseases, as part of the nature of the nonmalignant illness trajectory, experience anxiety-provoking exacerbations, for example, severe dyspnea, which may leave them in fear of not having access to the medical expertise at hospitals. 21
Most patients experience anxiety throughout their illness trajectory regardless of their diagnosis. 22 In terminally ill cancer patients, anxiety negatively affects patients' quality of life. 23 Anxiety is also outspoken in patients who are admitted and readmitted to the hospital following an acute exacerbation of chronic obstructive pulmonary diseases and cardiovascular diseases.24,25 To our knowledge, only one study has investigated levels of anxiety among terminally ill patients. 26 This study found a slightly higher level of anxiety among patients with chronic obstructive pulmonary diseases and chronic heart failure than among patients with cancer. 26 Our results reveal clear differences; hence, cancer patients had far lower levels of anxiety than patients with heart and lung diseases. Still, our results remain in accordance with previous research showing that health professionals in oncological settings are more aware of patients' palliative needs and better at initiating end-of-life discussions, which may lower the level of anxiety in cancer patients. 27 Another possible explanation for the lower level of anxiety among cancer patients in our study could be that the cancer patients were younger and more likely to have more relatives than patients with heart and lung diseases. Relatives can be a valuable source of support and help for patients, which may lower their level of anxiety. 28
Implications and further research
Since PPOC and PPOD are influenced by several factors such as optimal symptom management, it is pivotal that professionals inform and guide patients as their illness progresses. 29
This study reveals much diversity among patients with terminal diseases and emphasizes that healthcare professionals should be aware of patients' palliative needs, regardless of their diagnosis. The high level of anxiety in patients with nonmalignancies calls for a stronger focus on these patients' palliative needs. Future research should focus on how palliative care can be adjusted to different patient groups with different needs and wishes at the end of life.
In conclusion, our study demonstrates marked differences among terminally ill patients with lung diseases, heart diseases, and cancer regarding their preferences for place of care and place of death, and differences in levels of anxiety. The study highlights the need for paying attention to patients' palliative needs, regardless of their diagnosis.
Ethical Approval
The study was conducted in accordance with Danish legislation on ethical standards for studies that are not classified as a biomedical intervention: according to the Scientific Ethics Committee for the Central Denmark Region, this study does not need the approval of the Scientific Ethics Committee (j. no. 35/2013). The study was approved by the Danish Data Protection Agency (j. no. 1-16-02-367-14) and is listed in ClinicalTrials.gov.
Footnotes
Acknowledgments
Danish Cancer Society and the Danish foundation TrygFonden supported the work through the joint grant “Safety in Palliative Care” [Tryghed i palliative forløb]. Profound gratitude is extended to participating patients, relatives, and the staff at the recruiting departments. The authors also express their appreciation to data manager Hanne Beyer, Research Unit for General Practice, Aarhus University, Denmark. Furthermore, gratitude is extended to nurse Linda Sigaard, department of Respiratory Medicine, Aarhus University Hospital, Denmark, and to nurse Lene Vahle, department of oncology, Aarhus University Hospital, Denmark, for their dedicated assistance to the recruitment of patients. Finally, gratitude is expressed to Morten Pilegaard, department of business communication, Aarhus University, Denmark, for linguistic support.
Funding
Funding sources had no role in the design, conduct, and analysis of this study or in the decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.